

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute mountain sickness (AMS) is characterized by headache in an unacclimatized person who recently arrived at an altitude above 2,500 m, plus one or more of the following: gastrointestinal symptoms, weakness, dizziness or lightheadedness, and difficulty sleeping (1, 2). Altitude acclimatization is associated with hypoxia-induced erythropoietin (EPO) secretion that begins 1-2 days after the ascent commences, however, it takes weeks to affect an increase in hemoglobin (Hb) (3). EPO is a glycoprotein which stimulates red blood cell production. According to the review article about effects of recombinant human EPO in normal humans, EPO increases the arterial O2 content not only by a increase in red blood cell volume, but also by a decrease in plasma volume. EPO also increases exercise performance and cognitive function in healthy adults (4). Several reports have suggested that EPO may also have nonerythropoietic properties that protect the brain, spinal cord, retina, heart, and kidney from ischemic and other types of injury (5), independently of its effect on Hb (6-8). While it is possible that Hb-elevating EPO therapy weeks before altitude exposure can decrease AMS, this has not been tested. The present randomized controlled trial was performed to assess whether prophylactic EPO injections can prevent AMS.
MATERIALS AND METHODS
This study was a open-label randomized, parallel-arm, controlled trial performed in Asan Medical Center, a tertiary referral university hospital.
Participants
Participants were excluded if they had a history of cardiovascular disease or other serious illness, uncontrolled hypertension (>140/90 mmHg), were current smokers, or had a known hypersensitivity to mammalian cell-derived products. Subjects with Hb>15.5 g/dL were also excluded so that the Hb levels after EPO therapy would be <17 g/dL. We could not estimate the sample size in the design of this study, because there was no similar study previously and we could not do pilot study. Initially, 45 subjects with Hb≤15.5 g/dL volunteered to participate. However, baseline testing then revealed that six men had Hb>15.5 g/dL and they were excluded. The remaining 39 subjects were enrolled after being informed of the requirements and risks of this research and providing written consent. There were 16 men and 23 women. The mean age of the cohort was 44.5±12.6 yr (range, 18-65 yr). All subjects lived in the Seoul area at sea level.
Interventions
The EPO group subjects were administered 10,000 IU epoetin alpha (Epokine®, CJ, Seoul, Korea) subcutaneous injections with a pre-filled syringe once per week for 4 consecutive weeks, starting 5 weeks before departure. The last injection was given 7 days before departure.
Subjects were not permitted to use any self-prescribed drugs that could affect AMS during the 5½-week study period. Aspirin 100 mg/day (Aspirin protect®, Bayer, Leverkusen, Germany) was prescribed to all subjects during the study period. The 10 subjects with <20% transferrin saturation were given iron 80 mg/day (Feroba®, Bukwang Pharma, Seoul, Korea). These subjects comprised six (two males, four females) and four (four females) subjects in the EPO and control groups, respectively. After arriving at the 3,230 m high lodge at Deurali on day 33 of the study (see below), all subjects were given sildenafil citrate (Heragra®, CJ, Seoul, Korea) 50 mg p.o. before sleeping and on the following morning. This treatment was repeated when the subjects arrived at the 4,130 m high lodge at Annapurna base camp (ABC) on day 34 (see below). Subjects who met the criteria for an immediate descent were treated with an intramuscular injection of dexamethasone (Dexamethasone®, Yuhan, Seoul, Korea) 5 mg.
The ABC is 4,130 m high and located in Nepal and was chosen as the climb summit because the highest altitude in South Korea is 1,950 m. Moreover, many Koreans consider climbing to the ABC a desirable objective, which made it easy to recruit study participants. In total, 45 people went to the ABC, namely, the 39 participants, four investigators, and two research assistants.
The schedule of this study was as follows: Day 1 (24 January, 2013): The blood pressure (BP), pulse rate (PR), arterial oxygen saturation (SaO2), iron status, hemoglobin (Hb), and hematocrit (Hct) of all subjects were measured. The first EPO injection was given to the EPO group. Daily aspirin (100 mg) and iron treatment started.
Days 8, 15, and 22: The BP was measured and the second, third, and fourth EPO injections were given to the EPO group.
Day 29: BP, PR, SaO2, iron status, Hb and Hct in all subjects were measured.
Day 30: Departed from Seoul (which is at sea level) by airplane and arrived at Pokhara (900 m) via Kathmandu.
