

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is the most common chronic inflammatory disease of the airways and is a complex disorder entailing both environmental and genetic factors (1). Various studies have proposed several risk factors for the development of asthma in children, such as exposure to allergen, parental tobacco smoke, air pollution, and oxidative stress. In asthma, exposure to triggers has been associated with innate immune activation including increased expression of interleukin (IL)-8, IL-1β and major receptors, such as Toll-like receptor (TLR)2, and TLR4, leading to production of reactive oxygen species (ROS) (2, 3).
A recent worldwide study showed that exposure to acetaminophen in the intrauterine environment, infancy, childhood, and adult life as significantly increasing the risk of asthma that being so acetaminophen usage is one of the most convincing candidates for influencing asthma development in children (4, 5, 6, 7).
Acetaminophen is a potential source of oxidative stress (6, 8) and many studies have provided evidence indicating a rise in oxidative stress in asthma (9). Oxidative stress produced by ROS has been associated with airway inflammation, bronchial hyperresponsiveness (BHR) (10), and stimulation of inflammatory cells (11, 12, 13). Some studies have suggested that acetaminophen ingestion results in a decline in antioxidants (such as glutathione), and related this to the adverse effects observed in asthma (11, 14, 15). In addition, in our previous study, we demonstrated that ROS-related gene polymorphisms were significantly associated with the relationship between acetaminophen (paracetamol) use and asthma (16).
Polymorphisms in the TLR4 gene may play a role in the development of allergic airway inflammation (17). Several studies have indicated that specific polymorphisms at TLR4 (rs4986790 and rs1927911) were associated with asthma (18, 19, 20). In addition, it was previously suggested that the TLR4 polymorphisms, rs4986790 and rs4986791, are associated with an altered response to endotoxin, modifying the risk of asthma (17). In particular, a further study reported that the TLR4 polymorphism, rs1927911, is associated with the influence of increased exposure to fine particulate matter (PM2.5) levels in childhood doctor-diagnosed asthma (18).
Therefore, we investigated whether recent acetaminophen usage was associated with asthma or BHR and if there was an association between polymorphism at TLR4 (rs1927911) and asthma or BHR.
MATERIALS AND METHODS
Study participants
In this study, we recruited a total of 2,428 school children aged 8-13 yr from two cross-sectional surveys, in nine elementary schools of Seoul and Jeongeup cities in Korea (21). Children were ineligible to participate in the study if they suffered from a chronic or immune disease, or had used steroid or antihistamine medication in the 4 weeks before the test.
ISAAC questionnaire
Questions were taken from the International Study of Asthma and Allergies in Childhood (ISAAC). The written questionnaire was translated into Korean according to the ISAAC protocol. The questionnaire was used to determine the prevalence of symptoms and diagnosis of allergic diseases, demographic factors, and potential explanatory and confounding factors. Questionnaires were distributed and collected from July to October of 2008.
The questionnaire was composed of three main sections: 1) general characteristics including date of birth, sex, height, and weight; 2) a history of symptoms related to allergic disease, including asthma; 3) exposure to environmental factors associated with allergic disease. Parents completed the Korean version of the ISAAC questionnaire.
Prevalence of asthma was categorised as follows: "asthma diagnosis ever" (individuals who had been diagnosed with asthma in their lifetime) and "current asthma" (children included in the "asthma diagnosis ever" category who had experienced symptoms within the 12 months before completing the survey). Use of acetaminophen was defined as taking the medication for more than 3 days within the 12 months before the survey.
Measurement of bronchial hyperresponsiveness
The methacholine challenge test was executed using a dosimeter with a concentration range of 0.625-25 mg/mL. A spirometer (Microspiro HI298, Tokyo, Japan) was used to measure the forced expiratory volume in 1 second (FEV1) after each inhalation. Bronchial hyperresponsiveness (BHR) to methacholine was defined as a PC20 (the concentration of methacholine required to provoke a 20% reduction in FEV1)≤16 mg/mL.
Measurement of eosinophils and total IgE
The percentage of blood eosinophils was evaluated (Coulter Counter, STKS; Beckman Coulter, Fullerton, CA, USA). Serum total immunoglobulin E (IgE) was measured by fluorescent enzyme immunoassay using the ImmunoCAP system (Phadia AB, Uppsala, Sweden).
