

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary heart disease (CHD) is one of the leading causes of death in both high- and low-income countries (1). The increased prevalence and mortality associated with the large burden of CHD is a reflection of the epidemiological transition that has accompanied economic and social development (2). Numerous studies show that the socioeconomic status (SES) is associated with a risk of CHD (3, 4, 5, 6). There was the definite relationship between the low SES and the predicted risk of ischemic heart disease (IHD) (7). Also, both individual SES and the SES of the neighborhood of residence are independently associated with the incidence of acute myocardial infarction (AMI) (8, 9).
The association between SES and outcomes of AMI is generally well documented in western countries (10, 11, 12). Therefore, the measures of SES have been identified as the risk factors after AMI (13, 14). However, because the SES is a multidimensional concept comprising various indicators acting at different levels, the mechanisms by which it affects post-AMI prognosis are incompletely understood (15, 16).
The objective of this study was to investigate whether the SES variables independently contribute to 3-yr clinical outcomes in Korean patients with AMI who underwent percutaneous coronary intervention (PCI).
MATERIALS AND METHODS
Study design
This was a retrospective cohort observational study of 2,700 AMI patients who admitted to Chonnam National University Hospital between November 2005 and June 2010. Among the patients, 2,358 eligible patients (64.9 ± 12.3 yr old, 71.5% male) who underwent PCI were sorted according to the level of education and followed-up during 3-yr. The medical records of all patients were reviewed and the patients' clinical data were collected. The patients were followed-up in order to find out whether they were still alive. All patients were contacted by telephone. In each successful contact, either patient or a close relative (wife or husband, son or daughter, parents, and sister or brother) were interviewed. If the patient be found, it was regarded as censoring.
AMI was defined as the elevated cardiac biomarkers (troponins or creatine kinase MB fraction) with ischemic symptoms or electrocardiographic findings indicative of ischemia and was further classified by the ST-segment change. ST-elevation myocardial infarction was defined as new ST elevation in at least two contiguous leads, measuring >0.2 mV in leads V1-V3, or >0.1 mV in all other leads or presumably new-onset left bundle branch block (17). All other electrocardiographic patterns, including ST-segment depression or T-wave inversion, were diagnosed as non-ST-elevation myocardial infarction.
Diagnostic angiography and PCI were performed after the premedication with aspirin (at least 100 mg) and the unfractionated heparin (from 50 to 70 U/kg). Loading of clopidogrel (from 300 to 600 mg) was done before PCI. Coronary angiography was performed through the femoral or radial artery. Heparin was infused throughout the procedure to maintain an activated clotting time of at least 250 sec. Stents were deployed after prior balloon angioplasty and administration of platelet glycoprotein IIb/IIIa-receptor blocker was left to the decision of each cardiologist.
Socioeconomic measures
SES was measured by the self-reported educational level, the residential address, and the national health insurance status. Individual SES data were self-reported at the index hospitalization and included the following variables: education (years of schooling) and national health insurance status (medical aid beneficiaries). The study group was divided into 3 groups according to the years of schooling (lower group, ≤6 yr; middle group, 7-12 yr; upper group, ≥13 yr).
Neighborhood SES was estimated through a social deprivation index (SDI) by the report of Health Promotion Strategies and Programmes Development for Health Inequalities Alleviation (18). The index, which is based on the 2005 National Census data (19), is a summary of numerous socioeconomic measures (ratio of living environment instability, elderly population, low educated population, low social class per household, apartment resident, households without cars, household alone, and female-headed household). The neighborhood SES was classified into three levels of SDI: lower (less than the lowest tertile of SDI), middle (the lowest tertile to the middle tertile), and upper (greater than the highest tertile).
Demographic and clinical variables
Demographic and clinical characteristics recorded were gender, age, and medical history. The latter included any history of current smoking, drinking, hypertension, diabetes mellitus, dyslipidemia, previous IHD, family history of heart disease, time of symptom onset, and Killip classification.
Current smoking was defined as self-report of active smoking within the last year before the admission. Drinking was defined as the consumption of an alcoholic beverage (1 unit) at least one times per week. The hypertension was defined as systolic blood pressure >140 mmHg and/or diastolic blood pressure >90 mmHg at rest, at repeated measurements, or treatment with anti-hypertensive medications. The diabetes mellitus was defined as a fasting plasma glucose levels ≥126 mg/dL or 2-hr postprandial plasma glucose readings ≥200 mg/dL. The dyslipidemia was defined as low-density lipoprotein cholesterol concentration of >140 mg/dL and/or triglyceride concentration of >150 mg/dL and/or high-density lipoprotein cholesterol concentration of <40 mg/dL in male and <50 mg/dL in female and/or the use of treatment with medication for dyslipidemia. The coronary angiographic lesion characteristics were classified according to the criteria of the American College of Cardiology/American Heart Association (ACC/AHA) (20). The degree of coronary flow was classified using Thrombolysis In Myocardial Infarction (TIMI) score (21).