Day 31: Started trekking and arrived at Landruk (1,565 m).
Day 32: Arrived at Sinuwa (2,360 m).
Day 33: Arrived at Deurali (3,230 m). Gave all subjects sildenafil before sleeping.
Day 34: Gave all subjects sildenafil in the morning. Arrived at the ABC (4,130 m). Gave sildenafil to all subjects before sleeping.
Day 35: Gave all subjects sildenafil in the morning. Arrived at Chomrong (2,170 m).
Day 36: Arrived at Pokhara (900 m).
Day 37: Returned to Seoul.
Outcomes
Outcomes measures were Lake Louise score (LLS), AMS incidence, and number of subjects who met immediate descent criteria. At 3,230 m (Deurali) and 4,130 m (ABC), each subject was given a LLS questionnaire that had to be completed in the evening before dinner. The LLS score is the sum of answers to five questions about headache, gastrointestinal symptoms (anorexia, nausea, or vomiting), fatigue or weakness, dizziness or light-headedness, and difficulty sleeping. The subjects had to rate these symptoms from 0 to 3, where 3 indicates severe and incapacitating symptoms (1). Degree of sleep was evaluated with sleep last night, for example, the first LLS score at Deurali (3,230 m) was evaluated with sleep at Sinuwa (2,360 m). If the subject had a headache and a total score of ≥3, AMS was diagnosed (1). Table 1 shows the immediate descent criteria by US Army Research Institute of Environmental Medicine (USARIEM) (9).
Systolic and diastolic blood pressure (SBP and DBP, respectively) and pulse rate (PR) were measured by using the wrist blood pressure monitor BC-16 (Beuer, Ulm, Germany). Arterial oxygen saturation (SaO2) was measured by using a NB-Oximeter (Netblue, Daegu, Korea). All measurements were performed 2-3 hr after arrival, at rest and during breathing quietly for several minutes before taking measurement. We measured value for several minutes to determine the predominant value.
Randomization and baseline characteristics
Study subjects were randomly assigned in a 1:1 ratio to the EPO or control group after the baseline Hb results became available. The randomization sequence was generated by computer at the Asan Medical Center. Block randomization to ensure gender or age equivalence between groups was not performed.
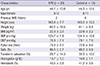
Twenty and nineteen subjects were randomized into the EPO and control groups, respectively (Table 2). Two subjects in each group were taking anti-hypertensive medications.
Comparison of the men and women in terms of baseline characteristics revealed significant differences in mean Hb levels (14.6±0.6 vs 13.3±1.0 g/dL, P<0.001), hematocrit (Hct, 42.6±1.6 vs 39.6±2.5%, P<0.001), height (171.5±6.4 vs 158.0±5.3 cm, P<0.001), weight (68.4±8.0 vs 55.2±6.4 kg, P<0.001), SBP (129.5±7.9 vs 120.1±8.0 mmHg, P=0.001), and iron saturation (34.8±13.2 vs 26.6±10.7%, P=0.048). However, the males and females did not differ in terms of age, body mass index (BMI), PR, SaO2, and DBP.
Statistical analysis
The data were presented as mean±SD. To assess the statistical significance of differences between the EPO and control groups, Student's t-test and Fisher's exact test were used. Normality test was performed with Shapiro-Wilk test.
Multiple linear regression analysis was used to evaluate independent predictors of AMS score and multiple logistic regression analysis to identify independent predictors of AMS and satisfaction of immediate descent criteria. To perform multivariate analysis, we chose dependent variables as significant factors for AMS score, AMS or the number of subjects who met immediate descent criteria in univariate analysis.
Differences were considered to be statistically significant if P was <0.05. All analyses were performed by using SPSS version 12.0 (SPSS Inc, Evanston, IL, USA).
