

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gout is a common disorder causing painful inflammatory arthritis characterized by hyperuricemia. Hyperuricemia reflects an enlarged body pool of uric acid and increases the risk of precipitation of monosodium urate crystals in joints, connective tissue, and parenchymal organs including the kidneys (1). The prevalence of gout is increasing in not only industrialized countries, but also in emerging countries (2, 3). Patients with gout frequently have multiple comorbidities including hypertension (HTN), type II diabetes mellitus (DM), cardiovascular disease (CVD), chronic kidney disease (CKD), urolithiasis, hyperlipidemia and in combination known as the metabolic syndrome. Treatment of gout with hypouricemic agent was reported to prevent acute gout attacks in a retrospective study (4) and is expected to reduce the development of comorbidities (5) without definite evidence. Furthermore previous study did not target specific serum urate level.
We evaluated the effect of uric acid lowering therapy (ULT), maintaining the serum urate level below 6.0 mg/dL, in reducing the new development of comorbidities, and the frequency of acute attacks in gout patients.
MATERIALS AND METHODS
Patients
We retrospectively examined data of 200 patients who were diagnosed to have gout and treated with hypouricemic agent for at least 3 yr during the period from January 1996 to December 2012 in one rheumatology center. They were divided into 2 groups; the adequately treated group consisted of 53 patients whose mean serum uric acid level (sUA)<6 mg/dL (2012 American College of Rheumatology [ACR] uric acid treatment target [6]) and the inadequately treated group consisted of 147 patients whose mean sUA≥6 mg/dL. The only female patient belonged to the adequately treated group. The serum uric acid level was measured at every outpatient visit at an average of 2 to 3 month intervals (unless the patient refused or forgot) and the mean uric acid level was calculated by using this value. The patients were initially treated with allopurinol. After increasing the dosage to 400 mg and if the patients did not reach sUA<6 mg/dL, allopurinol was changed to febuxostat or benzbromarone. The diagnosis of gout was based on the 1977 criteria proposed by the ACR (7). Hypouricemic agent consisted of allopurinol (85%), febuxostat (1%) and benzbromarone (4%).
Measurements
The characteristics of the patients in each group, including sex, age, height, weight, body mass index (BMI), duration of gout (calculated from first gout attack), duration of ULT (calculated from the first date of starting ULT), presence of tophi, family history of gout, history of smoking or alcohol, medication possession ratio (MPR) and frequency of acute gout attack during follow up period were collected through chart review. History of comorbidities of gout such as HTN, type II DM, CKD, CVD and urolithiasis were investigated at baseline and at the last follow up visit.
Diagnosis of HTN was made if the patient was on anti-hypertensive medication or if the patient showed continuous stage I hypertension or above (SBP over 140 mmHg or DBP over 90 mmHg [JNC 7 guideline]). Diagnosis of DM was made if the patient was on oral hypoglycemic agent or insulin, if the patient showed continuous elevation of fasting glucose above 126 mg/dL or if HbA1c was over 6.5% (American Diabetes Association 2013 guidelines). CKD was defined as glomerular filtration rate (GFR) less than 60 mL/min per 1.73 m2 calculated by modification of diet in renal disease (MDRD) formula. CVD consisted of myocardial infarction (MI), angina, heart failure (HF) and cerebrovascular disease. Diagnosis of urolithiasis was made if the stone was visualized by computed tomography, intravenous pyelogram or abdominal sonography or when confirmed by a physician.
MPR was calculated by dividing the number of medication consumed days by the number of total clinic follow up days and converted into percentage. The MPR was dichotomized at 80%, with MPR of <80% considered non-adherence (8,9,10). Gout flare was defined as an incidence with 3 or more of the following criteria: any patient-reported warm joint, any patient-reported swollen joint, patient-reported pain at rest of >3 (0-10 scale) intensity and patient-reported flare (11) or if directly diagnosed by a physician.
Statistical analysis
Statistical analysis was carried out using the Statistical Package for the Social Sciences (version 19.0; SPSS, Inc., Chicago, IL, USA). The Mann-Whitney U test and chi-square test was used to compare the variables between the 2 groups. McNemar's test was used to evaluate the treatment effects on the incidental comorbidities of gout in each group. A value of P<0.05 was considered significant.
