

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pituitary adenoma (PA), comprising 10%-15% of intracranial neoplasms, is the most common benign neuroendocrine tumor of the central nervous system (1-5). The prevalence of PAs in autopsy subjects has been reported to be 5%-20% (6). In community-based cross-sectional studies, their prevalence is one per 1,000 population (3, 4). Most PAs found in autopsies are incidentaloma without clinical impact (5). However, the exact incidence and proportion of hormone-producing PAs, especially in the Korean population, remain unknown.
PAs are classified as functional or nonfunctional and divided into macroadenomas (≥ 10 mm) and microadenomas (< 10 mm) according to tumor size (6). Patients with PAs present with a variety of signs and symptoms related to excess or impaired pituitary function and/or mechanical effects. In order of frequency, prolactin (PRL)-, growth hormone (GH)-, and adrenocorticotropic hormone (ACTH)-producing tumors are the most common functioning PAs that can cause functional changes in end organs. One-third of PAs are not associated with symptoms or signs of hormone excess. The majority of clinically nonfunctioning pituitary tumors are gonadotroph cell adenomas (7, 8). True nonfunctioning pituitary tumors are difficult to recognize until their growth results in symptoms such as headaches, visual disturbances, and cranial nerve palsies as a result of their mass effect, or hypopituitarism. In this study, we analyzed surgically resected and immunohistochemically evaluated PAs in our institute over 6 yr to determine the clinicopathological characteristics such as gender, age, symptoms, size, and proportion of hormonal subtypes of PAs in the Korean population.
MATERIALS AND METHODS
We analyzed 506 cases of surgically resected pituitary lesions from 2006-2011 and reviewed the patients' medical records, pathology reports, radiological findings and immunohistochemical studies retrieved from the Seoul National University Hospital (SNUH) archives.
This research was approved by the Institutional Review Board (IRB) of SNUH (1304-038-479). Informed consents were waived by the IRB board.
RESULTS
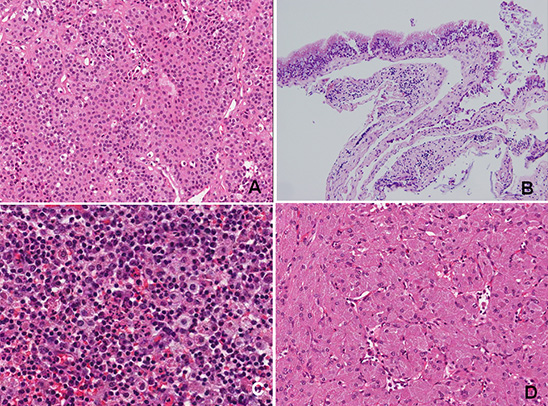
In total, 506 cases of surgically resected and pathologically confirmed pituitary lesions were reviewed: PAs (n=422, 83.4%), Rathke's cleft cysts (RCCs) (n=54, 10.6%), inflammatory lesions (n=8, 1.6%), meningiomas (n=4, 0.8%), craniopharyngiomas (n=4, 0.8%), granular cell tumors (n=1), metastatic renal cell carcinomas (n=2), germinomas (n=1), ependymomas (n=1), and normal pituitary tissue or unsatisfactory specimens (n=9, 1.8%) (Table 1). Fig. 1 depicts representative microscopic findings.