RESULTS
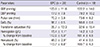
Five weeks after the baseline measurements on day 1 (Table 2), during which time the EPO group received four injections of EPO, the clinical parameters of the two groups were measured again (day 29, Table 3). The two groups did not differ in terms of SBP, DBP, PR, SaO2 or transferrin saturation. None of the subjects started taking anti-hypertensive drugs or increased the dose during the 5½-week period. However, the EPO group had significantly higher Hb levels than the control group on day 29 (15.4±1.1 vs 14.2±1.0 g/dL, P=0.001). They also had significantly higher percent changes in Hb relative to baseline (12.6±5.9 vs 1.4±4.6%, P<0.001). In one of the 20 EPO-treated subjects, the Hb was >17 (17.1) g/dL on day 29. Moreover, three of the EPO-treated subjects had Hct >50% on day 29 (up to 50.7%). The males and females in the EPO group did not differ in terms of mean Hb increase (11.6±5.7 vs 13.2±6.1%, P=0.56). In the EPO group, the mean EPO dose per kg of body weight was 170.8±28.3 U/kg. The mean dose was significantly lower in males than in females (146.3±17.0 vs 187.2±21.7 U/kg, P<0.001). This reflects the fact that the males in the EPO group had a significantly higher body weight than the females in that group (69.2±7.8 vs 54.2±7.3 kg, P=0.001). According to the review article about effects of erythropoietin in normal humans (4), the median weekly EPO dose in 9 studies was 162 IU/kg (range 60-120~350 IU/kg). The mean weekly EPO dose used in this study was 170.8 IU/kg.
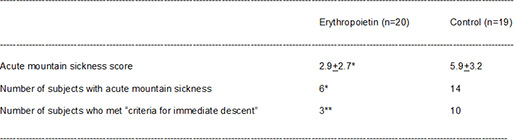
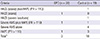
The two groups were then compared in terms of their clinical and AMS parameters at Deurali (3, 230 m) and ABC (4,130 m) (Table 4). The EPO group had significantly lower LLS scores at ABC than the control group (2.9±2.7 vs 5.9±3.2, P=0.003). Of the whole cohort of 39 subjects, 20 (51%) developed AMS at ABC. Compared to the control group (74%, 14/19), significantly fewer EPO-treated subjects (30%, 6/20) developed AMS at ABC (P=0.01). The two groups did not differ in terms of SBP, DBP, PR or SaO2. In addition, compared to the control group (53%, 10/19), significantly fewer EPO-treated subjects (15%, 3/20) met the criteria for immediate descent at 4,130 m (P=0.019) (Table 5).
The 13 subjects who met the criteria for immediate descent had lower mean SaO2 values at ABC than the 26 subjects who did not (84.7±4.2 vs 88.2±3.4%, P=0.017). However, the latter two groups did not differ in terms of SBP, DBP, hypertension, or PR at ABC.
Comparison of the 16 subjects in the whole cohort who were >50 yr old to the 23 subjects who were <50 yr old revealed these two groups did not differ in terms of LLS score (5.2±3.6 vs 3.7±3.0, P=0.19), AMS incidence (56% vs 43%, P=0.75), or the number of subjects who met immediate descent criteria (50% vs 22%, P=0.09) at ABC.
In addition, the 16 males in the whole cohort did not differ from the 23 females in terms of LLS score (3.3±2.5 vs 5.0±3.6, P=0.08), AMS incidence (38% vs 61%, P=0.20), or the number of subjects who met immediate descent criteria (19% vs 43%, P=0.17).
The 23 subjects in the whole cohort whose Hb was <15.0 g/dL on day 29 had significantly higher LLS scores (5.8±3.0 vs 2.3±2.5, P<0.001) and AMS incidence at ABC (74% vs 19%, P=0.001) than the 16 subjects whose Hb was ≥15.0 g/dL on day 29. However, these two groups did not differ in terms of the number of subjects who met immediate descent criteria (43% vs 19%, P=0.17).
The 16 subjects in the whole cohort whose SaO2 at ABC was <87% had higher LLS scores (6.2±3.5 vs 3.0±2.4, P=0.005), AMS incidence (75% vs 35%, P=0.022), and number of subjects who met immediate descent criteria (56% vs 17%, P=0.017) than the 23 subjects whose SaO2 at ABC was ≥87%.
To perform multivariate analysis, we chose three dependent variables, EPO group, Hb after EPO therapy and oxygen saturation at ABC, which were significant factors for AMS score, AMS or the number of subjects who met immediate descent criteria in univariate analysis. Two continuous dependent variables, hemoglobin after EPO therapy and oxygen saturation at ABC, showed normal distribution.
Multiple linear regression analysis revealed that SaO2 87% (β, -2.570, standard error [SE], 0.808; P=0.003), control group (β, -2.237, SE, 0.833; P=0.011), and Hb<15.0 g/dL (β, -1.935, SE, 0.879, P=0.034) were independent predictors of LLS score.
