

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic hepatitis B (CHB) often leads to serious health conditions including decompensated liver cirrhosis and hepatocellular carcinoma (HCC) (1). Host immune response to HBV infected hepatocytes results in hepatocyte apoptosis and necrosis that activates nonparenchymal cells including hepatic stellate cells to produce extracellular matrix such as type I collagen resulting in hepatic fibrosis (2, 3). Hepatic fibrogenesis is a dynamic process with a net result of fibrotic scar formation. Resolution of scars determines the progression from hepatic fibrosis to liver cirrhosis (4). The suppression of viral replication by long-term antiviral therapy may improve hepatic inflammation and fibrosis and halt the progression of disease to decompensated liver cirrhosis and HCC (5, 6). Lamivudine treatment decreased complications from portal hypertension and the development of liver cancer in patients with compensated liver cirrhosis, although the benefit was less in patients who develop lamivudine resistance (7). Entecavir treatment for 48 weeks in patients with advanced hepatic fibrosis or cirrhosis showed the improvement of liver histology in 57% with HBeAg+ve, 59% with HBeAg-ve, and 43% of patients with lamivudine-resistant CHB (8).
Accurate information about the hepatic fibrosis stage is very important in clinical practice because the extent of hepatic fibrosis predicts the development of hepatic decompensation and HCC in patients with CHB (9, 10). Liver biopsy has been a gold standard to assess the extent of hepatic fibrosis (11). However it is hard to perform liver biopsy repeatedly in patients with CHB because of its invasive nature. Instead, the assessment of liver stiffness using fibroscan has been reported as a relevant non-invasive tool for the assessment of hepatic fibrosis in various kinds of chronic liver disease including hepatitis B, hepatitis C, and alcoholic liver disease (12). In this study we aimed to evaluate the regression of hepatic fibrosis through repeated liver stiffness measurement (LSM) using fibroscan during long-term oral antiviral therapy in patients with CHB.
MATERIALS AND METHODS
Patients
From October 2007 to February 2011, a total of 3,156 LSM was performed in Gangnam Severance Hospital, Seoul, Korea. Eighty eight CHB patients on oral nucleos(t)ide therapy who received LSM twice were retrospectively enrolled. Five patients who had the interval between the first and the second LSM was shorter than 6 months, were excluded. No patients were positive to anti-hepatitis C virus (HCV) antibody (Ab) or anti-human immunodeficiency virus Ab. Finally, 83 patients were included in this study. We retrospectively reviewed the medical records and analysed the change of liver stiffness measured by transient elastography (Fibroscan®, Echosens, France). The patients were followed up every 3 months with serologic tests. When virologic breakthrough due to the development of antiviral drug resistance was confirmed, nucleos(t)ide analogue was added or changed according to resistant mutation.
Laboratory tests
HBsAg and HBeAg/Ab were determined by enzyme immunoassay (Dade Behring, Marburg, Germany). Serum HBV DNA was measured by a real-time polymerase chain reaction assay using a COBAS TaqMan 48 analyzer (Roche Diagnostics, Mannheim, Germany) with a detection limit of 12 IU/mL. The antibody against HCV was detected by a third-generation enzyme-linked immunosorbent assay (Korea Greencross, Yong-in, Korea).
Liver stiffness measurement (LSM)
Well trained and experienced physicians obtained all LSM according to the instructions provided by the manufacturer. All patients received LSM using FibroScan® two times during oral nucleos(t)ide antiviral therapy. The first LSM was performed before the starting antiviral therapy (n=33, 39.8%) or during follow up visit on antiviral therapy (n=50, 60.2%). The timing of the 2nd LSM was decided by physician's or patient's discretion to monitor liver stiffness. The mean interval between the first and the second LSM was 411.5±149.5 (range: 180-1,062) days. LSM was performed on the right lobe of the liver through the intercostal spaces on patients lying in the dorsal decubitus position with the right arm in maximal abduction (13). The results are expressed as kilopascals (kPa). The extent of liver fibrosis was classified according to the METAVIR scoring system (F0-F4). Transient elastography cut-off levels used for staging liver fibrosis ≥F2, ≥F3, and F4 were 8.8, 10.2, and 14.1 kPa, respectively (14).
