

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteogenesis imperfecta (OI) is a heterogeneous group of diseases characterized by congenital bone fragility, low bone mass, subsequent development of the spine and limb deformities. In majority of the OI patients, type I collagen in the bone tissue as well as other connective tissues are quantitatively deficient or qualitatively defective by mutations of COL1A1/COL1A2 or enzymes involved in the synthetic process of type I collagen.
LT itself has a high risk of bleeding during the perioperative period, and requires mechanical retraction for the surgical field. Bleeding tendencies and bone fragility secondary to tissue and capillary fragility and platelet dysfunction of OI patients can make these problems worse. The worrisome anesthetic implication of OI is the possibility of malignant hyperthermia mimicking events. Herein, we report a case of living donor liver transplantation (LDLT) for an eight-month-old boy with OI and cholestatic biliary cirrhosis under intravenous anesthesia. This is the first case report of a successful LT in a patient with OI.
CASE DESCRIPTION
A one-month-old male infant was transferred to the Seoul National University Children's Hospital because of neonatal cholestasis and bone fragility on December 29, 2011.
Diagnosis of OI
Fibular fracture and bilateral bowing of the femora were noticed just after birth. And right femur shaft fracture, left humerus fracture and left femur fracture occurred at 1, 2, and 3 months of age respectively (Fig. 1). He showed blue sclerae with a triangular face and his father showed the OI type IB. In mutation analysis for COL1A1 and COL1A2 encoding alpha 1 and 2 chains of type I collagen (MIM 120150 and 120160), a novel heterozygous mutation c.1036-2A > C, (of IVS19) in COL1A2 was identified in both the patient and his father.
Cholestatic liver failure
At one month after birth, he developed white stool and abdominal distension. Liver function tests were abnormal; total bilirubin 7.3 mg/dL, AST 128 IU/L, ALT 82 IU/L, alkaline phosphatase 386 IU/L, albumin 4.0 g/dL, prothrombin time (PT, INR) 1.04, platelet 853 × 103/µL. The screening tests for metabolic diseases were normal. Viral markers for hepatitis A, B, C, and TORCH were all negative. Ultrasonography was incompatible with biliary atresia. Liver biopsy showed cholestasis with periportal fibrosis and damaged bile ducts without definite cause. At the seven month follow-up, his liver function had deteriorated (total bilirubin 19.3 mg/dL, direct bilirubin 12.9 mg/dL, AST 211 IU/L, ALT 165 IU/L, albumin 3.0 g/dL, PT INR 1.09, Platelet 254×103/µL). His CTP score was 9 and pediatric end stage liver disease (PELD) score was 13. Preoperative dynamic liver CT revealed hepatomegaly with surface nodularity and splenomegaly. Because his cholestasis had begun in infancy and had progressed to cirrhosis within seven months, progressive familial intrahepatic cholestasis (PFIC) was suspected. But abnormality was not detected in PFIC type III gene. Body weight was 7.9 kg (10th percentile) and height was 69.6 cm (20th percentile) at the time of LT.
Preparation of LT
Before surgery, the patient was treated with pamidronate infusion therapy (1.5 mg/kg per each cycle) for 4 cycles with vitamin D and calcium medications. His dual energy X-ray absorptiometry (DEXA) bone density showed 0.254 g/cm2 in spine L1-4, 0.301 g/cm2 in femur neck, and 0.393 g/cm2 in femur total after 3rd cycle of pamidronate therapy before LT. These values were comparable to reference values (1-3).
LT and postoperative care
LT was performed at the age of 8 months using the left lateral section from his mother under intravenous anesthesia because of the risk of malignant hyperthermia. An endotracheal tube was inserted smoothly under laryngoscopy without a difficult airway related with neck extension. There was no intractable metabolic acidosis during and after LT. Hyperthermia did not develop during the operation.
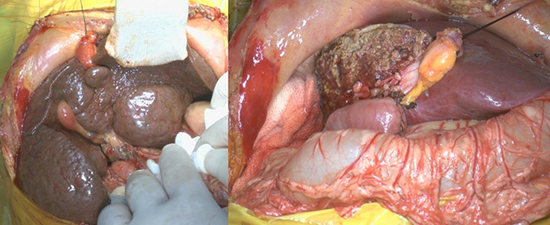
The graft weight was 215 gm and a graft versus recipient weight ratio was 2.72%. The retractors were not used because of high risk for rib fracture. Instead of that, skin was fixed to upper lateral portion in the chest wall with sutures to form the operation field (Fig. 2). The operation lasted for 420 min; cold ischemic time - 78 min, warm ischemic time - 24 min. Hepatic vein was anastomosed via piggyback method with strengthened fencing venoplasty. The recipient's main portal vein was anastomosed to the graft portal vein. The hepatic artery was anastomosed under a surgical microscope (×10). And hepatico-jejunostomy was done. The estimated blood loss was 530 mL. One unit of leukocyte depleted packed red blood cell was transfused during operation.
