

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary ventricular fibrillation (PVF) during acute myocardial infarction (AMI) refers to VF that occurs early (usually < 48 hr post myocardial infarction), and is not associated with recurrent ischemia or heart failure (1). The incidence of VF was reported to be more than 10% during AMI, and VF usually occurs in a few hours after the onset of chest pain (1). VF is the most frequent cause of death in association with AMI because it usually occurs before medical contact (1). Recent studies have demonstrated that J wave on the sECG has been associated with idiopathic VF in patients who do not have structural heart disease (2). A recent study also reported that the presence of J wave is associated with ventricular arrhythmia in patients who have chronic coronary artery disease (3). So far, few studies reported that the presence of J wave in sECG is associated with VF during AMI (1, 4, 5, 6). Several variables, including J wave, were reported as significant predictors of VF, but failed to get statistical significance. Through this study, we planned to evaluate that the presence of J wave on the sECG could be a potential risk factor for VF during AMI.
MATERIALS AND METHODS
Patient selection and data collection
We performed a retrospective study of 317 patients diagnosed with AMI in a single center from 2009 to 2012. Among the involved 317 patients, especially in the VF group, 21 patients who did not have a sECG before AMI were excluded in this group. As a result, 22 patients were selected as the VF group and 296 patients were enrolled for data analysis. Finally, all patients were classified as having a VF or not (VF group: n = 22 [13.5%], the non-VF group : n = 274 [86.5%]). Furthermore, all patients selected for this study received coronary angiography and underwent percutaneous coronary interventions (PCIs). We performed a subgroup analysis according to the location of the infarction, and the infarct-related artery (IRA) were left anterior descending (LAD) artery (45.4%), left circumflex (LCX) artery (6.1%), right coronary artery (RCA) (48.5%), diagonal branch (0.3%) and left main artery (1.0%), respectively. We also checked a pre-PCI Thrombolysis In Myocardial Infarction (TIMI) flow grade before the coronary intervention.
ECG analysis
The latest ECG before AMI was reviewed for J wave characteristics. Twelve-lead ECGs were digitally downloaded from the GE Marquette MUSE system (GE Medical Systems, Milwaukee, WI, USA) and were also analyzed digitally (Adobe Acrobat X Professional; Adobe Systems Incorporated, San Jose, CA, USA). Three investigators performed ECG analysis separately and randomly to confirm correct J wave patterns. The early repolarization on the sECG was defined as J point elevations manifested through QRS notching or slurring for at least 1 mm (0.1 mV) above the baseline in at least two consecutive inferior or lateral leads. As defined through prior studies, QRS notching in ECG was defined as a positive deflection at the terminal portion of a positive QRS complex. QRS slurring in ECG was defined as a smooth transition from the QRS complex to the ST segment with upright concavity. We excluded ECGs of Brugada pattern which have J wave in anterior precordial leads (V1-V3). We measured the amplitude of J wave at the peak of the positive deflection in case of notched pattern and at the QRS-ST junction in slurred pattern.
Statistics
Statistical analyses were performed with SPSS statistical software (version 12.K; SPSS, Inc., Chicago, IL, USA). Continuous variables were expressed as mean±SD and were compared by t tests. Categorical variables were expressed as percentages and were compared by chi-square statistics or Fisher's exact test as indicated. A multiple logistic regression analysis was used to identify the subset of variables as predictors of VF during AMI. Analyses were considered significant at a P value<0.05 (2-tailed).
RESULTS
Demographic and clinical characteristics of all AMI patients
Table 1 shows baseline characteristics of the study population. Among the total 22 patients of the VF group, 16 patients were males and 6 patients were females. The mean age of the VF group was a 59.95±12.94 yr. The non-VF group consisted of 274 patients and male was also predominant in numbers which were 207. The mean age of the non-VF group was 61.33±13.47 and was not statistically different from that of the VF group (P=0.644). VF occurred before ER arrival in 9 patients, during ER stay before PCI in 5 patients, during PCI in 1 patient, and within 48 hr after PCI in 7 patients. In this study, we excluded patients with VF after 48 hr from the onset of chest pain. The mean time gap from acquisition of the latest ECGs to occurrence of VF was 266 days in the VF group. In this group, the distributions of time gap were over 1 yr in 5 patients, between 1 month and 1 yr in 13 patients, and within 1 month in 4 patients. There was no statistical difference in the locations of IRA, or TIMI flow before PCI between the two groups. Also, there was no statistical difference in the numbers of stenosed coronary arteries and echocardiographic parameters, including ejection fractions of left ventricle and diameters of left atrium. Cardiac deaths were noted both in the VF group (n=1, 4.5%) vs in the non-VF group (n=1, 0.4%), which were not different statistically (P=0.150).