Multiple logistic regression analysis showed that Hb<15.0 g/dL (odds ratio [OR], 0.155; 95% confidence interval [CI], 0.027-0.875, P=0.035), SaO2<87% (OR, 0.130; 95% CI, 0.018-0.916; P=0.041) and control group (OR, 0.148; 95% CI, 0.022-0.976, P=0.047) were independent predictors for AMS incidence.
Multiple logistic regression analysis also showed that SaO2<87% (OR, 0.099; 95% CI, 0.015-0.659, P=0.017) and control group (OR, 0.095; 95% CI, 0.012-0.719, P=0.023), but not Hb <15.0 g/dL (OR, 1.146; 95% CI, 0.177-7.429, P=0.89), were independent predictors of the number of subjects who met the immediate descent criteria. During the night in ABC, one woman in the control group complained of symptoms of moderate high altitude pulmonary edema (HAPE); headache with cough, dyspnea at rest. All participants returned safely and there were no adverse effects of EPO such as thromboembolic events.
DISCUSSION
To the best of our knowledge, this is the first randomized controlled trial examining the ability of prophylactic EPO injections to prevent AMS. This study revealed that EPO pretreatment significantly decreased LLS scores, AMS incidence, and the number of subjects who met immediate descent criteria.
The most likely explanation for these effects of EPO on AMS is that EPO pretreatment increased the Hb levels by 12.6%. Since the theoretical arterial oxygen content (CaO2) curve rises with increasing Hb until a maximum Hb of 20.7 g/dL is reached (10), Hb may reduce AMS by elevating CaO2 levels.
In this study, EPO treatment, but not Hb≥15.0 g/dL, was independent predictor of the number of subjects who met immediate descent criteria. While the most likely explanation for the effect of EPO pretreatment on AMS is that the treatment elevated Hb levels, several reports have suggested that EPO may also have nonerythropoietic properties that protect the brain, spinal cord, retina, heart, and kidney from ischemic and other types of injury (5). Miskowiak et al. (6, 7) reported that EPO improved cognitive function and memory 3 days after the administration in healthy volunteers; these effects occurred in the absence of hematological changes. Another group also reported that EPO reduces cerebral and systemic vascular conductance independently of its effect on Hct in healthy male subjects (8). As another example of these nonerythropoietic effects of EPO, we found that in dialysis patients, EPO treatment but not RBC transfusion improves their muscle energy metabolism (11, 12).
Previous studies showed that an EPO dose of 150 IU/kg weekly (or 50 IU/kg three times per week) for 4 weeks increases Hb by 7.0%-12.0% 1-2 weeks after the last dose (13-15). In the present study, the dose was 10,000 IU (mean 170.8 IU/kg) weekly for 4 weeks and 1 week after the last dose, the Hb was 12.6% higher relative to baseline. However, in one of the 20 EPO-treated subjects, Hb exceeded 17 g/dL, while in three subjects, Hct exceeded 50%. Since an excessive increase in RBC mass (Hct>50%) can cause possible thromboembolic events, aspirin has been suggested to be a preventative treatment for altitude-related thromboembolic events (9). Thromboembolic events were not detected in either group in this study.
In the present study, the subjects arrived in high altitude locations (>2,500 m) 11 days after receiving the last dose of EPO. Krzyzanski et al. have shown that when healthy subjects are given a single dose of 20-160 kIU epoetin alpha, the RBC increase peaks around 10 days (16). Thus, the RBCs of our EPO-treated subjects may have been at their most elevated point when the subjects entered high altitude conditions.
In the present study, SaO2 was another independent predictor of LLS score, AMS incidence, and the number of subjects who met immediate descent criteria. Roach et al. (17) showed that SaO2 measured by noninvasive pulse oximetry correlated inversely with AMS severity; they also found that SaO2 may predict the development of AMS. Similarly, soldiers whose resting SaO2 levels are at or below the median value for a particular altitude are at greater risk of developing altitude sickness than individuals whose resting SaO2 exceed that median SaO2 value (9). Mean value of SaO2 at 4,240 m ranged 87%-87.6% (18), therefore, we chose 87% as a cut-off value in this study.
