

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Portal hypertension (PHT) is a common clinical consequence of chronic liver disease that is characterized by a pathological increase in portal venous pressure and is associated with significant morbidity and mortality (1-3). Portal pressure can be increased by a rise in portal blood flow, an increase in vascular resistance, or both. In cases of cirrhosis, increased intrahepatic resistance to portal blood flow is the primary factor leading to PHT. Although this increase is largely attributable to the structural changes of the liver architecture caused by the cirrhotic process, there is also a dynamic and reversible component that represents up to 30%-40% of the total increased intrahepatic vascular resistance in cirrhosis (4). Various vasoactive substances contribute to the development of PHT. Among these, nitric oxide (NO) is one of the important mediators that paradoxically regulates the intrahepatic and splanchnic/systemic circulation (5-7). Splanchnic overproduction and intrahepatic deficit of endothelial NO contributes to the hyperdynamic circulation. Impairment of the endothelium-dependent response to vasodilatation, a condition that has been called "endothelial dysfunction", is considered one of the mechanisms that leads to the increased vascular tone of cirrhotic liver (8). Indeed, endothelial dysfunction has been attributed to reduced NO bioavailability and to increased vasoconstrictor cyclooxygenase-1 derived prostanoids (9, 10).
Tetrahydrobiopterin (BH4) is an essential cofactor for the adequate generation of NO by nitric oxide synthase enzymes (11-13). If adequate quantities of BH4 are not present, NOS uncoupling will occur and the production of NO is decreased. Previous studies have shown that there is a deficiency of BH4 in cirrhotic livers, secondary to a reduction in the expression and activity of the rate-limiting enzyme in BH4 synthesis, guanosine triphosphate-cyclohydrolase I (GTPCH), which is associated with decreased NOS activity and NO availability (14). In a study of carbon tetrachloride (CCl4)-induced cirrhosis in rats, the exogenous administration of BH4 for 3 days increased liver NOS activity and cyclic guanosine monophosphate (cGMP) levels and significantly reduced portal pressure (15). However, clinical studies of BH4 have not been conducted.
The present study evaluated the relationship between BH4 and PHT, the histological grades of hepatic fibrosis using the Laennec scoring system, the clinical stage of cirrhosis and the grade of varices. In addition, we investigated the relationship between PHT and clinical outcomes.
MATERIALS AND METHODS
Patients
A total of 204 patients were enrolled in this study. All patients were admitted to Wonju Severance Christian Hospital between December 2008 and January 2012 for the evaluation of chronic liver disease and received a liver biopsy. The exclusion criteria were as follows: age younger than 19 or older than 75 yr, shock status requiring a vasopressor, active infection (e.g., spontaneous bacterial peritonitis), acute renal failure of any cause, serum creatinine above 3.0 mg/dL, hepatocellular carcinoma or a history of another primary malignancy within 3 yr, underlying severe cardiac illness, transaminases above ten-fold the upper limit of normal, ongoing antiviral therapy, the use of vasoactive drugs (including beta-blockers, nitrates, diuretics and anti-inflammatory drugs), pregnancy or lactation and medical or psychological conditions that would not permit the subject to complete the study or sign the informed consent. Of the 204 patients, 11 patients were excluded from the study. The reasons for the exclusion were serum creatinine above 3.0 mg/dL (4 patients) and failure to measure BH4 (7 patients). A total of 193 patients (159 men and 34 women, mean age of 51.6±8.9, age range of 29-75 yr) were included in the study.