Hyperthermia developed up to 40℃ on postoperative day (POD) one, and went down within normal range at POD 2 without any cause. A newly developed fracture line of his right humerus shaft was detected at POD 2 (Fig. 3), but it healed under conservative treatment. He was transferred to the general ward from intensive care unit at POD 10 and discharged at POD 15. The pathologic report of the explant liver was secondary biliary cirrhosis, damaged interlobular bile duct, bile duct proliferation with cholestasis and septal fibrosis. He remains well on follow-up 9 months later at the outpatient clinic.
DISCUSSION
The prevalence of OI is between 1 per 10,000 and 1 per 20,000 (4). It is subdivided into eight types. This patient may be type III or type IV of OI according to his clinical manifestations and the identified mutation in COL1A2 (5).
Until now, there is no report about hepatic cholestasis in a patient with OI, but it was life threatening for him. We suspected PFIC type III in the aspect of his fatal status and liver cirrhosis development within a year of presentation. And its gene abnormality, MDR3/ABCB4 defect, is located on chromosome 7q21.1. Because its location is close to OI type III COL1A2 gene abnormality on 7q22.1, their relation was doubted. But, the gene study for PFIC type III showed no abnormality. The cause of cholestatic hepatic failure for this patient needs to be studied furthermore.
Although there has been no report of LT for the patient with OI, multiple obstacles have been known in vascular or orthopedic surgery; bleeding tendency, cervical and rib fragility, and hyperthermia associated with the conventional inhalation anesthesia (6, 7). And another problem was lactic acidosis under the intravenous anesthesia with propofol (8).
With a planned strategy via multidisciplinary team approach, we could overcome these problems. Because of bleeding tendency for OI patients, operator and assistants manipulated tissues and vessels carefully and bleeding is controlled fastidiously. We only fixed the flap of his abdominal wall to the chest wall without mechanical retractors in order to avoid the possibility of rib fracture (Fig. 2). In this case, we used vascular interposition fencing flap using donor's left ovarian vein for anastomosis of the hepatic vein to the IVC in order to strengthen anastomosis site and to make a big outflow tract (9). And cooperation with plastic surgery for microscopic anastomosis of hepatic artery was successful.
All the tubes were washed and connected with a mechanical ventilator to decrease the risk for hyperthermia before LT. Intravenous anesthesia was well maintained during the full process of LT for 500 min. As Reed et al. (10) emphasized careful use of propofol in critically ill infants and children because of the development of propofol infusion syndrome with metabolic acidosis. We monitored the changes of lab findings carefully and metabolic acidosis did not developed.
Supportive therapies were aimed to increase the overall bone strength to prevent fracture and maintain mobility to succeed a long-lasting operation and post-transplant care. In this present case, the bone mineral density (as measured by DEXA) recovered within normal range for Korean children after 3 cycles of pamidronate therapy before LT. Although the bone could not recover to full strength with pamidronate, cyclic pamidronate therapy is effective in improving bone mineral density and reducing fracture risk during childhood in patients with OI (11) (12). Therefore, we continued cyclic intravenous pamidronate therapy after LT; the 5th pamidronate infusion therapy (1.5 mg/kg) was done for 3 days at POD 30. A fracture of the right humerus sustained at POD 2 was treated conservatively without any residual deformity.
Because life span was expected to normal in patients with OI type III or IV, LT was performed for him. Although there were obstacles to get over for a successful LT, we did LT with multidisciplinary teamwork. However, the cause of his cholestatic liver disease was not revealed, postoperative monitoring for possible causes as well as recurrence of original disease is needed (13).
In conclusion, the operative risk for rib fractures and vascular fragility could be overcome with preoperative pamidronate infusion therapy, omission of mechanical retractors replacing with skin traction, meticulous surgical techniques, and planning the operation. Intravenous anesthesia during full coverage of all process during operation was successful. Therefore, LT should be considered for patients with end stage liver disease and OI via multidisciplinary team approach.



 XML Download
XML Download