The interquartile range (IQR) was defined as an index of intrinsic variability of LSM corresponding to the interval of LSM results containing 50% of the valid measurements between the 25th and 75th percentiles. The median LSM was selected as representative of the LSM value in a given patient. In this study, only LSM examinations with at least ten validated measurements, an IQR to median value ratio (IQR/M) was less than 0.3, and a success rate of at least 60% were considered reliable and were included for the analysis.
Statistics
Data were analyzed using the statistical software SPSS (version 13.0, SPSS Inc., Chicago, IL, USA). Quantitative variables are expressed as mean±standard deviation. The degree of difference of LSM between two time points (% per month) was calculated as follows;

Data were analyzed using paired t-test, Wilcoxon signed rank test, Mann-Whitney U test, oneway ANOVA, and chi-square test. Data were considered to be statistically significant with P < 0.05.
RESULTS
Baseline characteristics of the patients
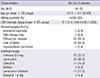
The baseline characteristics of the 83 patients are presented in Table 1. There were 61 men and 22 women, with a mean age of 51.5±9.1 yr. The mean interval between two LSMs was 411.5 ±149.5 (180-1,062) days. The number of patients received antiviral therapy as follows; entecavir 0.5 mg in 28 (33.7%), lamivudine in 22 (26.5%), clevudine in 14 (16.9%), adefovir in 4 (4.8%), lamivudine plus adefovir in 11 (13.3%), and entecavir 1.0 mg in 4 (4.8%) patients. Eighty patients (96.4%) showed serum HBV DNA below 2,000 IU/mL at 2nd LSM.
Comparison of clinical parameters between two LSMs during antiviral therapy
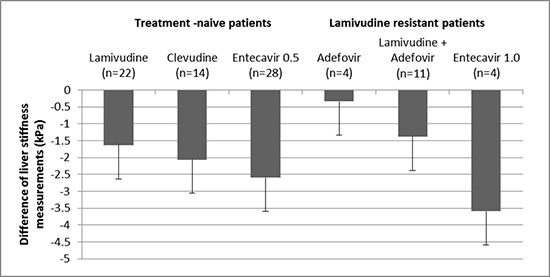
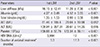
Clinical parameters and liver stiffness values are demonstrated in Table 2. During the antiviral therapy, aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, and HBV DNA levels were decreased. Accordingly, serum albumin levels and platelet count increased during the antiviral therapy. Liver stiffness values significantly decreased from 16.15± 12.41 kPa to 11.26±7.36 kPa during the antiviral therapy (P < 0.001). Sixty-two (74.7%) patients had a lower liver stiffness value at 2nd LSM compared to 1st LSM. The degree of regression of liver stiffness value was -2.03±0.36 (-10.25~8.83)% per month. There was no difference of the degree of regression of liver stiffness between the patients in whom initial LSM was obtained before starting antiviral therapy (n=33) and the patients in whom initial LSM was obtained during antiviral therapy (n=50) (-2.54 ±3.13 vs -1.69±3.35% per month, P =0.251). The difference of liver stiffness value between 1st and 2nd LSMs by the type of antiviral agents is summarized in Fig. 1. The differences of two LSM values were all negative regardless of antiviral agents. However, there was no significant difference according to the kind of antiviral agents (P = 0.625) or lamivudine resistance (P = 0.078).
Of the 30 (36.1%) patients with LSM≥14.1 kPa (cirrhosis) at 1st LSM, 25 (83.3%) had a lower LSM value and 12 (40%) proved to no longer have cirrhosis (≥1 decrease in fibrosis stage) at 2nd LSM.
Comparison of groups according to the change of LSM value during antiviral therapy
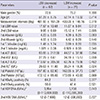
We compared the clinical parameters according to the presence of the improvement of LSM value during antiviral therapy (Table 3). Sixty two (74.7%) patients had a decrease in liver stiffness value (group 1), whereas 21 (25.3%) showed an increase in liver stiffness value (group 2) during antiviral therapy. There was no difference in sex, age, LSM intervals, baseline laboratory profiles including AST, ALT, total bilirubin, HBeAg positivity, HBV DNA levels between two groups. Only 1st LSM value was higher in group 1 (P = 0.012), and 2nd LSM value was lower in group 1 compared to group 2 (P = 0.005).
