

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
'At-risk patients' (also called 'high-risk patients') are patients who face a disparity between their medical needs and the available hospital resources (1). This disparity is often at the root of sudden cardiac arrest and mortality, and it occurs in up to 10% of in-hospital emergency patients who require urgent critical care (2-4). One of the main reasons for this disparity is an insufficient early detection system for at-risk patients, and because of this insufficiency, delayed decision-making often occurs (5). Critical physiological changes, such as unstable vital signs or altered mental status, have been reported in up to 80% of patients who have experienced an arrest, and these are often seen six to eight hours before the arrest occurs (5-10). However, in many cases, doctors and nurses overlook these warning signs (2). Detection is the first step in treatment, and approximately 37% of these events might have been prevented if a simple criterion were monitored, such as abnormal vital signs or altered mental status (e.g., a change from being alert to having slurred speech or becoming delirious or comatose) (4-6). Additionally, it has been reported that the prevention of unexpected clinical deterioration in critically ill patients could be achieved by the simple identification of the warning signs associated with a change in critical vital signs (11).
A rapid response system (RRS), which has also been called a medical emergency team (MET), a rapid response team (RRT), or a critical care outreach (CCO) team, is an innovative system for identifying at-risk patients and saving their lives in general wards. The system identifies at-risk patients before respiratory system, circulatory system, or multi-system organ dysfunction occurs, thus avoiding an intensive care unit (ICU) admission or even preventing cardiac arrest (12-14). Previous studies have identified many types of RRSs that are effective at decreasing cases of in-hospital mortality, although, most models focused on urgent actions in response to calls by a primary medical team. The underutilization of RRSs is widespread, and delays in requesting the RRS team occur in up to 30% of hospitals (15). To reduce the underutilization, one group worked with nurses to help them distinguish 'worry' from 'general concern' when making clinical judgments (16), and another group tried implementing a broad system that would allow family or patients themselves to initiated the RRS team (17). Despite these trials, many RRSs have a low utilization rate due to primary medical teams not calling the RRS despite criteria for activation being met (18). Unfortunately, patients who experienced a delayed RRS call have been shown to have a markedly increased mortality rate compared with those who received a timely call (19-23). More at-risk patients could be saved if an RRS is triggered in a more active and automatic manner. To overcome this limitation of lower utilization, we developed an extended RRS that includes sensitive screening tools and active triggering system before calls from the primary medical team are made. However, until now, most models of RRSs have focused on increasing the number of calls from a primary medical team or initiating urgent actions to the calls.
The Hanyang RRT (HaRRT) is an extended rapid response system (E-RRS) at the Hanyang University Hospital. The E-RRS differed from the previous RRS in that it did not depend on calls from primary medical members and it searched for at-risk patients before the calls were made. We also visited all of the screened at-risk patients and performed some consultations in critical situations prior to the standard medical respirology, cardiology, and nephrology consultations. Our aim was to demonstrate the effectiveness of E-RRS at decreasing unexpected cardiopulmonary arrests. Here, we report the successful first year of this E-RRS.
MATERIALS AND METHODS
Study design and hospital
This was a prospective, observational study performed at Hanyang University Hospital, an 813-bed tertiary care teaching hospital in Seoul, Korea. At the time of the study, this hospital contained a full complement of heart, solid organ, and bone marrow transplant services for adults and children, surgery programs, and medical and surgical sub-specialty services. When the study was conducted, approximately 28,700 patients per year were admitted to this hospital. The hospital also contains 45 intensive care unit (ICU) beds (16 medical, 15 surgical, and 14 pediatric ICU).
Prior to implementation of the E-RRS, staff education was performed from September 1 to December 31, 2011; and the E-RRS program rollout was completed by December 19, 2011. In this study, we included admitted patients who were 18 yr of age or older between January 1 and December 31, 2012. If a member of the primary staff asked for pediatric patients to be managed, we also included them for monitoring and urgent care management. We collected patient data during the year following E-RRS implementation, and we collected the results of sudden arrests occurring in patients over a two-year period. This 2-yr period included the year prior to and the year following E-RRS implementation, which took place from January 1, 2011 to December 31, 2012.