Liver biopsy and histomorphological analysis
Ultrasound-guided liver biopsies were conducted using a needle biopsy gun (Acecut, TSK laboratory, Tochigi, Japan) with a 16 gauge×11.5 cm needle and a 15 mm biopsy specimen notch. Five-micrometer-thick sections were prepared and were stained with hematoxylin and eosin and Masson-trichrome. A liver biopsy measuring at least 10 mm in length with a width of ≥1.2 mm was required for inclusion in this study. In the fragmented biopsies, the total length was approximated by adding the maximum dimensions of each individual fragment. The biopsies prospectively evaluated the degree of fibrosis and cirrhotic change according to the Laennec fibrosis scoring system (16). The Laennec fibrosis scoring system, a modification of the METAVIR system (17), scores fibrosis on a scale of 7 grades, with 0 indicating no definite fibrosis, 1-minimal fibrosis (no septa or rare thin septum; may have portal expansion or mild sinusoidal fibrosis), 2-mild fibrosis (occasional thin septa), 3-moderate fibrosis (moderate thin septa; up to incomplete cirrhosis), 4A-mild cirrhosis, definite or probable, 4B-moderate cirrhosis (at least 2 broad septa) and 4C-severe cirrhosis (at least 1 very broad septum or many minute nodules). In using the Laennec fibrosis scoring system, the thickness of the predominant type of septa in each specimen was chosen, and the smallest nodule was selected for scoring. Fibrosis was evaluated simultaneously and prospectively by a liver pathologist who was blinded to the clinical data.
Measurements of BH4
The BH4 level was measured using a high-performance liquid chromatography (HPLC) analysis after iodine oxidation in acidic conditions, as reported in a previous study (18). To measure the amount of biopterin, 100 µL of liver homogenate was used for acidic oxidation, followed by the addition of 100 µL of 0.2 N HCl. The homogenate was then incubated in the dark for 1 hr after 10 µL of an acidic iodine solution had been added (0.9% iodine and 1.8% potassium iodine in 0.1 N HCl). The reaction was terminated by the addition of 10 µL of 2% ascorbic acid. The centrifuged sample was then subjected to HPLC analysis. Concentrations were expressed as pM per mg of protein. The BH4 levels were derived by subtracting the biopterin levels under a basic oxidative state (biopterin+dihydrobiopterin [BH2]) from the levels under an acidic oxidative state (i.e., total biopterin=biopterin+BH2+BH4). The separation was performed on a Spherisorb ODS3 C18 (particle size 5 mm; length×internal diameter=250×4.6 of 1 mM GL Sci, Japan) using 10 mM Na2PO4 (pH 6.0) at a flow rate of 1.2 mL per minute. Pterins were detected by their native fluorescence (excitation wave length 350 nm, emission 450 nm) using a Hewlett-Packard model 1046A fluorescence detector.
Measurements of HVPG
After overnight fasting, the hepatic venous pressure gradient (HVPG) was measured. The right hepatic vein was catheterized percutaneously through the femoral vein, and the pressures in both the wedged and the free positions were recorded with a 7-F balloon-tipped catheter (Arrow Deutschland GmbH, Erding, Germany). In the case where a shunt was present in the right hepatic vein, HVPG was measured in the middle hepatic vein. All measurements were performed at least in triplicate, and permanent tracings were obtained on a multichannel recorder (19, 20). HVPG was determined by subtracting the free hepatic venous pressure from the wedged hepatic venous pressure (21). An examiner with 12 yr of experience with HVPG measurements performed all HVPG procedures.
Transient elastography
At the same day of measurement of HVPG, after overnight fasting, all patients underwent abdominal ultrasonography. Immediately following the ultrasonography examination, transient elastography was carried out by 2 experienced operators. The Fibroscan device (Fibroscan®, Echosens, Paris, France) consists of a 3.5 MHz ultrasound transducer M probe mounted on the axis of a vibrator. Mild amplitude and low-frequency vibrations (50 Hz) are transmitted to the liver tissue, inducing an elastic shear wave that propagates through the underlying liver tissue. Transient elastography was carried out on the right lobe of the liver, in the intercostal space with the patient lying in dorsal decubitus with the right arm at maximal abduction, as previously described (22, 23). The operator, assisted by an ultrasonic time-motion image, located a liver portion at least 6 cm thick and free of large vascular structures and the gallbladder. Ten successful measurements were performed on each patient. The success rate was calculated as the ratio of the number of successful measurements over the total number of acquisitions. Only liver stiffness measurements with an interquartile range of ≤30% of the median value and a success rate of at least 60% were considered reliable. The results are expressed in kilopascals (kPa) with the median value used to represent the liver stiffness measurement.
