

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The impact of positive lymphocyte cross-matching (XM) has been reported and antibody-mediated rejection (AMR) still remains a serious problem in the field of solid organ transplantation (1, 2). Human leukocyte antigen (HLA) XM is currently accepted as a mandatory test for kidney, heart, and lung transplants to improve survival outcomes in an era of donor shortages (3). This has not been the case with liver transplantation (LT). From the beginning, the liver was found to be unusually resistant to hyperacute rejection (HAR). An analysis of a large series from the cyclosporine era showed no difference in 2-yr graft or patient survival when stratified according to lymphocyte XM results, thereby casting doubt on the relevance of this test in clinical LT. However, Donaldson et al. (4) later reported an apparently strong association between vanishing duct syndrome and preformed HLA class I antibody. Thus, negative survival outcomes of grafts with positive lymphocyte XM is still a matter of debate in the field of LT (2, 5, 6, 7, 8).
Generally, it has been believed that a positive lymphocyte XM does not contraindicate LT. However, it does have a negative impact on early rejection-free graft survival, especially in the case of retransplantation involving a marginal graft and a severely ill recipient and in cases of adult-to-adult living donor liver transplantation (ALDLT) with a relatively small-for-size graft (SFSG) (2, 6).
In many Asian countries, including Korea, most adult LTs have been performed by ALDLT. In contrast to deceased donor LTs, the live donor-recipient pair have time to prepare. The New York State Committee (9) recommended the time for a live donor evaluation must be more than 2 weeks. Therefore, during the evaluation period for a LDLT, in common with many other Japanese and Korean transplant centers, we routinely perform a lymphocyte XM test (2, 10, 11).
There has been no pre-transplant desensitization protocol for the highly sensitized patients in LDLT. Until now, post-transplant management of AMR; i.e., plasma exchange, high-dose immunoglobulin, aggressive immunosuppression, and splenectomy have been used in lymphocyte XM-positive LTs (7, 12, 13, 14). However, these treatments had less impact on serious complications of lymphocyte XM-positive recipients, leading to patients' deaths. We (6) previously described four recipients with positive lymphocyte XM and with an SFSG who died of multi-organ failure and sepsis, regardless of receiving treatment for early postoperative acute rejection episodes. However, the incidence of lymphocyte XM positivity is low, and immunological complications associated with lymphocyte XM positivity are more uncommon. Thus, this fatal outcome was not studied and predicted well.
In this study, we investigated the feasibility of pre-transplant desensitization according to the degree of T lymphocyte cross-match titer, model for end-stage liver disease (MELD) score, and graft liver volume based on clinical and histopathological evaluation.
MATERIALS AND METHODS
We retrospectively reviewed 230 consecutive ALDLT recipients at our institution from January 2005 to June 2009.
Lymphocyte cross-match protocol
Complement-dependent cytotoxicity (CDC) XM analysis of the T cells was routinely undertaken, in addition to flow cytometry XM (FCXM) analysis of the T cells and the B cells, for all LDLT patients preoperatively. The T-cell CDC XM tests consisted of both the standard method of the National Institutes of Health (T-NIH) and the antihuman globulin-augmented method (T-AHG). The CDC XM test was interpreted as positive if more than 15% of the donor lymphocytes were killed by the recipient's serum. Serial two-fold dilutions of the recipient's serum (1:1-1:32) were performed in the CDC XM test, and the titer was defined as the highest dilution of test serum giving a positive result. The CDC XM test was interpreted as positive if the T-AHG was positive, regardless of the results of T-NIH. A positive T-NIH but negative T-AHG was usually found to be due to auto-reactive IgM type antibodies, and these cases were excluded. For the FCXM, the T and B cells were stained in a single tube using pronase-treated cells and three-color immunofluorescence staining, as previously described (15). The fluorescence-stained cells were analyzed with a flow cytometer (FACS Calibur Analyzer, Becton-Dickinson, San Jose, CA, USA). The FCXM was interpreted as positive when the ratio of median fluorescence intensity of the test serum compared with that of the negative control serum (normal human AB type serum) was ≥2.0. The panel reactive antibody (PRA) test was selectively performed in patients with a high titer of T-cell CDC XM.