Genotyping
Genomic DNA was obtained from peripheral blood of the subjects using the Gentra Puregene Blood kit (Qiagen sciences, Germantown, MD, USA). Genotyping of the TLR4 polymorphism, rs1927911 was performed using a TaqMan assay (Assay ID, C_ 11722141_10; ABI, Foster City, CA, USA), according to the manufacturer's instructions. Endpoint readings were performed on an ABI PRISM 7900 HT Sequence Detection System (ABI).
Statistical analyses
Statistical analyses were performed using SPSS version 20.0 (SPSS, Inc., Chicago, IL, USA). Results are presented with 95% confidence intervals (95% CIs). Logistic regression analyses were performed to calculate adjusted odds ratios (aORs) for associations between asthma and independent risk factors. The interactions between TLR4 polymorphism and asthma were evaluated by multivariate logistic regression analysis. The effect of use of acetaminophen on the development of asthma in context of the polymorphic genotype at TLR4 was also determined. In multivariate analyses, adjustments were made for the study participants age, sex, and body mass index (BMI), parental asthma as a familial factor, and family income as socioeconomic factor, and environmental tobacco smoke (ETS) as an environmental factor. For all analyses, a P value<0.05 was regarded as statistically significant.
Ethics statement
Approval to conduct the study was obtained from the institutional review boards of Hallym University and University of Ulsan College of Medicine (IRB number: 2008-0208), and from the principals of the schools attended by the children. Written informed consent was obtained from the parents or guardians of all children.
RESULTS
Population characteristics and prevalence of asthma
The demographic data of the 2,428 children participating in this study are presented in Table 1. Their mean age was 10.31±1.61 yr. The proportion of males was 52.17%. A parental history of asthma was observed in 3.56% of the study population. Exposure to environmental tobacco smoking was indicated in 42.58% of children. The usage of acetaminophen was reported for 53.33% of the subjects. Asthma had been diagnosed by a doctor in 9.07% of the children. Positive BHR (PC20≤16) was present in 12.09% of the subjects.
Risk factors for asthma
Use of acetaminophen in the last 12 months was associated with risk of BHR (aOR, 1.47; 95% CI, 1.08-2.00, P=0.01), but was not significantly associated with either asthma diagnosis ever or current asthma (Table 2). Family history of asthma increased the risk of asthma diagnosis ever (aOR, 1.97; 95% CI, 1.01-3.86, P=0.05), current asthma (aOR, 2.87; 95% CI, 1.11-7.42, P=0.03), and BHR (aOR, 1.99; 95% CI, 1.04-3.78, P=0.04) (Table 2).
The frequencies of CC, CT, and TT of TLR4 polymorphism were 26.0%, 35.3%, and 12.1%, respectively. Analysis of association between the TLR4 polymorphism, rs1927911, and asthma indicated no association between the genotypes (CT+TT) and asthma diagnosis ever, current asthma, or BHR (Table 2) compared to the homozygous reference allele (CC genotype).
Association between acetaminophen use and family history of asthma
The use of acetaminophen, combined with family history of asthma, was significantly associated with asthma diagnosis ever and current asthma (aOR, 2.55; 95% CI, 1.09-6.00, P=0.03; aOR, 4.64; 95% CI, 1.48-14.56, P=0.01, respectively); however, neither use of acetaminophen in the absence of family history of asthma, nor lack of use of acetaminophen in the presence of family history of asthma were associated with asthma diagnosis ever or current asthma (Table 3). Our results also indicated that acetaminophen use, with or without family history of asthma, was associated with BHR (aOR, 2.63; 95% CI, 1.11-6.22, P=0.03; aOR, 1.49; 95% CI, 1.09-2.05, P=0.01, respectively). Although subjects who had a family history of asthma but had not used acetaminophen showed a tendency towards increased risk for BHR, this was not significant (aOR, 2.31; 95% CI, 0.87-6.15, P=0.09) (Table 3).
