

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Because the life of all animals, including humans, is constantly influenced by the environment, time-dependent variations in biological functions, such as circadian or circannual rhythm, are commonly found in animal physiology (1, 2, 3). Interestingly, seasonal variations are frequently observed in metabolism of mammals. The most striking example is the seasonal variation in glucose metabolism in the desert gerbil Psammomys obesus (sand rat), exhibiting nutritionally induced insulin resistance and hyperglycemia (4), which is observed in spring and autumn when the animal is in its natural habitat (5).
Glycemic variation has also been observed in humans. Hemoglobin A1c (HbA1c), which is the product of non-enzymatic glycation of the hemoglobin molecule and reflects the average plasma glucose concentrations over the previous 2-3 months (6), has been shown to exhibit seasonal variations in both type 1 and 2 diabetic patients. For example, seasonal variation in HbA1c was shown in young type 1 diabetic patients in Poland, with the highest values in winter and lowest values in summer (7); in children with type 1 diabetes in the U.K., with lower levels of HbA1c during the summer months (8); in type 2 diabetic veterans in the USA, with its peak during March to April and trough during September to October (9); and in Japanese diabetic patients with type 1 or type 2 diabetes, with the highest values in March and lowest values in August (10). These studies were performed mainly in the northern hemisphere. Intriguingly, a study encompassing multiple geographic regions, including Calgary, Edmonton, Wisconsin, Singapore, and Melbourne, revealed that HbA1c levels in subjects with or without diabetes were lowest during warmer seasons and highest during cooler seasons regardless of hemisphere (11), indicating that temperature or other seasonal factors may influence plasma glucose levels. Because Korea has four distinct seasons, we hypothesized that ambient temperature or season may affect the glycemic control of patients with type 2 diabetes. Therefore, in this study, we examined the association between HbA1c and calendar day and/or ambient temperature in Korean patients with type 2 diabetes who received various types of anti-diabetic treatments.
MATERIALS AND METHODS
Subjects and data collection
We retrieved data from electronic medical records of the Seoul National University Hospital from October 2007 to May 2011. Mean daily temperature data in the Seoul area during the study period were obtained from the Korea Meteorological Administration. The data collected from electronic medical records included age, sex, diagnosis, HbA1c, prescribed medications and residential addresses. In total, we collected 128,284 HbA1c values measured using high performance liquid chromatography (Variant II Turbo, Bio-Rad, San Francisco, CA, USA) from 14,689 patients (Fig. 1). We excluded subjects if: 1) age<30 yr; 2) patients had type 1 diabetes; 3) patients were treated with immunosuppressants, diagnosed with cancer or had been hospitalized during the study period; and 4) HbA1c measurements were made fewer than three times per year. According to these criteria, 10,498 patients and 70,314 HbA1c observations were excluded. Therefore, a total of 4,191 patients (2,211 men and 1,980 women, 65±10 yr old) and 57,970 HbA1c observations were subjected to the final analyses. The patients were classified into four categories arbitrarily determined according to baseline HbA1c: HbA1c<7% (n=1,727); 7%≤HbA1c<9% (n=2,148); 9%≤HbA1c<11% (n=274); and 11%≤HbA1c (n=42). We also divided the patients into five groups based upon the type of anti-diabetic therapy as follows: a group using lifestyle modification alone (n=166), a group using oral anti-diabetic drugs (OADs) (n=3,022), a group using insulin therapy only (n=172), a group using combined therapy of OADs and insulin (n=186), and a group who changed treatment from OADs to add-on insulin therapy or insulin-only therapy (n=645).
