

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In 1962, two university hospitals in Korea set up intensive care units (ICUs) as postoperative respiratory care units. Since then, the number of ICUs has continued to increase. When the Korean Society of Critical Care Medicine (KSCCM) was organized in 1980, 18 university hospitals and nine general hospitals had ICUs. Compared with other medical fields, the quality of critical care has lagged behind that of advanced countries. Moreover, the level of critical care quality differs significantly between university hospital ICUs (1).
To analyze the problems in critical care, the first step is to know the current status of critical care at the national level. Little information is available on critical care delivery in Korea. The purpose of this study was to clarify current problems related to ICU organization, critical care-giver staffing, and the characteristics of patients admitted to an ICU.
MATERIALS AND METHODS
Questionnaire survey
In the autumn of 2009, a questionnaire prepared as an official document of the KSCCM was distributed to the critical care physicians in all 105 critical care subspecialty training hospitals. The collected data were specific to the individual ICU rather than the hospital, and included ICU type, number of ICU and hospital beds, any association with a medical school, and nurse and physician staffing levels. We categorized ICUs as medical, surgical, pediatric, neurologic, emergency, coronary care units (CCUs), or mixed (not classified on the basis of patient characteristics). A dedicated physician was defined as a medical doctor who worked in an ICU more than 8 hr a day as a trainee or specialist. Patient information included age, length of stay, ICU admission source, ICU admission diagnosis, receipt of mechanical ventilation, vasoactive or inotropic drugs, blood transfusion(s), invasive monitoring, and cardiopulmonary resuscitation (CPR). Some survey data (including number of nursing staffs on duty per day, and demographic and clinical characteristics of patients per day) were recorded for 5 days and averaged to obtain a representative value for a single day. If necessary, local site visits were performed to clarify the information in the questionnaires.
Statistical analyses
Results are expressed as mean and standard deviation, or as percentages of respondents. Data were analyzed with SAS version 6.12 statistical software (SAS Institute, Cary, NC, USA). Two-tailed Student's t-tests, analyses of variance (ANOVA), Chi-square test, linear by linear association Chi-square test, and logistic regression analysis were used to test the significance of differences in responses, where appropriate. Differences were considered statistically significant at a P value<0.05.
RESULTS
Response rates
The questionnaires were administered to the 105 hospitals with a critical care training program, and were endorsed by the KSCCM. A total of 220 responses were received from the ICUs in 86 hospitals (81.9%) and critical care data were obtained from 3,197 patients.
Characteristics of the ICUs
To be designated as a critical care subspecialty training hospital, several requirements of the KSCCM should be met. One of the most important is having an appropriate educational environment. As a result, 82.3% of all ICUs are in teaching hospitals, either university or university affiliated hospitals. Among the 220 ICUs (41 in public and 179 in private hospitals), 56.4% were located in (35%) or near (21.4%) the capital city, Seoul. Sixty-two of the ICUs (28.2%) were in hospitals with more than 1000 patient beds; 178 (88.2%) were specialized (Table 1). All but two of the neurologic ICUs admitted neurosurgical patients. Most of the ICUs were open units and most of the specialized ICUs were managed by the relevant hospital department (e.g., a medical ICU was part of a department of internal medicine). Of all the ICUs, 35.5% were affiliated with a Department of Internal Medicine, which was also the case for most CCUs, medical, and mixed ICUs. The next largest group was surgery (22.3%) followed by pediatrics (16.8%). All pediatric ICUs were affiliated with a pediatrics department. Anesthesiology was relatively infrequent as a separate department (14.1% of the total ICUs), but was evenly distributed among the various hospitals. Board certified internal medicine specialists were in charge of all the ICUs in most of the smaller hospitals: 61.1% of hospitals with ≤500 beds, 51.0% of hospitals with 501-1,000 beds, and 34.7% of hospitals with >1,000 beds (P=0.03, by linear-by-linear association Chi-square).
The number of ICU beds varied with the type of unit and the hospital size (median 15 beds, range 11-15; Table 1). The number of units also varied, increasing along with hospital size (Table 2) from 1.4 (≤500 beds) through 2.2 (501-1,000 beds) to 6.2 (>1,000 beds) per hospital. A single mixed or general ICU was more common in smaller hospitals and multiple, specialized ICUs were more common in larger hospitals (P<0.001).