Esophagogastroduodenoscopy, imaging studies and laboratory parameters for clinical stage
Esophagogastroduodenoscopy, imaging studies (including ultrasonography and computed tomography) and laboratory tests were performed in all patients to determine the clinical stage of cirrhosis, model for end-stage liver disease (MELD) and the Child-Pugh score. The grades of esophageal varices were classified according to the classification of the Japanese Research Society for Portal Hypertension: F1, straight varices not disappearing with insufflations; F2, enlarged tortuous, occupying less than 1/3 of the lumen; and F3, coil-shaped, occupying more than 1/3 of the lumen. The clinical stage of cirrhosis was established by the presence or absence of varices, ascites, and bleeding, and it was classified into 4 stages as follows: stage 1, no varices; stage 2, varices and no ascites; stage 3, ascites±varices; and stage 4, bleeding±ascites. Stages 1 and 2 are compatible with compensated cirrhosis, but stages 3 and 4 are compatible with decompensated cirrhosis (24, 25). Laboratory parameters were obtained in all patients on the day of HVPG measurement and included serum albumin, bilirubin, alanine aminotransferase, aspartate aminotransferase, platelet count, hemoglobin, hematocrit, white blood cell count, International Normalized Ratio (INR), blood urea nitrogen, creatinine, electrolytes and C-reactive protein.
Statistical analysis
Statistical analysis was carried out using the IBM SPSS statistics 21. Categorical variables were expressed as proportions and compared using the chi-square and Fisher's exact tests, as appropriate. All results are expressed as the mean±standard deviation (SD). Normally or near-normally distributed variables were compared using Student's t-test. Non-normally distributed continuous variables were compared using the Kruskal-Wallis test. Linear regression analyses were conducted using the least squares method. One-way ANOVA was used to analyze the relationships among BH4, HVPG, hepatic fibrosis by Laennec fibrosis scoring system, BH+BH2/BH4 ratio, clinical stage of cirrhosis and Child-Pugh class. P values less than 0.05 were considered statistically significant.
Ethics statement
The study protocol was approved by the institutional review board for human research at the Yonsei University Wonju Severance Christian Hospital, Wonju, Republic of Korea (CR 109021). The nature of the study was explained to all patients, each of whom provided written informed consent before the beginning of the study, in accordance with the principles of the Declaration of Helsinki (revision of Edinburgh, 2000).
RESULTS
General characteristics of the patients
The general characteristics of the patients are summarized in Table 1. The etiology of chronic liver disease was classified as alcohol (n=136, 70.5%), hepatitis B virus (n=32, 16.6%), alcohol with hepatitis B virus (n=10, 5.2%), hepatitis C virus (n=4, 2.1%) alcohol with hepatitis C virus (n=1, 0.5%) or cryptogenic cirrhosis (n=10, 5.2%). The Laennec fibrosis stage was classified as F0 (n=3, 1.6%), F1 (n=3, 1.6%), F2 (n=12, 6.2%), F3 (n=22, 11.4%), F4A (n=25, 13.0%), F4B (n=74, 38.3%) or F4C (n=54, 28.0%). Cirrhosis was present in 153 of the 193 patients. The etiology of cirrhosis was classified as alcohol (n=105, 68.6%), hepatitis B virus (n=27, 17.6%), alcohol with hepatitis B virus (n=8, 5.2%), hepatitis C virus (n=3, 2.0%), or cryptogenic cirrhosis (n=10, 6, 5%). The clinical stage of cirrhosis was classified as stage 1 (n=39, 25.5%), stage 2 (n=44, 28.8%), stage 3 (n=45, 29.4%), or stage 4 (n=25, 16.3%). The mean Child-Pugh and MELD scores were 6.8±1.7 (range 5-12) and 10.4±3.7 (range 4-22), respectively. The mean HVPG was 14.5±4.9 (range 3-27).