RESULTS
Subject disposition and demographics
There was no significant difference in presence of tophi (19% vs 16%, P=0.222), family history of gout (8% vs 7%, P=0.242), smoking (40% vs 44%, P=0.230), alcohol consumption (60% vs 73%, P=0.112) and hypercholesterolemia (49% vs 54%, P=0.502) between the adequately treated group and the inadequately treated group (Table 1). Patients in the adequately treated group was older (54±13 yr vs 44±12 yr, P<0.001), lighter (70.4±9.9 kg vs 76.0±11.9 kg, P=0.003), shorter (167.16±7.2 cm vs 169.8±6.0 cm, P=0.032) with lower BMI (25.0±2.8 kg/m2 vs 26.3±3.3 kg/m2, P=0.001). There was no significant difference in the duration of gout (11.5±7.1 yr vs 12.1±5.7 yr, P=0.151) and ULT duration (6.9±3.1 yr vs 7.8±3.3 yr, P=0.050). The MPR (94±10% vs 61±27%, P<0.001) and the percentage of patients with MPR≥80% (92% vs 29%, P<0.001) were both higher in the adequately treated group. There was no difference in the frequency of sUA measurement between the adequately and inadequately treated group (35±15 vs 35±21, P=0.718). In the inadequately treated group, 81% (n=119), 4.1% (n=6) and 15% (n=22) of the patients were treated with allopurinol, benzbromarone and febuxostat respectively. In the adequately treated group, 96.2% (n=51) and 3.8% (n=2) of the patients were treated with allopurinol and benzbromarone respectively. There was no significant difference in the dosage of allopurinol between the adequately and inadequately treated group (257±98 mg vs 257±100 mg, P=0.890).
Efficacy analysis
During the mean follow up period of 7.6 yr, the average frequency of acute attack and the yearly rate of acute attack were both lower in the adequately treated group compared to the inadequately treated group (1±2 vs 3±4, P<0.001 and 0.25±0.39 vs 0.47±0.53, P<0.001) (Table 1).
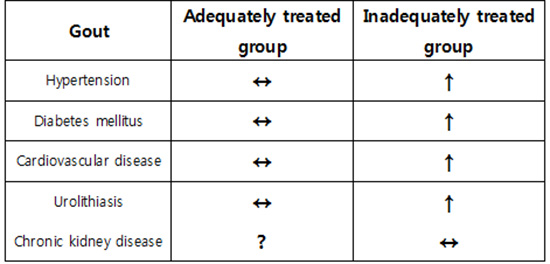
In the adequately treated group HTN increased from 58% to 68%, DM from 8% to 15%, CVD from 23% to 28%, urolithiasis from 8% to 11% and 2 patients showed decrease in CKD stage (Table 2). However, McNemar's test showed no significant increase in incidence of HTN, DM, CVD, and urolithiasis or significant decrease in incidence of CKD stage (Table 2).
In the inadequately treated group HTN increased from 22% to 48% (P<0.001), DM from 6% to 18% (P<0.001), CVD from 5% to 12% (P=0.004) and urolithiasis from 3% to 11% (P=0.001). McNemar's test showed significant increase in incidence of each comorbidity. Only 1 case showed increase in CKD stage (Table 2).
Age and the frequency of baseline HTN which could have influenced the CVD outcome were all higher in the adequately treated group. However BMI was higher in the inadequately treated group which could influence on the HTN, DM and CVD state. Generalized estimating equation (GEE) analysis after adjusting for BMI also showed higher incidence of HTN and CVD (P<0.001, P=0.002, respectively) in the inadequately treated group. There was no difference in the DM outcome (P<0.762).
DISCUSSION
Although the optimal uric acid level to be achieved with ULT has been controversial (12, 13, 14), the 2012 ACR guideline and 2013 multinational evidence-based recommendations (15) recommends the uric acid treatment target of <6 mg/dL with ULT in gout patients. Our study demonstrated that tight control of uric acid decreased the development of acute gout attacks which was correlated with the study by Shoji et al. (4). Patients with high MPR of urate lowering agent consequently achieved mean uric acid level of <6 mg/dL and effectively reduced the risk of acute gout attacks. Theoretically serum is supersaturated for monosodium urate at concentrations >6.8 mg/dL at 37℃ and urate levels below this can be considered appropriate target for treatment (16).
Hyperuricemia is common in patients with HTN. Among patients with gout, 40% have hypertension (17, 18). Kanbay et al. (19) reported significant reduction in blood pressure in hyperuricemic patients treated with allopurinol and Feig et al. (20) reported reduction in blood pressure in adolescents with newly diagnosed essential hypertension treated with allopurinol. Treatment with xanthine oxidase inhibitor allopurinol may contribute to reduction in blood pressure. However, there is yet to be a study on blood pressure in gout patients treated with allopurinol. This study also showed no significant increase in the prevalence of HTN in the group tightly treated with ULT. However, in the inadequately treated group there was a significant increase in the prevalence of HTN after mean follow up period of 7.6 yr. In this study 85% of patients were treated with allopurinol and early treatment with allopurinol could have prevented the new development of HTN.