Outcome measures
The primary study endpoints were the composite of major adverse cardiovascular events (MACEs) and mortality during the three years of clinical follow-up. The former included a composite of all-cause death, recurrent AMI, and repeated PCI or coronary artery bypass graft. Recurrent AMI was defined as the recurrence of symptoms or new electrocardiographic changes compatible with AMI in association with a rise in cardiac enzymes at least twice the upper limit of normal. Repeated PCI included target lesion revascularization and target vessel revascularization.
Statistical analysis
The analyses were performed with SPSS for Window, version 17.0 (SPSS Inc., Chicago, IL, USA). The baseline clinical characteristics across educational levels were compared by the chi-square test for categorical variables (expressed as percentages) and ANOVA for continuous variables (expressed as mean±standard deviation). The statistical significance was generally defined as a 2-tailed P value of less than 0.05.
The survival across SES variables was assessed by the Kaplan-Meier method with right censoring at the time of last follow-up and compared by the log-rank test. The Cox proportional hazards models were constructed to evaluate the hazard ratio and 95% confidence interval for MACEs and mortality associated with SES variables. The proportional hazard assumptions were examined by inspecting log minus-log survival plots, with no violations detected. The initial adjustment was made for age, sex, hypertension, diabetes mellitus, dyslipidemia, current smoking, drinking, previous IHD, and family history of heart disease. Subsequently, the additional adjustment was performed for Killip class, multivessel disease, ACC/AHA lesion types, drug-eluting stent, and post-procedural TIMI flow grade.
RESULTS
Baseline clinical characteristics of the subjects
Of the 2,358 patients, 1,686 (71.5%) were male and 672 (28.5%) were female. The mean age of the sample was 64.9±12.3 yr old (62.0±12.0 yr old in male, 72.2±9.7 yr old in female). The mean follow-up period was 823±389 days with the loss of follow-up (321 patients) for MACEs and 920±332 days with the loss of follow-up (356 patients) for mortality. The loss of follow-up was a censored observation for the analysis.
The patients of female were residing in upper-SDI area and higher prevalence of medical aid beneficiaries, hypertension, diabetes mellitus, and higher Killip class. The male patients had higher prevalence of drinking, current smoking, family history of heart disease than female patients (Table 1).
The patients of lower group were generally older and predominantly female. They also had higher prevalence of hypertension and diabetes mellitus and had severe disease, as indicated by higher Killip class and more frequent previous history of IHD compared with upper group patients. The patients of lower group were residing in upper-SDI area and higher frequency of medical aid beneficiaries (Table 2).
No significant differences in the coronary angiographic and procedural characteristics were found between the groups, except that the lower group had a higher incidence of multivessel disease and more frequent implantation of bare-metal stent (Table 3).
Unadjusted effect of educational levels on three-year MACEs and mortality
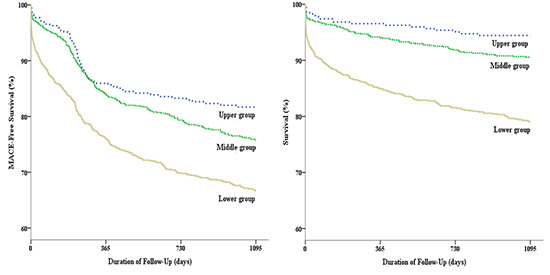
The mortality rate and incidence of MACEs were significant differences among the three groups during 3-yr follow-up. During the 3-yr follow-up period, MACEs occurred in 344 patients (32.3%) in the lower group, 223 patients (23.6%) in the middle group, and 63 patients (18.1%) in the upper group (P<0.001). An all-cause death occurred in 216 patients (20.3%) in the lower group, 87 patients (9.2%) in the middle group, and 19 patients (5.4%) in the upper group (P<0.001) (Table 4).
Fig. 1 showed unadjusted Kaplan-Meier survival curves for MACEs and mortality by the education level groups. The lower group had higher MACEs and mortality in patients with AMI who underwent PCI.
Independent predictors of three-year MACEs and mortality including clinical and angiographic variables
Cox regression analyses were then conducted to determine which variables were predicted 3-yr MACEs and mortality in patients with AMI who underwent PCI. All variables confirmed by bivariate analyses were entered in the analysis. The independent predictors of MACEs were found to be an old age, previous IHD, diabetes mellitus, Killip class≥3, multivessel disease, post-TIMI flow grade≤1, and lower education. The independent predictors of mortality were found to be an old age, Killip class≥3, post-TIMI flow grade≤1, and lower education (Table 5).
Multivariable model of SES on three-year MACEs and mortality
The multivariable-adjusted associations of various SES determinants with MACEs and mortality are shown in Table 6. The only education of individual SES indicators out of various SES variables was strongly associated with 3-yr MACEs and mortality in the patients with AMI who underwent PCI (model 1). Furthermore, the association of most of these measures persisted even on the simultaneous adjustment for coronary angiographic and procedural characteristics (model 2). However, the SDI of neighborhood SES indicators was not significant for the incidence of MACEs and mortality in the patients with AMI who underwent PCI.
DISCUSSION
The results of this study indicated that the lower education of individual SES indicators was associated with a trend toward worse the 3-yr clinical outcomes in patients with AMI who underwent PCI. However, the SDI of neighborhood SES indicators and the economic status were not associated with the outcomes after adjustment of clinical and angiographic variables.