Statistical analysis
Statistical analyses were carried out using SAS software (SAS Institute, Cary, NC, USA). First, the time series analysis was used to find seasonality in HbA1c. Next, we performed a Spearman correlation analysis to evaluate the correlation between HbA1c and ambient temperature because neither variable followed a normal distribution. In the time series analysis, monthly mean HbA1c values were determined by averaging the middle 95% of HbA1c values over a one month interval after excluding the upper and lower 2.5% of the values. The time series analysis of monthly mean HbA1c values was modeled as a linear combination of time t, cos t, sin t, ∈1, and ∈2. The coefficient of t represents a linear trend in HbA1c values corresponding to time change. The coefficients of cos t and sin t represent a cyclic patterns in HbA1c variation, such as seasonality. The noise terms ∈1 and ∈2 were derived separately from the first and second autoregressive parts of the time series model and represent the randomness of the HbA1c values. The total time series model was fitted to monthly mean HbA1c and coefficients, and corresponding P values were determined. Time series analyses were conducted separately in the whole patient group and subgroups divided by types of anti-diabetic therapy or baseline HbA1c value. Spearman correlation analysis was performed using a daily mean of the middle 95% of HbA1c values as the response variable. A P<0.05 was considered statistically significant.
RESULTS
Time-series analysis
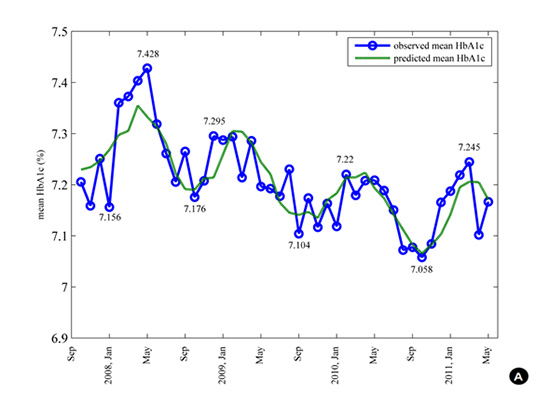
The HbA1c values exhibited a decreasing secular trend over the study period (the coefficient for t=-0.0042, P<0.05) (Fig. 2A and Table 1). Overall, a trend of seasonal variation in the monthly average of HbA1c was observed with highest values from February to March and lowest values from September to October (the coefficient for cos t=-0.0743, P=0.058). The differences between the highest and lowest HbA1c values (i.e., amplitudes) in a year were 0.16%-0.25%. However, a distinct seasonal variation in HbA1c was noticed in the subgroup using OADs only (the coefficient for cos t=-0.0949, P<0.05), indicating that glycemic control was better in the warmer season and worse in the cooler season for this group of patients (Fig. 2B and Table 1).
Correlation between HbA1c and temperature
The Spearman correlation coefficient between daily mean HbA1c values and 3 month-moving averages of daily ambient temperature was measured (Table 2). Overall, the correlation coefficient between these two variables was -0.2154 (95% confidence interval [CI] -0.2711, -0.1580; P<0.05), suggesting that a lower ambient temperature may have a negative influence on glycemic control in patients with type 2 diabetes. In subgroup analysis, however, this negative correlation was not statistically significant in subjects who were treated with lifestyle modification alone or insulin or whose baseline HbA1c was ≥11% (Table 2).
DISCUSSION
We observed a trend in seasonal variation in monthly averages of HbA1c with the highest values in February-March (late winter-early spring) and the lowest values in September-October (early autumn) in Korean patients with type 2 diabetes. Because the HbA1c value mirrors the average plasma glucose levels during the previous 2-3 months (6), these peak and trough HbA1c values reflect the mean plasma glucose levels during the winter and summer seasons, respectively. These results are consistent with previous reports showing maximum values of HbA1c in cooler seasons and minimum values in warmer seasons (7, 8, 9, 10, 11, 12). In addition, the differences between the highest and lowest HbA1c values (i.e., amplitude) in a year were 0.16%-0.25%, which is also similar to the results of other studies, which reported amplitudes of 0.13%-0.45% (7, 9).