Comparison of groups according to the change of fibrosis stage during antiviral therapy
The patients' initial fibrosis stages were 16 (19.3%) in F0-1, 15 (18.1%) in F2, 22 (26.5%) in F3 and 30 (36.1%) in F4, respectively. After antiviral therapy, the patients' fibrosis stages were 42 (50.6%) in F0-1, 6 (7.2%) in F2, 12 (14.5%) in F3 and 23 (27.7%) in F4, respectively (Fig. 2). The fibrosis stage was improved in 37 (44.6%) between two LSMs. Thirty eight (45.8%) patients showed no change of fibrosis stage, only 8 (9.6%) showed the aggravation of fibrosis stage. Among these 8 patients, their initial ultrasonographic findings were diffuse liver disease in 2 patients, and liver cirrhosis in 6 patients. The antiviral treatment for these 8 patients was as follows; lamivudine for 2 patients, clevudine for 2 patients, entecavir for 2 patients, adefovir for one patient, and lamivudine and adefovir combination for one patient. Clinical parameters according to the improvement of fibrosis stage were compared (Table 4). There was no difference in age, LSM intervals, initial laboratory profiles including AST, ALT, total bilirubin, HBeAg positivity, and HBV DNA levels. However, patients with improved fibrosis stage were female predominant, and had lower initial LSM value and higher initial albumin level.
Comparison of groups according to ALT levels at 1st LSM during antiviral therapy
It has been reported that ALT level may affect the LSM value. So we compared two groups accoding to ALT levels at 1st LSM time point (Table 5). AST, ALT, and HBV DNA levels were significantly higher in the high ALT (>upper limit of normal [ULN]×2) group. However, there was no difference in sex, age, LSM measurement intervals, baseline albumin, total bilirubin, and HBeAg positivity between two groups. The second LSM significantly decreased in both high ALT (>ULN×2) and low ALT (≤ULN ×2) group compared to 1st LSM (P < 0.001; P=0.001, respectively).
DISCUSSION
Chronic HBV infection is one the most common etiologies of chronic liver disease in Korea (15). There are several clinical features of HBV-related chronic liver diseases in Korean population (16). HBV genotype C is more than 95%, and precore and core promoter mutant HBV are common. Lamivudine resistance is not uncommon among CHB patients who are candidates for the treatment with oral nucleos(t)ide analogues in Korea. The aim of treating patients with chronic HBV infection is to prevent disease progression to liver cirrhosis and hepatocellular carcinoma (17). Oral antiviral agents are widely used to suppress viral replication and to prevent disease progression. However, long-term antiviral therapy is usually required because of the nature of oral nucleos(t)ide analogues. After introduction of potent antiviral agents such as entecavir or tenofovir, it becomes possible to maintain HBV viral load very low or even undectable during long-term antiviral therapy. Moreover, the reversal of hepatic fibrosis/cirrhosis was observed in patients with long-term oral antiviral therapy (6).
Liver fibrosis results from wound healing response for chronic inflammation in the liver. The stage of liver fibrosis has a good correlation with liver-related clinical outcome such as decompensated liver cirrhosis or even development of HCC (18, 19). The accurate information about the extent of liver fibrosis in patients with CHB is clinically very important for the evaluation of severity of the disease, for making treatment decisions and for evaluating efficacy of antiviral treatment. Liver biopsy has long been a gold standard to assess the degree of liver fibrosis (11). However, because of invasive nature and risk of bleeding complication it is difficult to perform liver biopsy, particularly when it needs to be repeated in real clinical practice. Moreover, liver biopsy has limitations such as extremely small sampling size representing only 1/50,000 liver volume, intra- or inter-observer variation for the accurate assessment of liver fibrosis (20).
Recently noninvasive methods such as transient elastograpy, acoustic radiation force impulse (ARFI), Fibro-CT, MRI have been explored for the assessment of hepatic fibrosis (12). Liver stiffness measurement by fibroscan is the most widely used noninvasive method for assessing the extent of liver fibrosis. It was reported that LSM discriminates significant liver fibrosis or liver cirrhosis (F4) with high accuracy in patients with chronic viral hepatitis (21, 22). Our study showed that mean LSM was decreased from 16.15±12.41 kPa to 11.26±7.36 kPa during antiviral therapy for an average 411 days, suggesting the regression of hepatic fibrosis during oral antiviral therapy. The average of degree of regression of liver stiffness during antiviral therapy was -2.03±0.36% per month. There was no statistical difference of degree of regression by the type of antiviral agents or presence of lamivudine resistance. These results might be caused by the small number of patients in each oral antiviral agents group, and should be studied further in a larger study.