Desensitization protocol
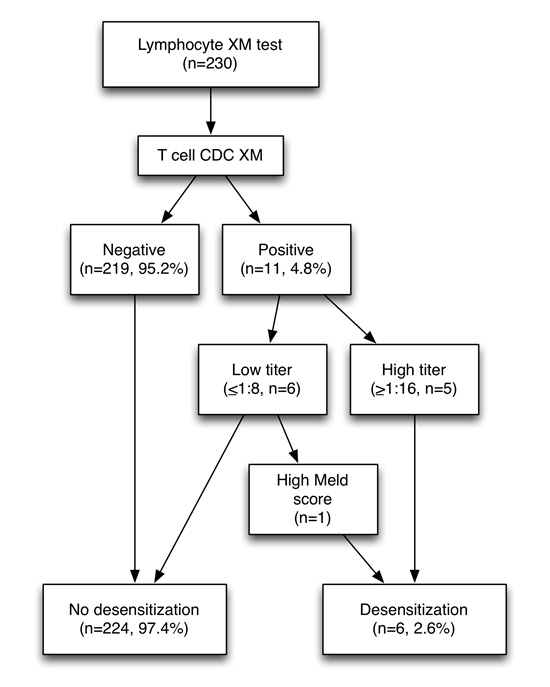
The desensitization protocol was applied to the lymphocyte XM-positive patients with a high T-AHG titer (≥ 1:16) or to the patient with a high MELD score, even though the T-cell CDC XM titer was low (Fig. 1) (2). The T- or B-cell FCXM-positive cases without positive reactions in the T-cell CDC XM test were not considered for desensitization.
The protocol consisted of an anti-CD 20 antibody (rituximab, 375 mg/m2 body surface area) injection 3 weeks before the transplantation, and two or three sessions of plasmapheresis (PP) one week before the LT (Fig. 2). As per previous studies (16, 17), in urgent cases, intravenous immunoglobulin was injected rather than rituximab when there was insufficient time to administer rituximab before the LT. The post-PP target T-AHG titer was less than 1:16. After the LT, we checked the T-cell CDC XM titer weekly for 4 weeks. If the T-cell CDC XM titer was more than 1:64, we planned the post-LT PP. Baseline peripheral B-cell levels were sampled 3 weeks before and 3 weeks after the LT.
A liver biopsy protocol and a dynamic CT scan were routinely performed on postoperative day (POD) 10 for early detection of subclinical graft rejection and surgical complications. The diagnosis of AMR was based on the patients' histopathological findings (Banff score ≥3) and C4d immunohistochemistry (18). Positive C4d staining was defined as linear staining of portal venous and capillary endothelial cells.
Immunosuppression
The immunosuppression protocol for the positive lymphocyte XM recipients was the same as that of the negative lymphocyte XM recipients. It comprised quadruple therapy based on basiliximab induction (20 mg administered twice, just before the operation and on POD 4) and maintenance triple therapy: tacrolimus, mycophenolate mofetil, and steroids. Tacrolimus was initiated at a dose of 0.075 mg/kg per orally on POD 2, and the dose was changed according to the target levels: 10-12 ng/mL during the first 2 weeks, 8-10 ng/mL during the first 3 months, and then 5-8 ng/mL thereafter. The steroid was initiated at a dose of 500 mg before and after reperfusion during the operation and then reduced to 20 mg at the end of the first week and changed to an oral form. It was tapered to 10 mg/day until the third month after the LT and then gradually withdrawn over the next 3 months. Mycophenolate mofetil was initiated at a dose of 500 mg twice a day.