SES was a commonly used concept in health research. This factor has been shown to be associated with other established medical risk factors that contribute to further increase cardiovascular risk (22). There was no single best indicator of SES suitable for all study aims and applicable at all time points in all settings. Each indicator measures different, often related aspects of socioeconomic stratification and may be more or less relevant to different health outcomes and at different stages in the life course. Therefore, the SES of the individual was multidimensional, and the dimensions most relevant to health differences are considered to be education, occupational social class and income (23).
Gerber et al. (24) reported that the neighborhood SES was strongly associated with long-term survival after AMI. Also, the neighborhood effects can be related to the characteristics of the social environment, which include the social norms and prevailing attitudes toward the health and health-related behavior and features of the social connections within neighborhoods such as social cohesion and support (25). Such connections may lead to better sharing of health-related information and expertise gained from experience with the healthcare system. However, our results demonstrated that the neighborhood SES as measured by SDI was not associated with the outcomes in the patients with AMI who underwent PCI.
The income was the indicator of SES that most directly measures the material resources component. Also, the income level was associated with worse outcome among the patients with acute coronary syndromes (26). The result of our study showed that the income level as measured by medical aid beneficiaries demonstrated a correlation with mortality rate in the patients with AMI who underwent PCI. However, the effect was attenuated by adjust for demographic and clinical variables.
The educational level was normally completed in young adulthood and strongly determined by parental SES, which in turn contributes to a person's social class, income, and knowledge, all of which were interwoven with other non-material resources that were likely to have an impact on the health. The knowledge and skills attained through education may affect a person's cognitive functioning, make them more receptive to health education messages, or more able to communicate with and access appropriate health services. Furthermore, the education was most often used, because it was easily obtained and also frequently treated as a proxy for SES overall (27). The education was comparatively easy to measure in self administered questionnaires, garners a high response rate, and was relevant to people regardless of age or working circumstances, unlike many other SES indicators (28). In addition, the collection of information on the education may be less contentious in some contexts than other SES indicators. However, there may be heterogeneity between the education level and the health outcomes across different populations within specific countries. For example, the risk for AMI increased with higher education in the black African group in the INTERHEART African substudy but the opposite was observed in coloured and white Africans (29). Nevertheless, our findings suggest that lower education was the SES marker most consistently associated with increased incidence of MACEs and mortality in the patients with AMI who underwent PCI.
The failure to identify the symptoms correctly was associated with the lower education, which was found to be a predictor of prehospital delay in previous study (30). The patients who present with atypical symptoms are frequently misdiagnosed, and less likely to receive optimal treatment for AMI. Consequently, the greater morbidity and mortality are noted. This finding might be explained by old age and lower education compared to typical symptoms patients (31, 32). Because the education were easily ascertained and frequently used as proxies for SES, these variables can be used to screen for high-risk groups, especially among the patients with AMI who underwent PCI. Therefore, our findings indicated the importance of enhancing preventive/rehabilitative healthcare services for post-AMI patients with lower education.
Our study had several strengths. Firstly, this study was the complete enrollment of all comers of the patients who were hospitalized with independently confirmed AMI and the use of relatively recent data that reflect the current medical practices. Secondly, our study was the first to evaluate the roles of individual-level and neighborhood-level SES measures in post-AMI prognosis. Finally, this study could contribute to existing literature on the topic and also could provide the evidence for better understanding of social determinants of health in general and the issue of health equity in particular in Korea and perhaps in other developing countries of similar conditions.
There were several limitations to the present study. Firstly, because of an observational registry study, there were the baseline differences in several important prognostic factors between our primary comparison groups. The limitation of propensity score matching is that many unmatched samples are excluded from analysis, resulting in loss of data which may reduce the precision of the estimated association between the SES factors and outcomes. Thus, we included most confounders in the multivariable Cox regression model. It is possible that some potential confounders might have crept in. Secondly, although we have measured SES more directly by using individual-level measures and more comprehensively by looking at multiple measures than many previous studies, there are facets of SES that we did not include, such as measures of wealth and occupational class that might provide a more comprehensive picture of social class. Thirdly, we did not include additional factors that might confound the relationship between SES and rehospitalization and mortality, specifically the behavioral or lifestyle factors such as diet, substance use, or adherence to medications; the mental health factors such as depression; and additional comorbidities. Fourthly, although we assessed risk factors at the time of the index event, we could not reliably measure how long the risk factors had been present before the AMI. Fifthly, our study cohort was comprised of the patients with AMI who underwent PCI. Therefore, our results may not be applicable to the general population of the patients with AMI. Finally, this study only included a patient population admitted to a single hospital. So, the future studies should also investigate about the patients who admitted in multicenters.
The study results indicated that the lower education was a significant associated factor to increased MACEs and mortality in patients with AMI who underwent PCI. This work also highlights the need for continued investigation of the specific means by which SES affects a variety of health outcomes, as the mechanisms vary by disease process and outcome.






 XML Download
XML Download