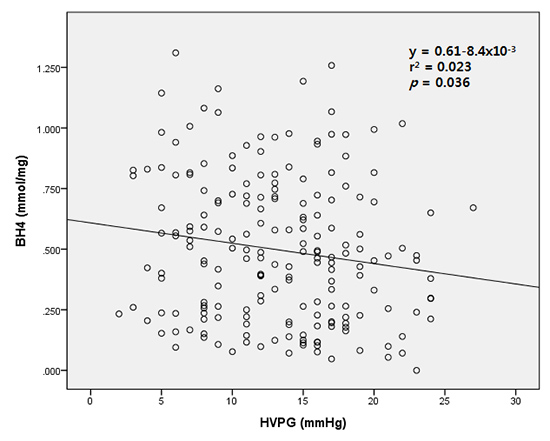
Relationship between BH4 and HVPG
Considering the whole patient population, a negative correlation between HVPG and BH4 was observed. Fig. 1 shows the linear regression analysis between HVPG and BH4 (r2=0.023, P=0.036). However, because the coefficient of determinant is 0.023, the linear regression fit is poor. Therefore, BH4 is not a useful predictor for HVPG.
Relationship between BH4 and the Laennec fibrosis scoring system
Fig. 2 shows the relationship between the Laennec fibrosis scoring system and BH4. The Laennec fibrosis score does not correlate with BH4. The mean BH4 levels in the F0 (n=3), F1 (n=3), F2 (n=12), F3 (n=22), F4A (n=25), F4B (n=74), and F4C (n=54) stages were 0.621±0.336 (range 0.223-0.826), 0.530±0.313 (range 0.205-0.830), 0.501±0.233 (range 0.095-0.886), 0.500±0.315 (0.077-1.082), 0.569±0.342 (0.077-1.310), 0.484±0.302 (0.047-1.258) and 0.472±0.298 (0-1.162), respectively (P=0.867). However, although not statistically significant, the mean BH4 levels showed a lower trend with increased hepatic fibrosis progression. In addition, higher hepatic fibrosis progression, a Laennec fibrosis score above 2, was associated with a higher trend in the mean BH+BH2/BH4 ratio. The mean BH+BH2/BH4 ratio in the F0, F1, F2, F3, F4A, F4B, and F4C stages were 0, 0.3±0.52 (0-0.09), 0.312±0.31 (0-0.913), 0.32±0.631 (0-2.927), 0.223±0.518 (0-2.343), 0.332±0.9 (0-7.623), and 0.398±0.545 (0-2.577), respectively (P=0.883).
Relationship between BH4 and clinical outcomes
Fig. 3A shows the relationship between BH4 and the Child-Pugh class. The Child-Pugh class does not correlate with BH4. The mean BH4 levels in the non-cirrhosis (n=40), Child A (n=83), Child B (n=58), and Child C (n=13) classes were 0.512±0.284 (range 0.077-1.082), 0.534±0.320 (range 0-1.31), 0.433±0.278 (range 0.047-1.067), and 0.5±0.298 (range 0.5±0.298), respectively (P=0.260). Fig. 3B shows the relationship between BH4 and the clinical stage of cirrhosis. The clinical stage of cirrhosis does not correlate with BH4. The mean BH4 levels in the non-cirrhosis (n=40), stage 1 (n=39), stage 2 (n=44), stage 3 (n=45), and stage 4 (n=25) cases were 0.512±0.284 (range 0.077-1.082), 0.561±0.315 (range 0.047-1.310), 0.509±0.345 (range 0.054-1.258), 0.453±0.272 (range 0-1.067), and 0.435±0.298 (range 0.071-0.994), respectively (P=0.405). The severity of esophageal varices does not correlate with BH4. The mean BH4 levels in the F0 (n=92), F1 (n=44), F2 (n=44), and F3 (n=13) stages were 0.496±0.290 (range 0-1.310), 0.501±0.312 (range 0.071-1.018), 0.511±0.311 (range 0.054-1.258), and 0.451±0.298 (range 0.071-0.962), respectively (P=0.938). However, although not statistically significant, there was an inverse relationship between the clinical stage of progression of cirrhosis and the mean BH4 levels.