RESULTS
Characteristics of the lymphocyte XM-positive recipients
In this study, preoperative lymphocyte XM was positive in 11 recipients (4.8%) among the 230 ALDLT patients (Fig. 1). Among these 11 patients, six had a low titer of T-AHG, ranging from 1:1 to 1:4 (Table 1). The median age of these lymphocyte XM-positive recipients was 50 yr (range, 34-57). Female patients were dominant, comprising 10 of 11 XM-positive cases. The median age of the donors of these lymphocyte XM-positive recipients was 33 yr (range, 17-47). Male donor was dominant, eight in total. There were no ABO-incompatible (ABOi) LTs, and 10 of the patients received a graft from identical blood type donors. In HLA typing, 10 of the patients showed 1-haplotype match and one patient showed 0-haplotype match. The median graft versus recipient weight ratio (GRWR) was 1.32% (range, 0.82-1.89). We did not perform the desensitization protocol for these patients with a low titer, except for one patient (case No. 6) who had a high MELD score of 36, irrespective of the low T-AHG titer (1:4). All the other five patients with a high T-AHG titer underwent the desensitization protocol.
Pre-LT desensitization
Five of the six patients received a rituximab injection, but this drug was not administered to one patient (case No. 7) with a high titer (> 1:32). Because she experienced cholangitis just before LT, there was no time to wait the impact rituximab. In this patient, a high dose of intravenous immunoglobulin was administered for nine consecutive days after transplantation. All six recipients underwent PP two to three times before the LT. The post-PP T-AHG titer was markedly decreased before the transplantation in four of the patients; negative conversion was achieved in three cases (50%, case No. 6, 10, 11), and a significant drop was noted in one case (case No. 7). The desensitization treatment was not associated with any major complications (more than Grade 3 requiring intervention) or infectious episodes (Table 2) (19). Although five of the recipients had hepatitis B-related liver cirrhosis (HB LC), there was no flare up of viral hepatitis before the LTs. Minor complications were noted in two of the patients (case No. 9, 11): urticaria and transient hypotension during PP.
Liver transplantation procedures
The operation procedures were not different from the negative lymphocyte XM recipients (20). None of the patients underwent splenectomy. All 11 patients received a right liver with interposition vascular graft draining of the middle hepatic vein branches of the anterior section (20). The median operation time was 465 min (range, 350-810), and the total ischemic time was 133.5 min (range, 35-169).
Outcome of LT and case review of the desensitization group
The median observation period was 23.5 (range, 0-55) months after LT. There was no recurrence of hepatitis B or hepatocellular carcinoma (HCC) during the follow-up period. There was no mortality and no HAR (1 acute cellular rejection [ACR]) after the transplantation in the lymphocyte XM-positive recipients (Table 2). In the lymphocyte XM-negative group (n=219), there were 15 cases of mortalities (6.8%) with 20 cases of rejection (9.1%). The outcome showed no significant difference in survival (P=1.000) and rejection (P=0.605) between lymphocyte XM-positive and XM-negative recipients (Table 3).
Case No. 6
A 52-yr-old woman with HB LC (MELD score 36 and United Network of Organ Sharing [UNOS] status 2B) and HCC received a modified right liver (GRWR, 1.25%) from her 34-yr-old ABO-identical son-in-law. The initial T-AHG was 1:4, the T- and B-cell FCXM were all positive, and PRA I and II were 90% and 77%. The patient underwent preoperative desensitization (rituximab and PP three times). The T-AHG was negative before the LT. On POD 10, there was no acute cellular rejection (ACR) or C4d deposition on the protocol biopsy. She experienced postoperative bleeding (Grade 3B) but recovered well. She was discharged on POD 23. The follow-up duration was 40 months.
Case No. 7
A 38-yr-old woman with primary biliary cirrhosis (MELD score 17 and UNOS status 3) received a modified right liver (GRWR, 1.39%) from her ABO-identical 41-yr-old brother. The initial T-AHG was > 1:32, and the T- and B-cell FCXM were positive. The post-PP T-AHG titer had decreased to a titer of 1:8, although the T- and B-cell FCXM were still positive. Intravenous immunoglobulin was administered nine times after the transplantation. There was no ACR or C4d deposition on the protocol biopsy on POD 10. She recovered well and was discharged on POD 13. During follow-up, she experienced ACR (Banff score 4) at 5 yr after LT (Fig. 3A). Fortunately, there was no C4d staining on the biopsy. She recovered following steroid pulse therapy. The follow-up duration was 7 yr.