PAs were common in patients in their 40s to 60s (mean age: 48.8 yr), and there was female predominance at these ages; however, there was male predominance in patients under 20 yr and over 70 yr (Fig. 2, Table 2). The mean ages at diagnosis of patients with immunohistochemically proven prolactinoma (PRLomas), GH-producing PAs, follicle stimulating hormone (FSH)-producing PAs, adrenocorticotrophic hormone (ACTH)-producing PAs, thyroid stimulating hormone (TSH)-producing PAs, leuteinizing hormone (LH)-producing PAs, plurihormonal PAs, and nonfunctioning PAs were 41.1, 43.6, 57.2, 49.9, 36.1, 46.0, 44.8, and 53.7 yr, respectively (Table 2). Therefore, FSH producing PAs tended to occur in older patients and TSH producing PAs tended to develop in younger patients. In patients in their 40s with PA, women were more predominant (M:F=1:1.78) (Table 2). However, the most PA types exhibited a female predominance (M:F=1:2.91) except FSH-producing PAs (M:F = 1:0.58). None of them had gonadotrophin induced symptoms, which might be associated with age and gender. All the gonadotrophin producing PAs occurred in old age (more than 41 yr old), except one case (19 yr old). And the patients with FSH-producing PA showed male predominance as mentioned above. The age and gender distributions for patients with PAs are shown in Fig. 2. Among PAs, PRL-producing adenomas were most common (16.6%), followed by GH-producing adenomas (9.2%). The remaining PAs were FSH- (8.8%), ACTH- (5.9%), TSH- (1.7%), and LH- (0.5%) producing adenomas. Plurihormonal PAs produce more than one pituitary hormone, occurred in 14.9% of patients. Nonfunctioning adenomas comprised 42.4% of pituitary adenomas (Table 2). Most of our cases (about 95%) were macroadenoma (diameter>1.0 cm), which frequently involved the sellar and suprasellar area, and showed cavernous invasion.
Clinically, the patients with PAs had been suffered from visual disorders (37.0%), abnormal hormonal effects (23.1%), headaches/nausea and vomiting/dizziness (23.0%), neurological deficits (1.9%), but 15 % of them was found incidentally (15.0%) (Table 3). Seventy patients with PRL producing PAs had been suffered from more amenorrhea/galactorrhea (36%), headache/dizziness (26%) and visual problems (24%) and 10% was incidentally found. Thirty-nine patients with GH producing PAs had been suffered from acromegaly/gigantism (74.4%), headache (12.8%), decreased visual acuity (5.1%) and incidentaloma (7.7%). Thirty-nine patients with gonadotrophin (FSH or LH) producing PAs had suffered from visual problems (52.6%), headache, nausea and vomiting and/or dizziness (18.4%), incidentaloma (23.7%), neurologic deficit (2.6%) and panhypopituitarism (2.6%), however, none of cases showed gonadotrophin related symptoms. Twenty-five patients with ACTH producing PAs had presented with visual symptoms (32%) including decreased visual acuity, visual field defect and diplopia, headache & nausea (28%), amenorrhea and dysmenorrhea/galactorrhea (20%), and incidentaloma (12%), but Cushing syndrome was rare. Seven patients with TSH-producing PAs had presented with visual problem (71.4%) and one goiter (14.3%) and remaining one case (14.3%) was incidentally found. Sixty three patients with plurihormonal PAs had been suffered from acromegaly (36.5%), visual problems (27.0%), headache, nausea and vomiting, and dizziness (20.6%), amenorrhea/galactorrhea (3.2%), and remaining was incidentalomas (12.7%). One hundred seventy nine patients with nonfunctioning PAs had been suffered from visual problems (45%), headache/nausea/dizziness (27%), amenorrhea/galactorrhea/dysmenorrhea (6%), and acromegaly (1%), but 20% was incidentalomas. The common symptoms and percent of incidentaloma are summarized in Table 4.
The median follow-up time for patients with PAs was 55.6 months (range: 2.7-72 months). During this follow-up period, 47 patients (11.1% of PAs) had tumor recurrence, most of them were surgically re-removed and some of them were treated by gamma knife surgery. Two most commonly recurrent tumors were nonfunctioning adenomas (4.0%) and FSH-producing tumors (2.1%). Six patients had more than two times tumor recurrence. In addition, 25.4% of patients with PAs were treated by gamma knife surgery due to residual tumor or regrowth of residual tumor, which produce successful control of residual PAs.
RCCs were also more common in women than in men (M:F =2:3.2). The mean age of patients with RCCs was 34.8 yr (range: 6-78 yr). RCCs were most common in patients in their teens and twenties (Fig. 3). The age distribution of patients with RCCs as compared with those with PAs is shown in Fig. 3. Inflammatory lesions were composed of chronic hypophysitis (n=3), cholesterol granulomas (n=3), chronic granulomatous inflammation (n=1) and aspergillosis (n=1).