Relationship between HVPG and clinical outcomes
HVPG significantly correlated with the Child-Pugh class. The mean HVPG in the non-cirrhosis (n=40), Child A (n=83), Child B (n=57), and Child C (n=13) classes were 8.2±3.8 (range 2-17), 12.8±4.9 (range 3-24), 16.4±4.2 (range 8-27), and 17.3±4.3 (range 8-24), respectively (P<0.001). Essentially, as HVPG increased, the Child-Pugh class also increased. HVPG also significantly correlated with the clinical stage of cirrhosis. The mean HVPG in non-cirrhosis (n=40), stage 1 (n=39), stage 2 (n=44), stage 3 (n=45), and stage 4 (n=25) cases were 8.2±3.8 (range 2-17), 11.1±3.7 (range 5-19), 14.4±4.9 (range 3-24), 16.8±4.8 (range 5-27), and 15.9±4.0 (range 5-24), respectively (P<0.001). Fig. 4 shows the relationship between HVPG and the Laennec fibrosis scoring system. The mean HVPG in the F0 (n=3), F1 (n=3), F2 (n=12), F3 (n=22), F4A (n=25), F4B (n=74), and F4C (n=54) cases was 2.7±0.6 (range 2-3), 4.7±1.2 (range 4-6), 8.0±3.8 (range 4-17), 9.6±3.4 (range 6-17), 11.2±5.0 (range 5-22), 14.3±4.4 (range 5-24), and 16.3±4.8 (range 3-27), respectively (P<0.001). A statistically significant, positive correlation between HVPG and liver stiffness was found by linear regression analysis (r2=0.402, P<0.001).
DISCUSSION
Intrahepatic vascular resistance is an important component of portal hypertension in chronic liver disease. Endothelial dysfunction in liver sinusoidal endothelial cells decreases the production of vasodilators, such as NO (26). The role of NO in the modulation of intrahepatic vascular resistance has been well demonstrated. eNOS dysfunction in sinusoidal endothelial cells and consequent reduction in NO production or bioavailability plays an crucial role (9, 10). Activation and contraction of hepatic stellate cells also contributes significantly to the dynamic component of intrahepatic vascular resistance. Activated hepatic stellate cells are more susceptible to vasoconstrictor substances than quiescent cells (27). Under condition of reduced NO production and/or impaired NO bioavailability in cirrhosis promotes hepatic stellate cells activation and contraction, leading to sinusoidal remodeling and elevation of the intrahepatic vascular resistance.
NOS are enzymes that catalyze the formation of NO from L-arginine. BH4 is an essential cofactor for endothelial NOS. A previous study using an animal model showed that there is a deficiency of BH4 in cirrhotic livers, secondary to a reduction in the expression and activity of GTPCH (the limiting enzyme in BH4 synthesis), which is associated with decreased NOS activity and NO availability (14). Another in vivo study showed that 3 day supplementation with exogenous BH4 decreased portal pressure in cirrhotic rats (15). However, there has not been any clinical study conducted to evaluate BH4 in human cases. Therefore, we evaluated the relationship between BH4 and HVPG, Laennec fibrosis scoring system, Child-Pugh class and clinical stage of cirrhosis in humans.
In the present study, although HPVG showed a statistically significant correlation with clinical outcomes, including Child-Pugh class, clinical stage of cirrhosis, Laennec fibrosis scoring system and liver stiffness measurement, there is no relationship between BH4 and HVPG. Even though linear regression analysis showed P value smaller than 0.05 for the relationship between BH4 and HVPG, the respective values are widely scattered in the central value as well as very low R square value (0.023), as shown in Fig. 1. It thought to be the statistical limitation that can occur in a large number of subjects. Additionally, BH4 does not correlate with clinical outcomes, including Laennec fibrosis scoring system, Child-Pugh class, clinical stage of cirrhosis and severity of esophageal varices. There is no clear explanation for these results, but several possibilities can be considered.