The E-RRS organization
The E-RRS included a respirology staff member as an intensivist (n=1), an interventional cardiologist (n=1), one internal medicine resident (1 day and 1 night duty), and an experienced ICU nurse who was exclusively responsible for the team (n=1). The staff members were available from 07:00 until 20:00. After hours, the night-duty resident was available, and if an additional decision was needed, he or she could call the remainder of the staff at any time; therefore, the effective coverage period was 24 hr per day.
To define the meaning of 'at-risk patients', we modified the E-RRS criteria using the triggering criteria from previous studies (4, 6, 8, 10-13, 19, 22-25). Our definition included not only criteria related to abnormal vital signs, but it also contained critical symptoms, such as stridor, chest pain, altered mental status, and abnormal laboratory findings. The criteria were posted in the form of a yellow poster that was displayed prominently in each ward (25 sites). Specifically, if any of the conditions in the posted criteria were present, the staff members were instructed to call a cellular phone that was exclusive to the E-RRS. The E-RRS criteria are shown in Table 1.
Promotional and educational strategies
We presented the outline of the E-RRS three times for the chiefs of all medical and surgical departments and one time for each department of internal medicine, orthopedics, general surgery, obstetrics and gynecology, and urology. We also introduced screening and early management of high-risk patients to nurses in each hospital wards (23 wards) for three times (69 education sessions over 3 months). We twice held conferences about the management of at-risk patients (shock, mental change, chest pain, and respiratory failure) for all staff of the medical center. All new hires at the medical center were educated regarding the E-RRS. We placed yellow paper regarding the screening of high-risk patients and an introduction to the E-RRS on the wall for medical personnel and patients. We also wore yellow work clothes for the initial 3-month period after implementation. When we screened at-risk patients, we provided consultations to primary medical personnel (doctors and nurses) directly and in written form with a computerized order communication system (OCS). We also found and reported some medical errors such as inappropriate oxygen supply, uncharged infusion pump of main vasopressor, and missing alarms of critical vital signs of patients in step-down units to the department of Quality Improvement (Q.I.). We created hot lines for nurses in each general ward, called 'Ward Saver'. After implementation, we educated them every month and they delivered the contents to their wards.
The E-RRS intervention
In contrast to previous RRS teams, we screened high-risk patients before we received calls from the patient's primary team. This was achieved by cardiology and pulmonology consultations. We also used computerized alerts of abnormal laboratory findings by evaluating abnormal laboratory data from the clinicopathology department (critical value result, CVR). We monitored the patients in a treatment room (step-down unit) of each ward and closely observed patients as they transitioned from the ICU to the general ward. Even if patients were flagged as high risk for a major operation but had normal vital signs and laboratory findings, we monitored them for one day before the operation and followed them for more than 2 days after the operation. E-RRS staff had regular rounds more than twice per day and evaluated patients every day (Table 2).
When activated, an E-RRS team was expected to arrive within 3 min, complete patient assessments within 15 min, and order diagnostic tests and therapeutic treatments that were pertinent to the patient's condition. In addition, management of the evaluation was discussed with the patient's primary medical personnel, and the need for more intensive monitoring or the establishment of a 'do-not-resuscitate (DNR)' status was determined as appropriate.
The E-RRS team was equipped with an emergency pack containing the drugs and equipment needed for resuscitation and endotracheal intubation. After an E-RRS call, if the patient was not admitted to the ICU, then a regular medical round for the patient was performed twice per day until the patient crisis was resolved. At this time, the E-RRS visit was considered a formal consultation, and when the parent unit was contacted, any concerns, advice, and suggestions were verbally communicated and recorded on the patient's chart. For this process, we opened an independent computerized report system for sharing patients' information; this included the reasons for close patient observation, the actions taken during this observation period, and specific symptoms and signs exhibited by the patient that necessitated a call to the team (from October 1, 2012).
