

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Severe congenital neutropenia (SCN) is a disorder of neutrophil production predisposed to recurrent and severe bacterial infection from early infancy. Although many genetic aberrations responsible for this condition were reported, SCN largely derives from ELANE gene mutations which are known to be correlated with more severe neutropenia and serious clinical manifestations in SCN. ELANE gene mutations are also identified in patient with cyclic neutropenia (CN). Although types of ELANE mutation largely differ among these diseases, specific mutations were associated with both SCN and CN in unrelated patients and in patients with a shared haplotype by a sperm donor, but not in the same family (1, 2). We described inherited SCN cases showing different disease severity with the same mutation of the ELANE gene in a Korean family.
CASE DESCRIPTION
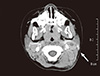
A 17-month-old Korean girl (patient 1) was admitted to the department of otolaryngology, Gachon University Gil Medical Center, with mild fever and neck swelling in January 2013. On admission, laboratory findings were as follows: leukocytes 7,600/µL (segment neutrophil 7%, lymphocyte 55%, monocyte 35%), absolute neutrophil count (ANC) 532/µL, hemoglobin 12.4 g/dL, platelet 459,000/µL, and C-reactive protein 3.06 mg/dL. The computed tomography of her neck showed multiple enlarging lymph nodes with some necrotic changes in her left neck lymph node level II and V involving overlying skin, subcutaneous tissues and paraspinal muscles on the left (Fig. 1). She was treated by incision and drainage under local anesthesia and by empirical antibiotics. On the 10th hospital day, she showed fever and persistent swelling on her neck, and methicillin-resistant Staphylococcus aureus was isolated on the pus drained from cervical lymph node. She was transferred to the pediatric department.
She was born by cesarean section delivery with a birth weight of 3.38 kg at full term. She had a history of admission and operation because of peritonitis complicating perforated appendicitis with Pseudomonas aeruginosa sepsis at 8-months of age. Her ANCs have been lower than 500/µL, and generally lower than 200/µL since then. In her family history, her second elder sister (patient 2) was getting evaluations due to persistent neutropenia in our pediatric hematology clinic. Her mother (patient 3) had had severe recurrent oral ulcers until her early 20s but had not known about her neutropenia. Her eldest sister and her father had not had any oral ulcers, lymphadenitis or netropenia (Fig. 2).
Patient 2, a 37-month-old Korean girl, had a medical history of recurrent oral ulcers and persistent neutropenia (< 200/µL) and several times of hospitalization for treatment of cervical lymphadenitis, pneumonia and oral ulcers with fever. She underwent bone marrow aspiration and biopsy three days before her sister's admission (patient 1). Her ANC was also low (162/µL) on the day of the bone marrow examination, and serum immunoglobulin G, A, and M levels were normal, and chromosome analysis showed normal female karyotype (46, XX). Her bone marrow finding showed myeloid hypoplasia with maturation arrest at the promyelocyte stage (Fig. 3).
Patient 3, a 32-yr-old Korean woman, had also showed neutropenia (ANC 329/µL). She had had severe recurrent oral ulcers until her early 20s. However, her stomatitis has no longer recurred after her marriage.
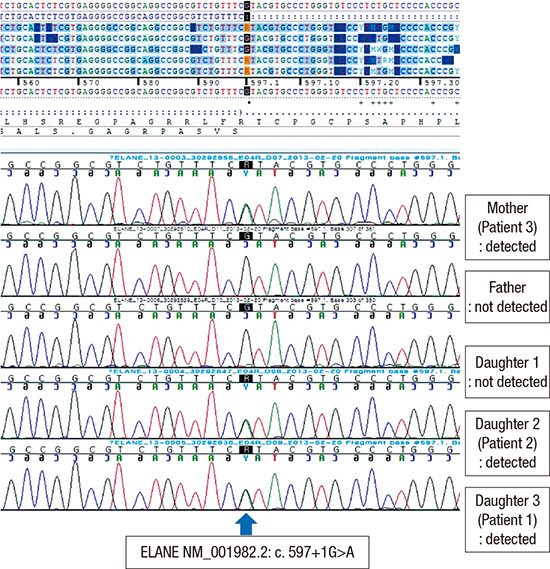
Considering the clinical courses and hereditary patterns of the two young girls and their mother, autosomal dominant congenital neutropenia was strongly suspected. Direct DNA sequencing analyses of the ELANE gene on chromosome 19p13.3 were performed on this family. The mutational analyses demonstrated substitution of the 597th base (G to A) in intron 4 (c.597+1G>A) on patients 1, 2, and 3, with negative study on their father and their eldest daughter (Fig. 4).
Despite administration of vancomycin for 7 days to patient 1, enlarged lymph nodes and inflammatory changes around lymph nodes did not improve. From the 17th hospital day, we started administration of subcutaneous 5-10 µg/kg/day granulocyte colony stimulating factor (G-CSF). Although we gradually increased the dose of G-CSF up to 25 µg/kg/day, her lesion remained unchanged until excision under general anesthesia. After her discharge, she needed hospitalization twice more for 5 months due to stomatitis and severe acute otitis media, respectively. Patient 2 had three episodes of stomatitis with fever for 5 months. Despite administration of G-CSF 5-10 µg/kg, her ANC was also lower than 500/µL. Her mother has had no fever and oral ulcer since then.