Fig. 1 shows baseline ECGs in AMI patients. Fig. 1A and Fig. 1B show notched J wave (arrows) in inferior (Fig. 1A) and lateral (Fig. 1B) leads in patients who had an event of VF, whereas Fig. 1C and D show no J wave in inferior (Fig. 1C) or lateral (Fig. 1D) leads in patients who showed no VF during AMI.
Predictors of VF during AMI
We found that several conventional risk factors of VF were significantly related to VF during AMI; a time delay from the onset of chest pain to the arrival to emergency room (ER) was significantly shorter in the VF group (634.6±135.3 min vs 1,815.6± 109.8 min; P=0.001, Table 1). Patients in the VF group had a larger IRA, in other words, a greater cardiac enzyme level. Hence, blood concentration of creatine phosphokinase (CK) was significantly higher in the VF group (12,429.78±2,650 IU/L vs 2,285.97±138.10 IU/L, P=0.001, Table 1). The incidence of ST-segment elevation was also higher in the VF group (n=21 [95.45%] vs n=172 [62.8], P=0.001, Table 1).
Among the 52 patients with J wave (13 in the VF group and 39 in the non-VF group) who received elicit PCIs, J wave persisted in 13 (100%) patients of the VF group and in 32 (82.0%) patients of the non-VF group during hospital stay. Lastly, the prevalence of VF was significantly higher in patients with J wave compared to the patients without J wave (n=13 [25%] vs n=9 [3.7%], odds ratio, 8.704, P<0.001).
Detailed Characteristics of J wave for Predicting VF
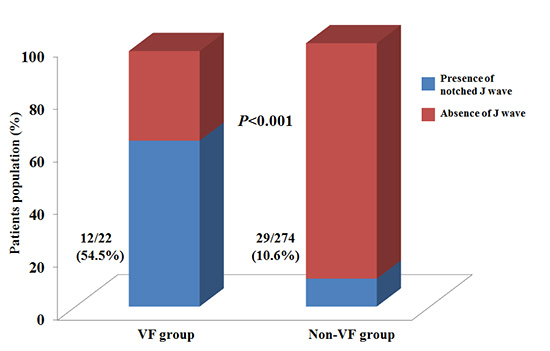
Table 2 and Fig. 2 show that the incidence of J wave, especially a notched pattern, on the sECG was significantly higher in the VF group than in the non-VF group (n=12 [54.5%] vs n=29 [10.6%]; P<0.001). Multivariate logistic regression analysis demonstrated that the presence of ST-segment elevation and the presence of J wave with notched pattern were significantly associated with the occurrence of VF during AMI (odds ratio, 15.250; P=0.019, odds ratio 16.547; P<0.001, respectively, Table 3). Additionally, the prevalences of J wave with notched pattern in inferior lead or J point elevation≥0.2 mV were significantly higher in the VF group than non-VF group (n=11 [50.0%] vs n=20 [7.2%], P<0.001; n=2 [9.0%] vs n=2 [0.7%], P=0.029; Table 4). The prevalence of J wave with notched pattern in inferior lead with J point elevation≥0.2 mV was also significantly higher in the VF group (n=2 [9.0%] vs n=1 [0.4%], P=0.015; Table 4).
Unfortunately, we could not document a fluctuation of J wave before AMI. Likewise, among the 13 patients with J wave in the VF group, we could not observe any fluctuation of J wave before VF.
DISCUSSION
Early repolarization pattern including J wave was considered benign and incidental finding, especially in young male individuals (7). Recent studies have demonstrated that J wave on the sECG is associated with idiopathic VF in patients who do not have structural heart disease (8, 9).
In several reports, many investigators have suggested that J wave on the sECG was created by the production of transmural voltage gradient between the endocardium and the epicardium during repolarization or depolarization because of a decrease in inward sodium or calcium channel currents or an increase in outward potassium currents mediated through the Ito, IK-ATP, and IK-Ach channels (7, 10). When the epicardial current is amplified disproportionately through the same ionic mechanism, J wave-mediated arrhythmia could be triggered. Also, when J wave is accentuated, which indicates an increase in the height of action potential notch in epicardium, action potential dome in epicardium can be lost. This loss of action potential dome could trigger phase-2 reentry and VF (11).