Feedback
We reviewed all the screened patients every week and held conferences each month to report monthly results (incidence of unexpected arrest and the analysis of related factors) to the chief of the department of Q.I., the hospital president, head nurses of the general wards and intensive care units, and the chief of the 'Risk Management Team (RMT)'. We prepared questionnaires to assess the satisfaction with the education sessions and actions of the E-RRS (feedback was given monthly and after every education session), and we also created a Facebook site (https://www.facebook.com/withHaRRT) to collect feedback. We regularly reported the number of actions, the types of actions and the results. With the Department of Medical Information Systems, we developed independent electronic medical records for the E-RRS in OCS. We wrote newsletters every 6 months to report the outcomes of the implemented actions.
Study outcomes
The primary outcomes were in-hospital cardiopulmonary arrest rate per 1,000 admissions without a pre-existing do not resuscitation (DNR) order and mortality rate per 100 discharges. A code was defined as any patient with an unexpected cardiac or respiratory arrest requiring resuscitation, with or without the activation of a hospital-wide alert. Cardiac arrests were defined as the cessation of cardiac activity determined by the absence of a palpable pulse. In addition, patients requiring life-saving cardiac compression or emergency resuscitation were considered to have had a cardiac arrest. Respiratory arrest was defined as apnea and unresponsiveness. The data on the primary reason for a rapid response team activation, rapid response team interventions, and disposition of patients after a rapid response team evaluation were also prospectively collected.
Statistical analysis
The data were analyzed using SPSS software, version 19.0. Continuous variables were expressed as the mean±standard deviation or the median±the interquartile range. The study variables were compared with a chi-square test. A multiple logistic regression analysis was used to evaluate the adjusted trends in the outcome variables throughout the study period. A modified early warning score (MEWS) was used to reflect the initial status of the screened patients. This variable was selected according to previous reports on screening at-risk patients (24-26). Continuous variables were tested using a two-tailed t-test for independent samples.
RESULTS
Baseline patient characteristics
We screened 2,722 at-risk patients among all patients who were hospitalized over a one-year period. Of these patients, 1,996 were treated with interventions including emergency consultations, procedures (e.g., intubation, C-line insertion and early goal-directed therapy) and ICU arrangements, and the rest were closely observed without actions. The mean patient age was 64.5±15.8 (13-101) yr, and the number of males was 1,368 (51.0%). The baseline characteristics of the subjects are shown in Table 3. Most of the subjects were patients in step-down unit or were at-risk patients who were automatically identified by an emergent cardiology or respiratory consultation (n=2,302, 84.6%). Other patients were identified following calls from primary physicians (n=234, 8.6%), abnormal laboratory findings (CVR, n=141, 5.2%), or those deemed to be at high risk for a major operation (n=70, 2.6%) as determined by the Department of Anesthesia. Many of these patients had more than one cause for screening. There were 1,388 of screened patients who had symptoms and signs that met the call criteria (51.0%), but only 16.5% of them were reported to the E-RRS by calls from the primary physician (Table 4). Abnormal heart rate, elevated respiratory rate, and hypoxia were the most common signs that met the E-RRS criteria, and approximately 32.3% of patients exhibiting these signs required advanced procedures; however, only 17.9% of them were reported to the E-RRS. The patients with abnormal laboratory findings of low pH, high lactate level, or electrolyte imbalances were not reported to the E-RRS, even if they required advanced procedures after screening (Table 4). Calls from the primary ward doctor were more surgical in nature (surgical vs medical, 3.7% vs 3.3%, respectively, P=0.041). Surgical patients were also younger (63.0±16.0 vs 65.7±15.4 yr, P=0.027), and they had a lower MEWS than medical patients (1.49±1.12 vs 1.79±1.37, P<0.001).