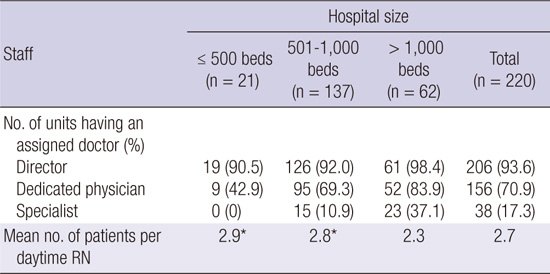
Physician and nurse staffing of the ICUs
Most ICUs had a director who played a major role in the administrative duties and was partly involved in management of the ICU patients. Overall, 70.9% of the ICUs were staffed by dedicated physicians who worked in the unit more than 8 hr a day (Table 3). The dedicated physician included medical specialists, critical care subspecialists, interns (in only 12 ICUs), and residents. Only 38 ICUs (17.3%) had specialists on duty 5 days each week, and that decreased to 17 ICUs (7.7%) when the data from pediatric ICUs were excluded. Fulltime adult critical care subspecialists were only available in 17 units in nine hospitals (Fig. 1) and 12 of the 17 units (70%) were located in Seoul. The daytime nurse-to-patient ratio averaged 1:2.7, and was greater in small and medium sized hospitals than in large ones (P<0.001). In 19 ICUs, one nurse cared for four or more patients.
Available technology in the ICUs
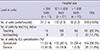
A picture archiving communication system was available in 98.6% of the ICUs and electronic medical records were available in 49.1% (Table 4). Local arterial blood gas analysis monitoring was available in 61.4% of the ICUs and a local patient information database was available in 71.4% of the ICUs. The number of ventilators and monitors per bed were 0.66 and 1.10, respectively.
Characteristics of ICU patients
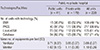
Table 5 shows the demographic and clinical characteristics of 3,197 patients in the ICUs. The mean age of the adult patients was 60 yr. The age distribution of ICU patients differed with hospital size; the percentage of elderly patients over 65 yr of age was higher in smaller than in larger hospitals (Fig. 2). The most common ICU admission was from the emergency room. The most common reasons for ICU admission were respiratory insufficiency (20.2%) and postoperative management (12.8%) among adults, and prematurity (56.4%) followed by respiratory insufficiency (13.6%) among children (Table 6). Central venous catheterization was the most common intervention (43.4%) (Table 7). Pulmonary artery catheterization was only done in 1.2% of the units, most often in surgical and CCUs. All interventions were performed more frequently in larger hospitals.
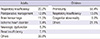
The mean percentage of patients receiving CPR before or after ICU admission was 4.8%, and a mean of 6.0% of patients had "do not attempt resuscitation" orders (Table 8). These percentages were significantly higher in medical ICUs than in other types of ICU, and also in smaller hospitals compared to larger ones.
DISCUSSION
In 2009, there were a total of 975 ICUs and 10,446 ICU beds in Korea, according to data from the National Health Insurance Corporation. The estimated 17 adult ICU beds per 100,000 populationis comparable to other advanced countries (2). Besides medical infrastructure, we are confident that our medical science and technology has grown to a level nearly the equal as that in advanced countries. However, we cannot say that the management and the outcomes in critical care units have reached the same levels as in advanced countries. In a multicenter retrospective analysis of 1090 ICU patients from 18 hospitals with 500-2,200 beds, the overall mortality rate was 24% (3). Considering that those were relatively large hospitals, it is apparent that our mortality rate is worse than that of advanced countries (2). It is clear that there are substantial differences among countries in clinical performance, medical resources, and national spending on health-care. Nevertheless, our findings and their implications raise some serious issues, which may account for this poor outcome.
First, the mean daytime nurse-to-patient ratio was 1:2.7 in this survey, and varied from 1:2.9 in small hospitals to 1:3.2 in mixed ICUs. One nurse provided care for more than four patients in 19 of the surveyed units. This situation could become worse at night due to decreased personnel on night shifts, as often occurs in the open ward setting. Moreover, because there are very few respiratory therapists in Korea, overall bedside duties of ICU nurses are increased, with a corresponding loss of quality of patient care. The increasing need for critical care beds, combined with decreasing budgets and nurse shortages, might lead to inadequate staffing and compromised patient safety in hospitals worldwide. Many studies have demonstrated a relationship between decreased nurse staffing levels and increased adverse patient outcomes in the ICU, including mortality, infection, and pressure ulcers (4-8). To overcome these problems, minimum standards of nurse staffing levels adopted by of critical care nurses associations (9, 10) have resulted in nurse-to-patient ratios of 1:1 or 1:2 in many advanced countries (11, 12).