It has been reported that the high risk patients for VF in Brugada syndrome also have characteristic ECG findings and clinical outcomes with similar ionic and cellular mechanisms (12). Also, AMI itself exhibits a characteristic ST segment change. It has been reported that acute regional myocardial ischemia results in markedly heterogenous loss of Ito-mediated epicardial action potential domes across the ischemic border, leading to phase 2 reentry and VF similar to Brugada syndrome and J wave-mediated VF (13).
In this retrospective study, we found that the presence of notched J wave on the sECG is associated with the occurrence of VF during AMI. This study suggests that notched J wave may be a potential risk factor of VF during an acute stage of disease, such as AMI. In other words, the presence of notched J wave may play a role as a substrate for development of phase 2 reentry and eventually VF through a transmural dispersion during cardiac action potentials. Additionally, an episode of acute regional ischemia could accentuate transmural voltage gradient between endocardium and epicardium. Through these mechanisms, patients who have notched J wave on the sECG exhibit an increased incidence of VF during AMI.
In addition, this study also showed that patients in the VF group were likely to have notched J wave in inferior leads and J-point elevation≥0.2 mV. Different distribution of specific ion channels contributes to the different location of J wave on the sECG (10). In the present study, we found that the incidence of J wave in inferior lead was higher in the VF group. This result might be explained by greater distribution of the Ito channel, associated with VF, in the right ventricular epicardium than in the left ventricular epicardium (14). The result of this study related to the amplitude of J wave was similar to those of previous studies (15). Meanwhile, Rosso et al. demonstrated that a slurring pattern of the terminal portion of QRS complex has no prognostic value in predicting idiopathic VF (16). Additionally, Rudic et al. demonstrated that a notching pattern of terminal portion of the QRS complex was the predominant morphology associated with a risk of VF (5). Likewise, in the present study, we could not find a significant relationship between slurred J wave and VF. In conclusion, through the present study, we found that the distribution and the amplitude of the J wave in patients with VF during AMI were similar to those of the previous studies.
There are several proposed risk factors of VF during AMI (1, 17). In this study, we tried to control those risk factors, such as male gender, age, and infarct size (based on the cardiac enzyme level), systolic blood pressure, presence of diabetes mellitus, QTc interval on sECG, history of smoking and the time delay from the onset of chest pain to medical contact (1, 17). Several baseline characteristics were associated with increased risk of VF during AMI in this study. A time delay from the onset of chest pain was earlier in the VF group. This might indicate that the symptomatic VF makes patients to find medical contact earlier than patients of non-VF. Blood concentration of CK level was higher in the VF group. In other words, more severely damaged patients were selected in the VF group. Moreover, there is a greater tendency to present ST-segment elevation in the VF group. Despite adjusting these important differences during this analysis, we found a statistically significant association between notched J wave and VF during AMI.
Through this study, we demonstrated that notched J wave was an independent predictor of VF during AMI. Accordingly, identification of J wave on sECG before AMI may be helpful to distinguish patients who are susceptible to developing VF, especially in patients with J wave in inferior leads and with J wave of high amplitude. We could propose a careful monitoring and consideration of primary prevention of VF during AMI in those patients. Additionally, recent studies have suggested that specific genetic disorders may be responsible for the VF (18, 19). Hence, further studies will be needed to clarify the relationship between the genetic susceptibility and VF in patients with J wave on sECG.
There are several limitations to our study. First of all, the small sample size restricts statistical power and presented as broad confidence intervals. This may contribute to somewhat different result from prior studies regarding morphological patterns of J wave. Secondly, we could not exclude myocardial scar, which could have had an arrhythmogenic potential, because we could not perform studies such as stress testing or cardiac magnetic resonance imaging to rule out scar tissue objectively.
We demonstrated that J wave is an independent predictor of VF during AMI. Accordingly, an identification of J wave on sECG before AMI may be helpful to distinguish patients who are more likely to have an episode of VF. Prospective, randomized, large sample sized, and long-term follow-up studies are required to certify the presence of J waves as a risk factor of VF during AMI.



 XML Download
XML Download