DISCUSSION
The overall recorded incidence of PAs has been reported as 1 per 100,000, similar to the rate reported by the Central Brain Tumor Registry of the United States (http://www.cbtrus.org) (9). PA prevalence has been reported at 77.6 to 94±19.3 cases per 100,000 population in community-based cross-sectional studies (3, 4); women were more frequently affected than men (M:F=2.2: 5.9) (10). However, because few studies have reported these statistics for pituitary lesions in Korea, the exact incidence or prevalence of PAs in this population is unknown.
In one of the largest series of PA studies, Nilsson et al. collected samples from 2,279 patients over 34 yr and found that the age-standardized incidence of PA increased significantly from approximately 6 to 11 cases per million inhabitants from 1958 to 1991, suggesting that the annual incidence of PA is increasing (2). The median age was 52.3±15.7 yr (2). PA diagnosis was made by histological examination in 79.8%, radiological examination in 11.7%, clinical examination in 2.3%, postmortem histological examination in 5.4%, and surgery without histological examination in 0.7% of cases (2).
There are several reports about the natural history of nonfunctional PAs (11, 12). Men were more likely to present with multiple hormonal deficiencies than women (47% vs 28%), and premenopausal women tended to have smaller adenomas than men, but neither adenoma size nor invasion was associated with multiple hormonal deficiencies at presentation (12). Premenopausal women with nonfunctional PAs generally have favorable hormonal outcomes after operation: postoperative hormonal recovery was observed in over one-third of cases, with the greatest recovery being in the gonadal axis of 60% of premenopausal women (12). Despite the relatively high prevalence of incidentalomas and nonfunctional PAs, complications were fairly rare; however, functional adenomas and macroadenomas produce remarkable sequelae of late diagnosis or therapy-related adverse effects, such as visual field defects, hypopituitarism, or radiation change (4, 11). More accurate information about PAs may improve patient outcome in these cases.
Clinicopathologically, PAs are benign tumors, and can be classified as functional (hormone-secreting) or nonfunctional. They cause pituitary dysfunctions such as adenoma-related hypersecretion or mass effect-related hypopituitarism. In addition, patients often present with visual field defect or loss of visual acuity or diplopia by oculomotor dysfunction, especially in cases of cavernous sinus infiltration.
Fernandez et al. (4) carried out a community-based cross-sectional study in a small UK town and found the proportion of PRLoma in 44.4%, nonfunctioning PA in 22.2%, acromegaly (ACRO) in 8.6%, corticotroph adenoma in 1.2% and unknown functional status in 1.2%. The distribution of each PA subtype was PRLoma, 57%; nonfunctioning PA, 28%; ACRO, 11%; corticotroph adenoma, 2%; and unknown functional status, 2%. The median age at diagnosis (yr) and duration of symptoms until diagnosis (yr) were PRLoma, 32.0 yr and 1.5 yr; nonfunctioning PA, 51.5 yr and 0.8 yr; ACRO, 47 yr and 4.5 yr; corticotroph adenoma, 57 yr and 7 yr. PRLoma was the most frequent PA diagnosed up to the age of 60 yr, while nonfunctioning PA was most common after 60 yr of age. Nonfunctioning PA predominated in men (57% of all men with PA) and PRLoma in women (76% of all women with PA). Fernandez et al. (4) also concluded that PAs were 4 times more prevalent than previously thought.