Case No. 8
A 44-yr-old woman with HB LC (MELD score 17 and UNOS status 2B) received a modified right liver (GRWR, 1.32%) from her ABO-identical 17-yr-old son. The initial T-AHG titer was 1:16, the T- and B-cell FCXM were positive, and PRA I and II were 100% and 77%. The patient underwent a desensitization protocol (rituximab and PP three times). The post-PP T-AHG titer had decreased to 1:2 seven days before the transplantation. However, it rebounded to more than 1:32 one day before the LT. Because her GRWR and her MELD score were acceptable, she underwent elective ALDLT. We assessed her lymphocyte XM again on PODs 4 and 14 to decide upon further treatment. Fortunately, post-LT, all lymphocyte XM tests showed a negative conversion. There was no ACR or C4d deposition on the protocol biopsy on POD 10. She recovered well and was discharged on POD 19. The follow-up duration was 6 yr.
Case No. 9
A 50-yr-old man with HB LC and HCC (MELD score 16 and UNOS status 2B) received a modified right liver (GRWR, 1.31%) from an ABO-identical unrelated 25-yr-old male donor. The initial T-AHG titer was> 1:32, the T-cell and B-cell FCXM were all positive, and PRA I and II were 100% and 53%, respectively. The patient underwent a desensitization protocol (rituximab and PP twice). The post-PP T-AHG titer was 1:32. As his GRWR and his MELD score were acceptable, he underwent elective ALDLT. His T-AHG titer was still 1:32 on PODs 6 and 14. On the protocol biopsy on POD 10, C4d linear deposition was noted on portal venous and capillary endothelial cells (Fig. 3B). However, he had no clinical symptoms or signs of AMR or ACR. The follow-up T-AHG titer was negative on POD 25. He was discharged on POD 32. During the 5-yr follow-up, there has been no adverse event.
Case No. 10
A 48-yr-old woman with HB LC and HCC (MELD score 13 and UNOS status 3) received a modified right liver (GRWR 1.55%) from her ABO-identical 49-yr-old brother. The initial T-AHG titer was 1:16, the T-cell FCXM was positive, and the B-cell FCXM was negative. PRA I and II were 100% and 73%, respectively. She underwent a desensitization protocol (rituximab and PP twice). The post-PP T-AHG titer was negative, but the T-cell FCXM was still positive. After the LT, the T-AHG and T-cell FCXM test showed a negative conversion on POD 6. There was no ACR or C4d deposition on the protocol biopsy on POD 10. She recovered well and was discharged on POD 24. The follow-up duration was 55 months.
Case No. 11
A 51-yr-old woman with HB LC (MELD score 32 and UNOS status 2B) received a modified right liver (GRWR 0.82%) from her ABO-identical 25-yr-old son-in-law. The initial T-AHG was > 1:32, the T- and B-cell FCXM were positive, and PRA I and II were 98% and 97%, respectively. She underwent a desensitization protocol (rituximab and PP three times). The post-PP T-AHG titer was negative, and it was sustained until POD 17. There was no ACR or C4d deposition on the protocol biopsy on POD 10. She recovered well and was discharged on POD 26. During the follow-up period, intrahepatic biliary tract stones formed 15 months after LDLT, and choledochoscopic removal was successfully performed. The follow-up duration was 4 yr.
In summary, among the six cases of desensitization, four were successful; three cases achieved a negative conversion, and one case achieved a low T-AHG titer. However, in two cases, the post-PP T-AHG titer remained high (1:32). These two cases showed a postoperative negative conversion of lymphocyte XM.