DISCUSSION
Severe congenital neutropenia (SCN) refers to a variety of disorders of neutrophil production characterized by recurrent and severe bacterial infections, with ANC consistently below 200/µL (3). Severe bacterial infections frequently occur during the first year of life in children with SCN. Omphalitis, beginning directly from birth, may be the first symptom, but otitis media, pneumonitis, infections of the upper respiratory tract, and abscesses of skin or liver are also common. Most patients suffer from frequent aphthous stomatitis and gingival hyperplasia, leading to early loss of permanent teeth. The most common pathogens causing infections in neutropenic patients are S. aureus and gram-negative bacteria. The absence of pus in SCN is a characteristic feature because of the inability to form pus (4). Patient 1 in this report showed prolonged local inflammation on adjacent muscles, overlying skin and soft tissues instead of significant abscess formation as the CT finding previously demonstrated (Fig. 1).
SCN is a genetically heterogeneous syndrome associated with mutations of ELANE (ELA2), HAX1, GFI1, WAS, CSF3R or G6PC3, etc. (5). Genetic transmission may be either autosomal dominant or recessive, with many more sporadic than inherited cases reported (2). In recent studies, it is reported that 60%-80% of inherited or sporadic cases are attributable to mutations in the ELANE gene, which encodes neutrophil elastase (NE) (2, 3). Neutrophil elastase is a chymotryptic serine esterase synthesized early in myeloid development, during myeloblast-to-promyelocyte transition (6). The mutant NE likely induces accelerated apoptosis in differentiating myeloid cells. One of the proposed mechanisms to accelerate apoptosis of granulocytic precursors is cytoplasmic accumulation of a nonfunctional misfolded NE protein in the endoplasmic reticulum (ER), subsequent activation of the unfolded protein response, and cell death from ER stress-induced apoptosis (7, 8). Therefore, bone marrow examination characteristically shows maturation arrest of neutrophil precursors at the promyelocyte/myelocyte stage of development.
The ELANE gene is located in chromosome 19p13.3 and consists of five exons and four introns, spanning approximately 5,000 base pairs of genomic DNA (9). The mutations of ELANE gene have been found in SCN cases, but more often in cyclic neutropenia (CN) cases as well (2). Cyclic neutropenia is characterized by regular oscillations of peripheral blood neutrophils from near normal to severely low levels, generally with 21-day periodicity. While SCN and CN are currently classified as two distinct diseases, some authors suggest that SCN and CN represent phenotypes on a disease spectrum and CN is generally considered milder than SCN (2).
Although studies have suggested a relationship between individual ELANE mutations and disease severity, a more general genotype-phenotype correlation has not been established. Rather, some authors have reported that patients with a shared ELANE mutation by sperm donor had SCN and CN phenotypes (2). More than 100 mutations in the ELANE gene have been found in SCN patients (10). The mutation detected in our cases was a substitution of the 597th base (G to A) in intron 4 (c.597+1G>A) of the ELANE gene. This splice site mutation leads to deletion of Val190-Phe199, which is the mutation firstly reported in CN patients (11). Three patients in this report had the same mutation of the same gene in the same family but revealed different degrees of the disease severity. Patient 1 had two distinct episodes of bacterial infection including life-threatening sepsis and peritonitis despite with moderate neutropenia, while patient 2 has had only recurrent oral ulcers and cervical lymphadenitis with more severe neutropenia below 200/µL. Patient 3 has not had any stomatitis, lymphadenitis or other significant infection despite with severe neutropenia since her early 20s.
For treatment of SCN, G-CSF is the treatment of choice since 1987. The Severe Chronic Neutropenia International Registry (SCNIR) reported that more than 95% of patients responded to G-CSF treatment with an increase in ANCs to ≥1,000/µL. Most SCN patients responded to a dose between 3 and 10 µg/kg/day. There were some reports of Korean children with SCN treated with G-CSF, while Shim et al. reported a SCN infant with an ELANE mutation unresponsive to G-CSF (12-14). For patients who do not respond to G-CSF, hematopoietic stem cell transplantation is the only currently available treatment (3).
In addition, approximately 20% of patients with SCN develop myelodysplasia (MDS) or acute myeloid leukemia (AML) (15). There was no correlation between distinct ELANE mutations and malignant transformation (10). The risk for MDS/AML was correlated with disease severity rather than with occurrence of an ELANE mutation (10). In recent analyses, the influence of the G-CSF dose required to achieve neutrophil response (ANC >1,000/µL) in the risk of developing acute myeloid leukemia (AML) has been reported. Less responsive patients, defined as those requiring greater than 8 µg/kg/day of G-CSF, had a cumulative incidence of MDS/AML of 40% after 10 yr, compared to 11% of more responsive patients (16). Since patients 1 and 2 did not respond to G-CSF, even at some high dose, we could consider stem cell transplantation as their treatment. However, because they are very young and patient 2 has had only recurrent stomatitis even with severe neutropenia near zero, we will closely follow them up.
In this report, the patients revealed different clinical phenotypes from life-threatening infections to no symptoms regardless of ANCs despite the same ELANE mutation in the family. It is suggested that the disease phenotype is not determined by the mutation alone and other factors can contribute to clinical features of patients. Further studies are needed to define the influence of genetic, epigenetic, or environmental factors.



 XML Download
XML Download