The heterogeneous timing of LSM from the retrospective study design is a limitation. The 1st LSM was measured as a baseline before starting antiviral therapy in 33 patients (39.8%). Median duration of antiviral treatment to 1st and 2nd LSM time point was 5.3 and 17.3 months, respectively. There was no difference of the degree of regression of liver stiffness between the groups in whom initial LSM was obtained before starting antiviral therapy (n=33) and the patients in whom initial LSM was obtained during antiviral therapy (n=50) (-2.54±3.13 vs -1.69±3.35% per month, P = 0.251). Therefore it is less likely that the improvement of LSM mainly resulted from lead time bias by previous long-term antiviral therapy.
In our study, we adopted LSM cut-offs for fibrosis staging from a previous report in which Korean patients with genotype C HBV infection were studied. Of the 30 (36.1%) patients with LSM ≥14.1 kPa (F4) at 1st LSM, 12 (40%) proved to have improved fibrosis (LSM less than 14.1 kPa) at 2nd LSM. According to recent meta-analysis, weighted mean LSM values were 7.9, 8.8, and 11.7 for F≥2, F≥3, and F=4 (23). When we apply cut-offs 7.9, 8.8, and 11.7 kPa for F≥2, F≥3, and F=4 from the meta-analysis, LSM improvement was also observed in a very similar manner during antiviral therapy compared with our current data. The fibrosis stage was improved in 39 (47.0%) between two LSMs. Thirty six (43.4%) patients showed no change of fibrosis stage, only 8 (9.6%) showed the aggravation of fibrosis stage. Of the 39 (47.0%) patients with LSM ≥11.7 kPa (cirrhosis) at 1st LSM, 17 (43.6%) proved to no longer have cirrhosis (≥1 decrease in fibrosis stage) at 2nd LSM. Taken together, these data indicate that oral antiviral therapy attenuates the extent of liver fibrosis in patients with B-viral liver cirrhosis.
For the assessment of hepatic fibrosis by LSM using Fibroscan, the following important limitation should be considered. The degree of hepatic necroinflammation may affect the LSM value, i.e., the presence of significant necroinflammation can exaggerate the LSM value (24, 25, 26). When we analysed the change of LSM during antiviral therapy with respect to baseline ALT level, the LSM value significantly decreased in high ALT (> ULN×2) group as well as in low ALT (≤ ULN×2) group, indicating that oral antiviral therapy decrease liver stiffness regardless of ALT abnormality in patients with CHB. These results suggest that the decrease in LSM value during oral antiviral therapy is not caused by purely reducing hepatic necroinflammation but at least partially by decreasing hepatic fibrosis. Macronodular cirrhotic architecture or the absence of significant histologic grade may results in false negative LSM (LSM below cutoff level of cirrhosis) for the accurate diagnosis of histologic cirrhosis. The absence or mild histologic grade during oral antiviral therapy in our study might cause lower 2nd LSM value resulting in the underestimation of liver cirrhosis.
Because of retrospective study design, pathologic changes were not verified to confirm the change of LSM in our study. In spite of this limitation, the demonstration of the LSM change in CHB patients on antiviral therapy through repeated measurement of liver stiffness in real life setting provides important clinical implication supporting the usefulness of LSM using Fibroscan for the assessment of fibrosis regression during antiviral treatment. Recently, Marcellin et al. demonstrated that oral antiviral treatment with tenofovir regressed liver cirrhosis in chronic hepatitis B patients (27). Our study provides similar results using repeated LSM measurement instead of repeated liver biopsies in real-life practice setting. Our study result warrants further prospective study to confirm the correlation of LSM and pathologic changes during oral antiviral therapy in CHB patients.
In conclusion, long-term oral antiviral therapy resulted in the improvement of liver stiffness in a substantial portion of patients with CHB. Liver stiffness measurement using transient elastography may be used as a useful clinical tool to evaluate disease progression in CHB patients.




 XML Download
XML Download