DISCUSSION
Preoperative desensitization has not been performed for patients with a positive lymphocyte XM test (2, 6, 7, 8, 12, 13, 21, 22). HAR after LT is rare but can be caused by preformed donor-specific antibody in the recipient. It is well known in ABOi LT. It can also occur in ABO-compatible LT. Recently, most centers that perform ABOi LDLTs have reported reasonable outcomes when they performed preoperative desensitization consisting of rituximab and PP. However, Hori et al. (2) showed that a positive lymphocyte XM test was a more important risk factor than ABO incompatibility in terms of HAR and graft survival. Efforts to manage HAR have not been successful (2, 7, 8, 23, 24).
Several studies (11, 12, 25) have also shown that positive lymphocyte XM tests were not prognostic factors, although the prevalence of ACR, but not refractory HAR, was higher than that in the negative lymphocyte XM tests. Treatable ACR may not induce graft loss under surveillance for early detection. However, in these studies, lymphocyte XM positivity was not classified according to the degree of the T-cell CDC XM titer. Neither was it classified according to the T-cell CDC XM test, but included a positive FCXM, as well as a low T-cell CDC XM titer. For this reason, we performed the desensitization protocol, adopted from the protocol of an ABOi LDLT, for patients with a high risk of graft failure due to a high titer (> 1:16) of T-AHG. Patients with low titer underwent LDLT without desensitization according to the ABOi LDLT protocol.
Considering the results of previous large-scale studies (2, 21, 26, 27) and our previous report (6), the preoperative desensitization may decrease the risk of rejection, including HAR, and overcome the risk of short-term graft failure. It may also eventually enhance long-term survival of the graft. Recently, Aoki et al. (26) reported outcomes in a patient with a remarkably high positive lymphocyte XM result (> 1:10,000). They performed desensitization of this patient according to our center's protocol (as acknowledged in their report). The patient experienced ACR (Banff score 3) on POD 27, but it was well treated by steroid pulse therapy. The lymphocyte XM test remained negative one year after the LT.
There are other well-known risk factors of survival outcome after LT, i.e., SFSGs (GRWR < 0.8%), elderly recipients, elderly donors, high MELD score, and steatosis of the graft (2, 27, 28, 29, 30, 31, 32). These factors could have an additional negative impact on the survival of grafts among recipients with a positive lymphocyte XM test. A SFSG might not be able to tolerate AMR, and additional immunosuppression against ACR might cause complex complications, including infection. Because management of small-for-size syndrome is complex, additional negative impact of immunological problems makes the matter worse. In our previous report (6), most of the recipients had a SFSG and died of multi-organ failure with sepsis (n=2), pneumonia (n=1), and circulatory shock (n=1) after treatment of ACR. One of these patients showed a severe degree of ACR (Banff score 8) with C4d deposition (Fig. 3C). In contrast, an enough size graft may be resistant to AMR because it can absorb the antibodies (33, 34, 35). Since 2005, we have routinely used a modified right liver graft to obtain a sufficiently sized graft in ALDLTs (20). Therefore, although we sometimes use a borderline-sized graft or even an SFSG (< 0.8% of GRWR) in the ALDLT setting, functional graft volume could be enough. Cases No. 8 and No. 9 were rebounders and had a risk of AMR. They underwent LDLT without additional PP because of the relative large size of the grafts (GRWR 1.32% and 1.31%) and sufficient patient condition, which might have an important role during the immediate postoperative period. Otherwise, we would have performed more PPs before LDLT.
Finally, the application of the desensitization protocol consisting of rituximab and PP in these six patients (2.6%) resulted in successful depletion of donor-specific antibodies in four of the patients. Another two patients with post-PP rebound in the titer showed good outcome because they have enough graft volume and not so high MELD score. All eleven T-cell CDC XM positive patients including 6 recipients who underwent desensitization have good outcome showing no statistical difference in rejection and survival compared to XM negative patients, in contrast to the previous reports.
In conclusion, the tailored desensitization protocol for selected recipients according to the titer of T-cell CDC XM, especially T-AHG, graft size, and patient condition is feasible and necessary for optimal outcome. However, it is difficult to perform a randomized controlled study and validation study because patients with significantly high titer of T-cell CDC XM positivity are rare in the ALDLTs.





 XML Download
XML Download