Here, we evaluated only surgically resected, biopsy-proven pituitary lesions from a single hospital with immunohistochemical studies of pituitary hormones. In our series, the most common surgically resected pituitary lesion was PA (84.1%), similar to other reports (4). PA was 8.6 times more common than RCC (9.8%). PAs were most common in middle-aged female patients (mean age: 48.8 yr) (overall M:F=1: 1.7), except FSH-producing PA, for which there was male predominance (M:F=1:0.58). The mean age of patients with PAs was 14 yr older than that of RCCs. Immunohistochemical study in our series found that 57.6% of PAs were functional and the remaining PAs (42.4%) was nonfunctional, respectively. The most common functional PAs were PRL- (16.6%) and GH-producing adenomas (9.2%). The remaining PAs were FSH- (8.8%), ACTH- (5.9%), TSH- (1.7%), and LH- (0.5%) producing adenomas. The proportion of immunohistochemically nonfunctional PAs we found was much frequent than that of previously reported cases (42.4% vs 25%) but the proportion of the remaining subtype was similar to that of previously reported (Table 4) (6, 10, 13). Pleurihormonal PAs was 14.9%, which was also very similar to that of previous reports (up to 15.0%). In our series, the mean age at diagnosis was lowest in the patients with TSH-producing PAs (36.1 yr) and highest in those with FSH-producing adenomas (57.2 yr) (Table 1). The mean age at diagnosis of PRL- and GH-producing adenoma patients was 41.1 yr and 43.6 yr, respectively, and the mean age of patients with FSH-producing, and nonfunctioning PAs was the sixth decade (Table 2).
It is known that up to two third of the PAs presented with symptoms or signs of hormone excess. For example, thyrotropin (TSH)-secreting adenomas constitute approximately 1%-2% of all pituitary tumors, resulting in central hyperthyroidism characterized by diffuse goiter, elevated circulating levels of free thyroid hormones, and non-suppressed serum TSH. In rare cases, gonadotropin-secreting tumors may result in ovarian hyperstimulation, testicular enlargement, or precocious puberty. However, in our series, only one fifth of the patients with PAs presented with hormone associated symptoms and signs and most of them were PRLoma or GH-producing adenomas. Our cases of TSH and gonadotrophin-secreting PAs rarely showed the symptoms or signs of the hormone excess. Our patients with PAs presented with visual disorders (37.0%), abnormal hormonal effects (23.1%), headaches/nausea and vomiting or dizziness (23.0%), neurological deficits (1.9%), however, 15.0% of PAs were discovered incidentally (Table 3). Abnormal hormonal effects were presented in patients with 3 hormone producing PAs, which were GH (acromegaly/gigantism in 74.4%) and PRL-producing (amenorrhea/galactorrhea in 36%) and plurihormonal PAs (acromegaly in 36.5%) (Table 4). Since the remaining PAs did not show hormonal effect, immunohistochemical study is essential for the determination of hormonal subtype of PAs.
The treatment of choice for PAs is trans-sphenoidal surgical resection, which is a relatively safe treatment option. Transsphenoidal surgery carries a low risk of mortality and surgical complications; surgery can improve visual field defects in almost 80% of patients (14). Radiation therapy or gamma knife surgery is an option for recurrent tumors. The recurrence rate of PAs is usually not high (6.2%-19.8%), and has recently decreased remarkably (14-16). In our series, the recurrence rate after surgery was 11.1%; in particular, nonfunctional PAs had the highest recurrence rate. All recurrent or residual tumors in our series were removed by additional surgery or treated by gamma knife surgery (25.4%=107/422 cases). With gamma knife surgery, most of the residual or recurrent PAs were controlled.
In conclusion, we found that PAs were most common in middle-aged women and that PRL- and GH- producing and plurihormonal PAs were the most common functional adenomas at our hospital. Since the remaining PAs rarely showed hormonal symptoms and signs, immunohistochemical study is essential for the determination of hormonal subtype of PAs. The recurrence rate was 11.1% and the recurrence rate of the nonfunctioning and gonadotrophic hormone producing adenomas had higher than that of the other hormone producing PAs. The proportions of hormone-producing PAs and pituitary lesions in Korean patients were similar to those of previous reports except nonfunctioning (null cell) PAs which were more common in our series than previous reports (42.4% vs 25%) possibly due to specimen bias because we analyzed surgically resected and immunohistochemistry proven cases only.





 XML Download
XML Download