First, if liver fibrosis progresses past a specific degree, BH4 may not decrease further. In vascular disease, BH4 bioavailability can be limited by superoxide production by various oxidases, forming peroxynitrite and other reactive oxygen species that oxidize BH4 (28). As a result, peroxynitrite and other reactive oxygen species oxidize BH4, via BH2 and BH, which reduces the bioavailability of BH4 and promotes eNOS uncoupling. eNOS then generates superoxide rather than NO, which further reduces NO bioavailability. Through this cycle, if BH4 decreases below a certain level, the progression of hepatic fibrosis will not have an impact on the reduction of BH4.
Second, the ratio of BH4 to oxidized biopterins is as important as absolute BH4 in the determination of eNOS activity. In a study of diabetic mice, endothelial dysfunction was shown to be associated with reduced BH4 levels, but no changes in total biopterins were observed, suggesting that BH4 is oxidized to biologically inactive dihydrobiopterin (BH2) and biopterin (BH) (29). In cirrhosis, the reduced/oxidized pterin ratio (BH4/[BH2+ BH]) has been shown to be markedly reduced in livers from rats with cirrhosis compared with control livers (15). Similarly, although not statistically significant, the present study also showed a direct positive association between hepatic fibrosis progress above a Laennec fibrosis score of 2 and the mean BH+BH2/BH4 ratio.
Third, many substances and drugs interact with BH4. The final step in BH4 biosynthesis is the reduction of 6-pyruvoyltetrahydropterin by sepiapterin reductase (SPR). Recently, several studies showed that sulfasalazine, antibacterial sulfa drugs and antidiabetic sulfonylureas are potent inhibitors of SPR and inhibit the biosynthesis of BH4 (30, 31). Additionally, another study has shown that glucocorticoids inhibit the expression of GTPCH (the rate-limiting enzyme for BH4 synthesis) (32). Metals, including aluminum, cadmium, mercury, lead and manganese, can also affect BH4 biosynthesis by dihydropterin reductase (DHPR) activity. BH4 is mainly regenerated by DHPR (33, 34). In contrast, one study demonstrated that fluvastatin potentiates GTPCH gene expression and BH4 synthesis, thereby increasing NO production and preventing relative shortages of BH4 (35). Additionally, both eplerenone (selective aldosterone antagonist) and enalapril (angiotensin converting enzyme inhibitor, ACEI) reduce NADPH oxidase activity, elevate vascular BH4 levels, and enhance eNOS expression and NO bioavilability (36). Additionally, several studies showed the presence of a chemical interaction between ascorbic acid and BH4 (37, 38). In regard to these data, BH4 concentrations can be affected by sulfa drugs, glucocorticoids, metals, statins, ACEI and vitamin C.
Fourth, in addition to BH4, there are many mechanisms for decreased hepatic NO synthesis in cases of cirrhosis. Increased caveolin expression (cholestasis), decreased Akt-p dependent eNOS phosphorylation, scavenging of NO by superoxide (consequence of reduced superoxide dismutase activity) and increased levels of asymmetric-malondialdehyde (MDA, a serum marker of oxidative stress) all contribute to decreased hepatic NO synthesis in cirrhosis (39).
Finally, in addition to endothelial dysfunction, cyclooxygenase (COX)-derived prostanoids and abnormal angiogenesis could also contribute to increased intrahepatic resistance in portal hypertension. An increased production of a COX-1 derived vasoconstrictor prostanoid has been shown to be responsible for the presence of endothelial dysfunction in liver cirrhosis (10). Additionally, recent studies have demonstrated that angiogenesis plays a critical role in the development and maintenance of splanchnic hyperemia and portosystemic collateralization (40). Multifactorial mechanisms are involved in decreased hepatic NO synthesis in chronic liver disease.
In conclusion, the present study demonstrated that there is no relationship between BH4 and portal hypertension or clinical outcomes in patients with chronic liver disease. BH4 concentrations can be influenced by various substances and drugs. Furthermore, in addition to hepatic endothelial dysfunction with NO, various other factors also affect the development and progression of PHT.




 XML Download
XML Download