In the present study, the EPO and control groups did not differ in terms of SaO2 levels at baseline, just before the departure from Seoul, or at high altitude. Several studies also found that subjects who received EPO or novel erythropoiesis stimulating protein (NESP) did not differ in terms of SaO2 levels from controls during exercise in acute hypoxia (19, 20).
According to a USARIEM report, when unacclimatized soldiers who ascend rapidly from an altitude below 1,200 m to 4,000-4,500 m, 30%-40% develop severe AMS (9). In the present study, however, 58% (11/19) of the control group subjects developed severe AMS, including high altitude cerebral edema (HACE) and moderate HAPE. This very high rate of severe AMS may be due to our short acclimatization schedule. The guideline for acclimatization is that once one has climbed above an altitude of 2,500 m, the altitude at which one sleeps should not be increased by more than 600 m in 24 hr and an extra day of acclimatization should be added for every 600-1,200 m increase (2). In the present study, the altitude at which our subjects slept rose by 870 m on day 32, when the subjects climbed from Sinuwa (2,360 m) to Deurali (3,230 m), and by 900 m on day 33, when we climbed to ABC (4,130 m). The reason for this short acclimatization schedule was that a direct flight from Seoul to Kathmandu was only available twice a week and most participants could not take 2 weeks of vacation for this study. It was decided that, given the beautiful sunrise over ABC, it was preferable to climb to ABC rather than climb to Deurali over 2 days and then descend (which would have met the acclimatization guidelines). The risks of this short acclimatization schedule were explained to all the participants before study and they agreed to accept them.
In this study, we employed the USARIEM guidelines for immediate descent. The Lake Louise Consensus definition of HAPE requires that at least two symptoms (dyspnea at rest, cough, weakness or decreased exercise performance, and/or chest tightness or congestion) and at least two signs (crackles or wheezing, central cyanosis, tachypnea, and/or tachycardia) are met (1), while a diagnosis of HACE requires the onset of ataxia, altered consciousness, or both in someone with AMS or HAPE (2). However, the USARIEM recommends immediate descent when only moderate HAPE is observed, namely when even one or two symptoms or signs are present (9). Moreover, the USARIEM includes "severe lassitude" in their definition of HACE. We followed USARIEM recommendations to ensure that we would detect the earlier forms of HAPE or HACE.
Acetazolamide is widely used to prevent AMS. However, several experts are concerned about the side effects of this drug, namely allergic reactions such as blood dyscrasias, Stevens-Johnson syndrome, renal failure, and toxic epidermal necrolysis (21, 22). In the present study, all participants were given sildenafil during their stay at Deurali and ABC. Sildenafil has been recommended for the prevention of HAPE because of its pulmonary vasodilator effects (23). While the recommended preventative dose of sildenafil is 50 mg q 8 hr, each subject was only given 50 mg sildenafil before sleep and in the following morning. The afternoon dose was omitted because headache is the most common adverse effect of sildenafil (16% of subjects) (24), and this could have affected the evaluation of AMS in the evening.
There is no US Food and Drug Administration (FDA) guideline of EPO use in healthy people. EPO increases the blood pressure even in healthy subjects (4). However, Lundby and Olsen (4) concluded that EPO seems safe to use for experimental purposes in healthy volunteers, because the metabolic and hormonal effects of EPO do not seem to range beyond physiologically acceptable limits and are reversible. EPO did not increase the blood pressure in this study.
There are several limitations in our study. First, our study was not blinded, which may affect the results, particularly regarding symptoms related to AMS. Second, AMS was evaluated in the evening rather than in the morning, which might affect the validity of the score. We tried to identify the subjects with AMS and to prevent from developing severe AMS during the night. This reflects the fact that hypoventilation during sleep increases the severity of hypoxemia, which can increase AMS severity (9). Third, at least 10 events per variable may be needed to analyze by multiple logistic analysis. Only 39 participants were included and total 13 events of "satisfaction of immediate descent criteria" happened in this study. However, this study is a exploratory study and this multivariate analysis is also a exploratory data analysis. Fourth, the numbers of subjects were relatively small considering diverse ages and both genders, therefore we could not draw a conclusion about safety of EPO in high altitude.
In summary, the present study shows that EPO is an effective prophylactic treatment for AMS in an actual mountain environment. Comparison of EPO with well-established means of prophylaxis such as acetazolamide or dexamethasone needs to be clarified in the future study.


 XML Download
XML Download