We examined the interaction between seasonal variation of HbA1c and types of anti-diabetic therapy or baseline HbA1c levels. Seasonal variations in HbA1c were observed only in patients who were treated with OADs, and this was not affected by baseline HbA1c values. It is of interest that HbA1c was not affected by ambient temperature in patients who were treated with either lifestyle modification alone or insulin. Perhaps this lack of effect means that glycemic control in relatively well-controlled type 2 diabetes is not affected by ambient temperature. In addition, patients using insulin therapy may effectively respond to the altered glycemic control by adjusting their insulin dosage. However, seasonal variations in HbA1c were also reported in healthy women (13) or patients who were treated with insulin (7, 9). Therefore, we cannot guarantee that patients who are treated with either lifestyle modification alone or insulin are less susceptible to seasonal changes in glycemic control. Furthermore, because the number of the patients in these subgroups was relatively small, we may have missed the actual signal of seasonal variation.
Although seasonal variations in HbA1c have been reported by several independent researchers (7, 8, 9, 10, 11), the mechanism underlying this phenomenon is still not definite. Our study was primarily concerned with the correlation between HbA1c and ambient temperature and the impact of sun exposure or different levels of physical activity in glucose homeostasis has not been considered. Nonetheless, serum 25-hydroxyvitamin D concentration, which is affected by exposure to ultraviolet light (14), or serum melatonin concentration, which is dependent on photoperiod (15), could play an important role. It was reported that vitamin D deficiency may increase insulin resistance and the risk of metabolic syndrome (16, 17, 18). Therefore, a lower serum level of 25-hydroxyvitamin D during the winter season (19) may aggravate glycemic control. Melatonin production is highest at night (20), and some studies reported seasonal variations in human melatonin production with increased levels in winter (15, 21). It was reported that the nighttime increase in melatonin was associated with rises in circulating glucose levels and reduced insulin sensitivity (22). However, there are studies showing that a lower level of melatonin was associated with development of type 2 diabetes (21, 23). Therefore, further studies are needed to examine the role of melatonin in the seasonal variations in HbA1c particularly in patients with type 2 diabetes.
Aside from seasonal biological variations, cultural events or food availability may influence the seasonal variability in HbA1c. In a Chinese study examining HbA1c during the Chinese New Year's holiday, mean HbA1c was increased by 0.094%±0.828%, most likely due to decreased physical activity, increased intake of foods and/or increased consumption of alcoholic beverages (24). In addition, there is a tendency for increased intake of animal fat-containing foods and decreased physical activity in winter (25, 26, 27). Furthermore, it was reported that body mass index and waist circumference were higher in winter than in summer (28), which could be explained by changes in calorie intake and physical activity. These non-biological factors should be considered when evaluating seasonal variations in HbA1c because these factors could be modified by education and counseling.
Of interest, there was a decreasing secular trend of monthly averaged HbA1c values over time during the study period, as depicted in Fig. 2. This trend reflects the movement towards stricter glycemic control for patients with type 2 diabetes, which was supported by compelling evidence for the "legacy effect" of intensive glycemic control from the initial diagnosis of type 2 diabetes based on long-term follow-up in the U.K. Prospective Diabetes Study (29). Additionally, the Korean Diabetes Association recommended a target HbA1c level of <6.5% in November 2007 (30), and this more stringent target level may have resulted in an improvement in HbA1c values during the study period.
There are some limitations and strengths in our study. As mentioned earlier, we did not measure the level of sun exposure or physical activity, which may affect glucose homeostasis in patients with type 2 diabetes. The lack of data on 25-hydroxyvitamin D and melatonin prohibited us from examining the association between these hormones and glycemic control. However, the strength of our study is that we included more than 4,000 type 2 diabetic patients with HbA1c values measured on a regular basis by a standardized method in a single institution over 4 yr, which allowed us to examine the seasonal variation according to the different types of anti-diabetic therapy.
In conclusion, we observed a trend in seasonal variation in HbA1c in Korean patients with type 2 diabetes, particularly in the OAD-treated patients. Although the mechanism underlying this phenomenon is yet to be elucidated, stricter adherence to lifestyle modification and frequent assessment of glucose control appear to be necessary during the winter season to prevent aggravation of hyperglycemia in patients with type 2 diabetes.


 XML Download
XML Download