The E-RRS procedures
The E-RRS team initiated and completed a variety of investigative, preventive and therapeutic procedures. An E-RRS response was triggered not only by an emergency call from primary medical personnel but also if the patient needed emergency management after evaluation by E-RRS staff. We also performed emergency consultations prior to regular consultations, which included correcting an electrolyte and fluid imbalance, early use of antibiotics, early anticoagulation treatment for a pulmonary thromboembolism, treatment of pulmonary congestion, ventilator care of patients with amyotrophic lateral sclerosis, treatment of arrhythmia (using a defibrillator or medication for PSVT, atrial fibrillation, and bradycardia), and emergency cardiology consultation via a hotline. Some cases required multiple actions (for example, septic shock due to pneumonia, intubation, C-line insertion, early goal-directed therapy, oxygen supplementation and ICU arrangements). An outline of these procedures is shown in Table 3. Advanced managements such as intubation, C-line insertion, early goal-directed therapy (EGDT) and ICU arrangements were performed in 16.9% of screened cases (Table 4). Hypoxia was the most common reason we were called, and 30.5% of these patients required an advanced procedure such as intubation or ICU care. For patients with chest pain, shock and altered mentality, half required advanced procedures, but the call rate was not high among these patients (Table 4).
Outcomes
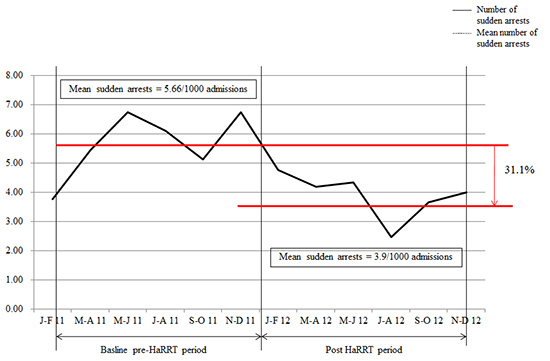
After E-RRS implementation, the mean hospital code rate decreased from 5.66 to 3.90 per 1,000 admissions. This represents a 31.1% decrease in sudden deaths compared with the pre-implementation period. The in-hospital mortality rate was also reduced by 15.3%, from 1.63 to 1.38 per 100 discharges (Fig. 1).
Of the 1,321 surgical patients, 19 patients (including 10 DNR-patients) died; 34 of the 1,440 medical patients (including 11 DNR-patients) died. Lower mortality was observed in surgical patients (mortality in surgical patients vs medical patients was, 1.4% vs 2.4%, respectively), but this difference was not significant after it was adjusted for age, sex, or patient MEWS (P=0.466).
Despite the E-RRS intervention, 49 patients died. In addition, 32 of these patients were not treated intensively and their surrogates signed a DNR permission document. The other 17 cardiac arrests that occurred during the E-RRS intervention developed due to acute myocardial infarction (n=3), respiratory failure (n=4), septic shock (n=8), or a postoperative complication (n=2). The outcomes are shown in Table 5. The rate of arrests due to respiratory failure was significantly reduced after E-RRS implementation (47.8% vs 33.3%, P=0.046), but shock and cardiac arrest rates did not change. Among surgical patients, the number of arrests declined (13 cases vs 10 cases), but this finding was not statistically significant (P=0.333).
DISCUSSION
This is the first report in Korea describing the implementation of an E-RRS triggered and activated automatically before calls from the primary medical attendants in an 813-bed university hospital. The implementation of the E-RRS significantly decreased the incidence of all-cause sudden arrest by 31.1%, and it was particularly effective at reducing the rate of arrests due to respiratory failure. The intervention may also be associated with a decline in the in-hospital mortality rate. Importantly, this system worked with only four E-RRS team members, including an intensivist, and devices for airway management. Furthermore, these results were achieved without more extensive investigation.
The literature on the results of previous RRSs reveals variable success in reducing sudden arrests and mortality. This variation may be explained by the unexpected variances in the baseline events rates, short observational periods, and differences between the types of RRS (nurse-led vs. doctor-led teams) (27-29). Screening is the first step in triggering an RRS, but there are many barriers to calling an RRS team to care for at-risk patients, such as disengagement between the doctors and nurses, professional resistance, and inadequate knowledge for recognizing at-risk patients (1). In previous studies, 20%-25% of patients at risk were not identified due to insufficient recognition of the patient warning signs by doctors and nurses (5, 6). It has been reported that 3.7%-4.0% of hospitalized patients show critical symptoms and signs and that the rate of adverse events due to negligence is 0.8%-1.0%. A delay in making an RRS call is a problem; it has been reported that approximately 30% of patients at risk had a delay between the presentation of critical signs and when the call was made (15), with a mean delay of >13 hr (22). Many of these delays were associated with an increase in patient mortality or morbidity rates (7, 22). Continuous education and awareness are solutions to this problem, but these measures also have limitations, including low perception rates and the underutilization of RRSs (20, 21, 23).