Serum uric acid level increases with increasing hemoglobin A1c (HbA1c) up to 6-6.9% and then decreases with a further increase in HbA1c (21). Whether optimal management of gout with ULT reduces the risk of future DM is unknown. The Finnish diabetes prevention study, based on 557 overweight or obese individuals with impaired glucose tolerance, reported that baseline uric acid predicted the risk of diabetes after adjusting for age, gender, blood pressure, BMI, triglyceride levels, baseline creatinine, physical activity and dietary variables (P=0.037) (22). Choi et al. (23) reported that men with gout and high cardiovascular risk are at risk of developing type II DM independent of other known risk factors compared with men without gout. Our study showed significant increase in prevalence of DM in the inadequately treated group compared to the adequately treated group at the end of follow up period. After adjusting for BMI, there was no significant difference in the incidence of DM between the 2 groups. However, our study did not include other risk factors for DM such as HDL cholesterol level <35 mg/dL, triglyceride level>250 mg/dL, or family history of DM.
This study showed significant increase in prevalence of CVD in the inadequately treated group compared to the adequately treated group. In vitro and animal studies suggest that uric acid is a biologically active compound that can increase inflammatory mediators such as monocyte chemoattractant protein-1 and nuclear factor-kappa B (24) known to lead to vascular damage. Framingham study (25) found 60% increased risk of coronary artery disease among gout patients and Edwards (26) reported that hyperuricemia is an independent risk factor for CVD. Hyperuricemia itself is associated with cardiovascular risk factors such as HTN and DM. Allopurinol itself through its ability to reduce myocardial oxygen demand also appears to be beneficial in patients with ischemic heart disease (27).
The most frequent type of gout-related-nephropathy is urolithiasis (10%-20%) and its prevalence is much higher than that observed in the general population (28). In 1967, Yü and Gutman (29) investigated 1,258 patients with primary gout and reported a 22% prevalence of urolithiasis, based on history of urolithiasis during the course of gout. Shimizu et al. (30) reported the prevalence of urolithiasis calculated from stone history was 16.2%. Our study showed urolithiasis prevalence of 11%. At baseline, we included the patients who reported medical history of urolithiasis. During the follow up period, we only included radiologically proven urolithiasis or urolithiasis confirmed by a physician. This could explain the lower prevalence of urolithiasis in our study. This study shows that strict control of uric acid level below 6.0 mg/dL with ULT is beneficial in decreasing the new development of urolithiasis.
Renal impairment is associated with hyperuricemia, which also contributes to renal impairment. Zhu et al. (31) reported that of the estimated 8.3 million Americans effected with gout, 71% had CKD greater than stage 2 (GFR<60 mL/min per 1.73 m2), using 2007-2008 data from the National Health and Nutrition Examination Survey. With increasing levels of sUA, there were graded increases in the prevalence of CKD. In our study there was a decrease in the frequency of CKD in the adequately treated group from 21 to 19 patients and in the inadequately treated group there was an increase from 26 to 27 patients. Although there was no statistical difference in the adequately treated group, this shows that renal function can be recovered by intensive ULT therapy.
The ideal MPR is 100% and good adherence is generally defined as an MPR of 80% or higher. Gout is among the chronic diseases with a low treatment adherence rate which is interestingly lower in younger patients (32). In studies of pharmacy dispensing gout medications, the percentage of patients with good adherence ranged from 18% to 44% (33). In a comparative study showing a 36.8% adherence rate among gout patients, patients with HTN or type II DM had higher rates of 72.3% and 65.4% respectively (32). In our study 46% of patients showed good adherence compared to 92% of patients in the adequately treated group who showed good adherence. The patients in the adequately treated group were also older, with higher prevalence of HTN and DM at baseline which could have influenced the drug adherence rate, in accordance with other studies.
The mean age of the patients in the adequately treated group was higher than the age of the inadequately treated group. This could explain the reason why higher percentage of patients in the adequately treated group had HTN, DM, CVD, urolithiasis and CKD compared to the inadequately treated group at baseline. However, only HTN, CVD and CKD showed significant difference (P<0.001) between the 2 groups at baseline (Table 1).
In conclusion, long term ULT maintaining the serum urate level under 6 mg/dL leads to significant decrease in the incidence of gout comorbidities such as HTN and CVD after adjusting for BMI. New development of DM and urolithiasis tends to decrease in the well-treated group despite the older age and preexisting comorbidities. Tight control of uric acid also decreases the development of acute gout attacks and can also potentially lead to recovery of renal function. Prospective randomized study is needed to confirm these results, taking into consideration other confounding factors for each comorbidity of gout.

 XML Download
XML Download