

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In the USA, more than 70,000 new cases of bladder cancer were diagnosed and at least 14,000 patients died from bladder cancer (1). Almost 25% of newly diagnosed patients have muscle invasive bladder cancer (MIBC) and nearly 50% of these patients already have occult distant metastases at the time of diagnosis. The standard mode of treatment for MIBC is radical cystectomy. However, despite improvement in surgical techniques, 5-yr disease-free survival after radical cystectomy remains between 55% and 65% (2, 3). The reason for such a low 5-yr survival rate for radical cystectomy is presumably due to clinical understaging and micrometastasis (4).
Stage and grade are well established predictors for survival in MIBC (5). Hence, clinicians have usually used these parameters for counseling of patients and decision of treatment. However, despite the same treatment, there are differences in survival outcomes for patients with the same stages and grades. Therefore, various studies for molecular markers have attempted to improve the survival rates and predicted outcomes.
Recently, interest has grown in the use of microarray-based gene expression profiling for predicting the survival and outcomes for individual cancer patients (6). High-throughput microarray technology can be used to investigate the RNA expression levels of hundreds of thousands of genes, and it can provide comprehensive insight for molecular levels of human cancer (7). Using this technology, numerous genetic markers have been found and validated as diagnostic and prognostic indicators. Already, microarray-based breast cancer analysis is a useful tool in predicting the response to hormonal treatment, the response to target therapy, and in estimating survival for breast cancer patients (8). For cases of MIBC, however, there have been only a few reports of the use of microarrays to successfully predict survival rates (9).
In a previous study, we investigated gene expression profiling in bladder cancer patients, and uploaded the full microarray data set at http://www.ncbi.nlm.nih.gov/geo/ with the data series accession number GSE13507. Using this data, we selected 3 candidate genes (USP18, DGCR2, ZNF699) and evaluated whether their identification by microarray-based gene expression profiling could be associated with cancer-specific survival in MIBC patients.
MATERIALS AND METHODS
Bladder cancer micro-array data
Micro-array gene-expression profiling techniques have been described in previous reports (10). Briefly, we used 165 primary bladder cancer samples, 23 recurrent non-muscle invasive tumor tissues, 58 normal-appearing bladder mucosa surrounding cancer, and 10 normal bladder mucosa for micro-array analysis. Unsupervised hierarchical clustering analysis was used to stratify the prognosis-related gene classifiers. The full microarray data set is available online at http://www.ncbi.nlm.nih.gov/geo/ under the data series accession number GSE13507.
Patients and tissue samples
Sixty-two patients with MIBC were selected by micro-array profiling (original cohort). We collected new tumor specimens from 118 MIBC patients with histologically verified urothelial cell carcinoma (UCC) as a validation cohort. To reduce confounding factors affecting the analyses, and to delineate a more homogenous study population, we excluded patients diagnosed with a concomitant carcinoma in situ (CIS), or for whom data collection was incomplete. All tumors were macro-dissected, typically within 15 min of surgical resection. Each bladder cancer specimen was confirmed by pathological analysis of a part of the tissue sample in fresh-frozen sections from cystectomy and transurethral resection (TUR) specimens, then frozen in liquid nitrogen and stored at -80℃ until use.
Tumors were staged and graded according to the 2002 TNM classification and the 1973 WHO grading system, respectively (11, 12). Patients with localized or locally advanced tumors and good ECOG performance status (0 or 1) underwent radical cystectomy and complete pelvic lymph node dissection. Patients who were not eligible for radical cystectomy due to metastatic disease, poor life expectancy, or poor ECOG performance status (=2) underwent TUR for histopathological diagnosis. Patients with pT3, pT4 or node-positive disease based on the analysis of radical cystectomy specimens, or with metastatic disease but good performance status, received at least four cycles of cisplatin-based chemotherapy. Each patient was followed and managed according to standard protocol (13).
RNA extraction and construction of cDNA
Total RNA was isolated from tissue using 1 mL of TRIzol (Invitrogen, Carlsbad, CA, USA) and homogenization in a 5 mL glass tube. The homogenate was transferred to a 1.5 mL tube and was mixed with 200 µL chloroform. After incubation for 5 min at 4℃, the homogenate was centrifuged for 13 min at 13,000 g and 4℃. The upper aqueous phase was transferred to a clean tube and 500 µL isopropanol was added, followed by incubation for 60 min at 4℃. The tube was then centrifuged for 8 min at 13,000 g and 4℃. Then, the upper aqueous phase was removed, mixed with 500 µL of 75% ethanol, and centrifuged for 5 min at 13,000 g and 4℃. After the upper aqueous layer was discarded, the pellet was dried at room temperature, dissolved with diethylpyrocarbonate (DEPC)-treated water, and stored at -80℃. The quality and integrity of the RNA were confirmed by agarose gel electrophoresis and ethidium bromide staining, followed by visual examination under ultraviolet light. cDNA was then prepared from 1 µg of total RNA using a First-Strand cDNA Synthesis Kit (Clontech, TAKARA, Otsu, Japan) according to the manufacturer's protocol.