We attempted to overcome this screening limitation in our RRS through an early screening protocol. The mean modified early warning score (MEWS) in this study was 1.5±1.3 compared with scores of more than 2.0 in other studies that relied on calls from primary medical attendants. We also established regular rounds to monitor the screened patients, directed the alarm for abnormal laboratory findings, and conducted emergency call training for emergency primary medical attendants. This E-RRS was effective despite the short implementation and brief intervention periods. Advanced procedures such as intubation, C-line insertion, early goal-directed therapy and ICU arrangements, occurred in 16.9% of cases. We screened a total number of 5.9 times of these patients, and approximately 80% of screened patients needed only consultation and monitoring of vital signs. Someone could criticize this as the squandering of the hospital's resources. However, the aim of study was to save as many at-risk patients as possible using limited resources by enrolling these patients in the E-RRS, which overcame limitations of a previous RRS that depended on calls, and we strove to find the maximum efficiency with the minimum resources. It may be an endeavor to develop a complete system as part of a patient safety initiative, and this study could provide elementary data for further trials.
Despite our efforts, we missed 22 at-risk patients during the year following E-RRS implementation, and 16 (72.7%) of these patients died after long cardiopulmonary resuscitations. Twelve of these patients experienced respiratory failure with metabolic acidosis, with or without septic shock, and 4 patients had sudden myocardial infarctions. This omission of at-risk patients revealed the limitation of our screening, and we should develop further screening tools for at-risk patients. To ameliorate the weak points in our RRS, we have tried to continuously screen the patients with greater regular rounding, regular RRS education, and small discussion groups about patient safety, and we also developed the in-hospital network services including a computerized alert.
There were more calls from the primary ward doctors in surgical parts and the surgical patients showed younger age and lower MEWS than the medical patients. However, they did not show differences in mortality between surgical and medical parts. This means that the at-risk patients in the surgical department had less severe signs and lower MEWS than medical patients, but experienced the same mortality. Thus, we expect that an E-RRS could be more effective at decreasing mortality among surgical patients than among medical patients, even if more minor symptoms and signs are incorporated to improve the E-RRS.
The E-RRS decreased the rate of sudden arrest and mortality. However, these data are from one center, and there are many confounding factors such as changes in the hospital management policy and in the perception of patient safety, as well as the opening of a coronary care unit (CCU). The decline in mortality may have resulted from a decrease in the number of at-risk patients admitted in this year. There were no data on the number of high-risk patients in the past year. It is likely that the rate of at-risk patients did not decrease in this year because the turnover rate in the intensive care units increased from 103% in the previous year to 112% in the study year. At-risk patients who required intensive treatment were screened effectively by the E-RRS, which resulted in a higher turnover rate in the ICU. Before implementation of the E-RRS, spontaneous reporting from the primary physician was the only way to collect data on sudden arrest. These many serious omissions in the official records and the neglect of critical signs led to at-risk patients being missed. Regarding this, making and posting definitions of at-risk patients might be one effective method to promote and implement the E-RRS.
There were few reports in the literature regarding computerized alert systems and the sharing of information. We designed the alert system to use critical values, and we also developed a new computerized chart for the E-RRS. With this, we could share the list of at-risk patients in real-time on ward computers, and the information provided a focus for management and an indication to the primary physicians and nurses of when an emergency call was warranted. This may be the first trial to use technology for the implementation of an E-RRS.
In conclusion, we report the implementation of an E-RRS associated with a reduction in hospital code and mortality rates over a short (one-year) observational period. A more active and automatic system could save more at-risk patients, and our design could be considered as a pilot trial for other RRS studies.





 XML Download
XML Download