Combined effects of acetaminophen use and the TLR4 polymorphism, rs1927911
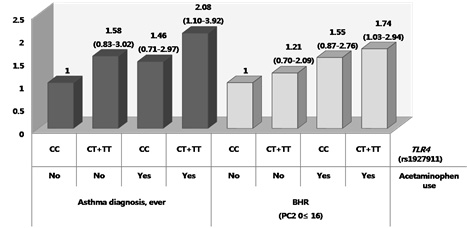
Analysis of association between use of acetaminophen and TLR4 polymorphism on asthma indicated that a combination of CT+TT genotype and acetaminophen use was significantly associated with asthma diagnosis ever (aOR, 2.08; 95% CI, 1.10-3.92, P=0.02), when compared to the CC genotype in the absence of acetaminophen use. Conversely, neither the CT+TT genotype in the absence of acetaminophen use, nor the CC genotype with acetaminophen were related to asthma diagnosis ever (Table 4). In addition, the CT+TT genotype in combination with acetaminophen usage was associated with BHR (aOR, 1.74; 95% CI, 1.03-2.94, P=0.04); whereas neither the CT+TT genotype without, nor the CC genotype with, acetaminophen usage were associated with BHR. No significant association was observed between TLR4 polymorphism and acetaminophen use for current asthma (Table 4).
DISCUSSION
In this study, we identified that acetaminophen use within the past 12 months was associated with asthma in children. The presence of a family history of asthma also increased the risk of asthma in children and this notably increased with use of acetaminophen. We analysed these risk factors in the context of TLR4 gene polymorphism to identify any associations with asthma. We found that acetaminophen use was associated with asthma and BHR in children with CT+TT genotypes at the TLR4 polymorphism, rs1927911. These findings suggest that the risk of asthma might be increased in susceptible subjects exposed to the acetaminophen use.
Previous epidemiologic studies have reported that usage of acetaminophen in the prenatal period, infancy, and childhood is associated with an increased risk of asthma in children (4, 7, 22, 23, 24). The ISAAC study reported that the use of acetaminophen in the first year of life was associated with an increased risk of asthma and that acetaminophen usage in the past 12 months was associated with an increased risk of asthma symptoms in children aged 6 to 7 yr (24). Furthermore, in a population-based case-control study in the United Kingdom, acetaminophen use was positively associated with asthma in subjects aged 16-49 yr (25), and a New Zealand study found that acetaminophen use in the past 12 months was related to an exposure-dependent increase in the risk of asthma symptoms in children aged 13 to 14 yr (4). These results are comparable to our findings that the use of acetaminophen within the previous 12 months in children was associated with an increased risk of asthma. Overall, these observations suggest that the risk for asthma in childhood is likely to be influenced by acetaminophen exposure within the past 12 months, as well as in early life.
Several potential mechanisms exist to explain the risk of asthma. One main mechanism is downregulation of the glutathione pathway, which can be triggered by acetaminophen. The depletion of reduced antioxidants, such as glutathione, can lead to a decrease in pulmonary antioxidant defences against ROS-mediated oxidative stress (26, 27). Such oxidative stress can damage important components of the airway epithelium and lead to cell destruction (6). Metabolism of acetaminophen can also lead to pulmonary toxicity as a result of reduced glutathione levels in the body (28). Another potential mechanism leading to asthma susceptibility is stimulation of the innate immune response through airway exposure to allergens, viruses, and air pollutants (29). Acetaminophen is often used to control fever that can be caused by such inflammation. Moreover, these reactions increase expression of innate immune receptors, such as TLR2, TLR4, and the pro-inflammatory cytokines, IL-8 and IL-1β (3), and lead to oxidative stress linked to the pathophysiology of asthma, which manifests as excessive production of ROS by activated eosinophils, neutrophils, and macrophages (9, 30). These pathways suggest mechanisms by which acetaminophen may be related to asthma and airway inflammation risk.