Real-time PCR
To quantify the mRNA expression levels, real-time PCR amplification was performed using a Rotor Gene 6000 instrument (Corbett Research, Mortlake, Australia). Real-time PCR assays using SYBR Premix EX Taq (TAKARA BIO INC., Otsu, Japan) were carried out in micro-reaction tubes (Corbett Research). Primers were used to amplify USP18, DGCR2, and ZNF699. PCR reaction was performed in a final volume of 10 µL, consisting of 5 µL of 2×SYBR premix EX Taq buffer, 0.5 µL each of 5'- and 3'-primer (10 pM/µL), and 2 µL of the sample cDNA. The product was purified with a QIAquick Extraction kit (QIAGEN, Hilden, Germany), quantified with a spectrometer (Perkin Elmer MBA-2000, Fremont, CA, USA), and sequenced with an automated laser fluorescence sequencer (ABI PRISM 3100 Genetic Analyzer, Foster City, CA, USA). The known concentration of the product was 10-fold serially diluted from 100 pg/µL to 0.1 pg/µL. The dilution series of PCR products was used for establishing the standard curve of real-time PCR. The real-time PCR conditions were 1 cycle at 96℃ for 20 sec, followed by 40 cycles of 3 sec at 96℃ for denaturation, 15 sec at 60℃ for annealing, and 15 sec at 72℃ for extension. The melting program was performed at 72-95℃ with a heating rate of 1℃ per 45 sec. Spectral data were captured and analyzed using Rotor-Gene Real-Time Analysis Software 6.0 Build 14 (Corbett Research). All samples were run in triplicate. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was applied as an endogenous RNA reference gene. Gene expression was normalized to the expression of GAPDH.
Statistical analysis
To normalize the highly skewed distribution of the mRNA expression of each gene, the data were natural-log transformed and then back-transformed for an interpretation of the results. The association between cancer-specific survival and the gene signatures was evaluated using univariate Cox regression analysis. Cancer-specific and overall survival was calculated according to the Kaplan-Meier method, with differences between the times assessed using log-rank statistics. After univariate Cox analysis of the three candidate genes, two were used to calculate a risk score of cancer-specific death for each patient, defined as the sum of the levels of expression of each gene multiplied by the corresponding regression coefficient (14, 15). Receiver operating characteristic (ROC) curves were used to identify the optimal cutoff point of each risk score that yielded the highest combined sensitivity and specificity for cancer-specific survival. Based on these values, patients were classified into either a good-prognostic or a poor-prognostic gene signature group. The prognostic value of the combination of gene expression was determined by univariate and multivariate Cox proportional hazard regression models. Statistical analyses were performed using SPSS ver. 19.0 (SPSS Inc., Chicago, IL, USA), and P values of less than 0.05 were considered statistically significant.
Ethics statement
The study protocol was approved by the institutional review board of Chungbuk National University (IRB approved number 2006-01-001). Informed consent was obtained from each subject.
The biospecimens for this study were provided by the Chungbuk National University Hospital, a member of the National Biobank of Korea, which is supported by the Ministry of Health, Welfare and Family Affairs. All samples derived from the National Biobank of Korea were obtained with informed consent under institutional review board-approved protocols.
RESULTS
Cancer-specific survival-related gene classifiers
In microarray analysis, we chose 21 candidate genes that showed highly significant differences between low and high mRNA expression groups in 62 patients with MIBC. And then, candidate genes were selected using Kaplan-Meier analysis and a log rank test (P<0.01, respectively). Finally, 3 candidate genes (USP18, DGCR2, ZNF699) were selected (P=0.002, P=0.008, and P=0.002, respectively).
Baseline characteristics
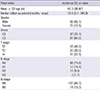
The mean age of the 118 subjects with primary MIBC was 67.3 (38-87) yr, and the median follow-up period was 16.9 (2.1-180.9) months. Eighteen patients (15.3%) had metastases. Other baseline characteristics of the patients are presented in Table 1.
Identification of genes associated with cancer-specific death in MIBC patients
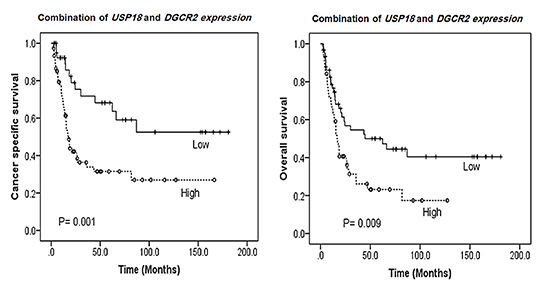
Univariate Cox regression analysis was performed for three genes (USP18, DGCR2, ZNF699), which were previously selected by microarray analysis. Two of them, USP18 and DGCR2, were significantly correlated to cancer-specific death (P=0.020, P=0.007, respectively). Cancer-specific survival was significantly different between the high and low USP18 or DGCR2 mRNA expression groups, in that cancer-specific survival in the low USP18 or DGCR2 expression group was significantly longer than that in the high expression group (P=0.018, P=0.006, respectively) (Fig. 1). Also, overall survival in the low USP18 or DGCR2 expression group was significantly longer than that in the high expression group (P=0.015, P=0.008, respectively) (Fig. 2).