Second, physician staffing is a serious problem for Korean critical care. In this survey, 70.9% of ICUs had dedicated physicians who worked more than 8 hr a day. That result does not seem bad, but most of the physicians were not intensivists or specialists. Only 7.7% of adult ICUs were staffed by physician specialists for 5 days each week. The outcome of severe sepsis and compliance with the Surviving Sepsis Campaign in Korea was poor in ICUs without fulltime intensivists (1). In several studies that evaluated the association between ICU physician staffing and patient outcomes, higher staffing of intensivists was associated with lower hospital mortality and morbidity (13-17). Furthermore, a new paradigm for 24-hr intensivist coverage in the ICU has emerged recently because of its impact on patient outcomes (18, 19). Staffing with intensivists may also decrease resource use because specialists may be better at reducing inappropriate ICU admissions, preventing complications that prolong length of stay, and recognizing opportunities for prompt discharge. Intensivists take primary responsibility in managing the critically ill patients in the ICUs of many advanced countries (20, 21).
Third, the deficiencies in nurse and physician staffing are related to an unreasonable health insurance reimbursement system and an inappropriate medical law in Korea. Currently, the reimbursement rates are estimated to support only 30%-50% of the original critical care cost. For this reason, most Korean ICUs operate at a deficit, and hospitals tend to avoid further investment in the human resources of their ICUs. Furthermore, Korean medical legislation mandates that neonatal ICUs, but not necessarily adult ICUs, must have dedicated specialists. Our findings show that advanced computer technologies are frequently adopted, with picture archiving communication system available in 98.6% of the surveyed ICUs. However, only 38 ICUs (17.3%) have specialists on duty for 5 days each week.
Korea is categorized as an aging society and is rapidly becoming an aged society. When data from pediatric ICUs were excluded, 53% of the adult patients in this study were elderly people (≥65 yr of age). As the population continues to age, the burden of acute and chronic illness and the demand for critical care services will rise (22). This study shows that critically ill patients may not be treated by the best equipped health-care professionals, even in large hospitals and teaching institutions. The situation in smaller, non-academic hospitals would be expected to be worse. The quality and patient outcome in critical care will worsen over time if current critical care practices remain unchanged. In 2008, as the only organization representing all professional components of critical care in Korea, the KSCCM introduced a subspecialty system for critical care medicine after 6 yr of discussion with other medical societies including those concerned with anesthesiology, emergency medicine, internal medicine, neurology, neurosurgery, pediatrics, surgery, and thoracic surgery. We anticipate that this system will increase the supply of qualified intensivists and will improve quality, efficiency, and outcomes of critical care in Korea. To implement this system, policy makers need to understand the current problems and improve critical care policy, including critical care cost and medical law.
We recognize that our study has several limitations. Our sample size was small, which limited the precision of the results. In addition, the survey was targeted to critical care subspecialty training hospitals instead of using a stratified random sampling method. Thus, the results may not provide a full description of critical care delivery in Korea. However, the results do increase our understanding of the current situation and problems in Korean ICUs. Second, more than half of ICUs in this study were located in the capital region, which occupies only 12% of the area of the country but houses about 50% of the Korea's population and medical institutions. Consequently, we did not need to adjust for these factors when analyzing the results. A third limitation is that we did not include mortality and complications data from each unit in the estimate of the ICUs quality of care. This study could be viewed as the first step in building a Korean critical care database, with more detailed morbidity and mortality data to be collected in the future.
In conclusion, we have described the organization and staffing of ICUs in Korean university and teaching hospitals, and characteristics of admitted patients. The data collected in this survey indicate that staffing of nurses and physiciansis poor compared with that in advanced countries. We believe that the roles of health-care professionals are important, and much effort including enhanced reimbursement of critical care costs must be made to improve the quality of critical care at the national level.






 XML Download
XML Download