TLR4 is a typical pattern recognition receptor (31), recognising pathogen-associated molecular patterns (PAMPs) (32) and endogenous damage-associated molecular patterns (DAMPs) released mainly as a result of tissue injury (33, 34). Moreover, direct damage of airways, through ROS-induced inflammation is mediated via TLR4 signalling pathways (33). Under conditions of airway hyperreactivity invoking inflammatory responses, epithelial cells damaged by oxidative stress can release DAMPs, which activate TLR4 signalling pathways in airway macrophages, initiating inflammatory responses, such as upregulation of Tumor Necrosis Factor-α (TNF-α) in concert with IL-1β (34, 35). Furthermore, TLR4 polymorphisms may influence the balance between Th1 and Th2 responses, and hence susceptibility to allergic airway diseases (17). Therefore, in this study, we were interested in TLR4 gene and selected 2 polymorphisms, rs4986790 and rs1927911, known to be associated with asthma. The majority of previous studies have analysed the relationship between asthma and the TLR4 polymorphism, rs4986790. One study of Swedish children reported that rs4986790 was associated with a 4-fold higher prevalence of asthma (36); however, an Egyptian study reported no significant association of this marker with childhood asthma (37), and a further study the British showed no association of rs4986790 with asthma development (38). However, this polymorphism is not informative in some Asian populations. According to the HapMap database, the minor allele frequency of rs4986790 is zero among Japanese individuals. Similarly, in our study, the results of genotyping in 100 Korean children indicated lack of polymorphism at this locus (all children had the AA genotype; data not shown) and it was therefore not investigated further. The meta-analysis study reported an insignificant association between the TLR4 polymorphism (rs4986790) and asthma. However, this report suggested that a relevant environmental exposures, other genetic variants, race/ethnicity, age, and gender involving this polymorphism should be considered when studying a complex, heterogeneous disease such as asthma (39). Literature regarding the asthma-related TLR4 polymorphism, rs1927911, is not as abundant as that for rs4986790; however, rs1927911 had the greatest impact among several polymorphisms of TLR4 on risk of childhood asthma associated with exposure to fine particulates (PM2.5) (18). In this study, we found a significant association between rs1927911 and asthma or BHR in Korean children. We propose that rs1927911 may enhance the risk of asthma in response to acetaminophen exposure during childhood, and such an effect might be explained by changes in the inflammatory response caused by the TLR4 polymorphism.
Our study has some limitations. First, we investigated the relationship between acetaminophen use in the 12 months before the survey, not use of acetaminophen during infancy and diagnosis of asthma instead of recent symptoms of asthma aggravation (40). This has the possibility of reverse causation, as the use of acetaminophen is common after aggravation of asthma due to viral or bacterial infections in children. Also, we did not investigate the apparent causal connection whether this has an attack of asthma by actually acetaminophen use. It should be to carry out prospective and mechanism-related further studies. Second, this is a cross-sectional study, which prevented us from testing for a causal relationship. Third, our study did not demonstrate mechanisms connected with oxidative stress. We analysed the relationship between asthma and ROS-related-polymorphisms (rs1695 and rs1800566) of glutathione S-transferase pi 1 (GSTP1) and NAD(P)H dehydrogenase, quinone 1 (NQO1), respectively; however, these were not associated with the effects of recent acetaminophen use on asthma and BHR in Korean children aged 8-13 yr (Supplementary Table 1, 2). Finally, we analysed only one SNP in the TLR4 gene and did not investigate its function.
Strengths of the study include the relatively large sample size and, the inclusion of BHR measurements from 2,428 children, providing more objective evidence for relationship between asthma and acetaminophen. In addition, while several studies have reported interactions between acetaminophen and ROS genes, this is the first to investigate whether the influence of acetaminophen and oxidative stress interacts with polymorphism at TLR4. Our results suggest that TLR4 polymorphism can affect an increased the risk of asthma, and that this depends on whether the children were recently given acetaminophen. Additional studies will be required to confirm the interaction between TLR4 and oxidative stress with regard to the development of asthma, to confirm these synergistic effects, and to clarify the underlying mechanisms.
In conclusion, TLR4 polymorphism appears to modify the relationship between acetaminophen use and asthma or BHR in genetically susceptible children. The underlying mechanism for the relationship is likely to be mediated by oxidative stress or innate immune responses. Further studies are required to verify the interaction between TLR4 and acetaminophen and to understand the relationship of this association to the pathogenesis of asthma.



 XML Download
XML Download