USP18 and DGCR2 mRNA expression level according to clinicopathological parameters
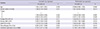
The mRNA expression of USP18 was significantly higher in patients with lymph node involvement (P<0.001) or grade 3 (P=0.013). The mRNA expression of DGCR2 was significantly higher in patients with lymph node involvement (P=0.034) (Table 2). There were no significant differences between USP18 and DGCR2 for other clinicopathological parameters such as T stage and M stage.
The value of the combination of USP18 and DGCR2 mRNA expression level as a prognostic marker for cancer-specific survival
These two genes were then used to calculate a risk score for cancer-specific death in MIBC patients. The risk score identified two groups of patients. A good-prognostic signature group represented relatively low expression levels of the two genes, while a poor-prognostic signature group had a significantly higher expression. Using a ROC curve, a cutoff value (46.6093) was determined for cancer-specific death with the highest combined sensitivity (77.6%) and specificity (50.0%). In univariate Cox regression analysis of clinicopathological variables, age, T4, positive lymph node, metastasis, and a combination of USP18 and DGCR2 mRNA expression levels were significant risk factors for cancer-specific death (P=0.035, P=0.005, P=0.011, P=0.006, and P=0.001, respectively). In multivariate Cox regression analysis, T4, metastasis, chemotherapy, and a combination of USP18 and DGCR2 mRNA expression levels were significant prognostic factors for cancer-specific death (HR, 2.587; CI, 1.357-4.933, P=0.004; HR, 2.376; CI, 1.160-4.866, P=0.018; HR,0.459; CI, 0.240-0.875, P=0.018, and HR, 2.106; CI, 1.043-4.254, P=0.038, respectively) (Table 3). Overall survival and cancer-specific survival in the low expression group was significantly longer than that in the high expression group (P=0.001, both) (Fig. 1C and Fig. 2C).
DISCUSSION
In the present study, the combined expressions of USP18 and DGCR2 were used to predict cancer-specific survival in patients with MIBC, which was reconfirmed by validation in different cohorts. In MIBC, pathological tumor characteristics such as lymph node involvement, tumor stage, grade, and histological subtype have been established as significant predictors of outcomes (16). Also, clinical factors such as time from diagnosis to surgery, patient age, and gender are considered to be important predictors of outcome (16). To improve the accuracy of predicting outcomes, several nomograms that include pathological tumor characteristics and clinical factors have been used (17, 18). However, the heterogeneity of the biological behaviors of tumors may limit the accuracy of predicting the outcome of nomograms based on clinical and pathological characteristics. Accordingly, there is growing interest in a molecular biomarker for predicting tumor aggressiveness and patient outcomes. p53 expression has been associated with tumor stage, grade, lymph node metastasis, and cancer-specific death (19). Also, p27 and Ki-67 could be used as predictive markers for recurrence and survival in MIBC patients who have undergone radical cystectomy (19). Bcl-2, caspase-3 and survivin were found to be associated with grade, stage, metastasis, and survival (20). Vascular endothelial growth factor (VEGF), basic fibroblast growth factor (FGF) and thrombospondin-1 have been used as independent predictors of clinical outcomes in bladder cancer patients (21, 22). However, a single molecular biomarker cannot reflect tumor biology due to the complexity of tumorigenesis. Therefore, the trend for predicting prognostic value has changed to the simultaneous assessment of multiple biomarkers in cancer patients (23). Similarly, this study was carried out to predict outcomes after the assessment of 2 biomarkers (USP18 and DGCR2) in MIBC.
Ubiquitin specific peptidase 18 (USP18) is a cysteine protease that is known to remove interferon stimulated gene 15 (ISG15), a ubiquitin-like protein family member, from conjugated proteins (24, 25). Duex et al. (26) reported that USP18 regulates epidermal growth factor Receptor (EGFR) expression and cancer cell survival. Inhibition of USP18 reduces the levels of EGFR and other oncogenic proteins and inhibits the tumorigenic activity of cancer cells. Interestingly, in bladder cancer, elevated EGFR expression has been strongly associated with a decrease in the rate of relapse-free survival (27). Certainly, low USP18 reduced the levels of EGFR and inhibited the tumorigenic activity of cancer cells, and then, increased the survival of cancer patients. In the present study, we also demonstrated that compared with a high expression group, a low USP18 expression group was indicative of significantly longer rates of overall and cancer-specific survival. DGCR2 (DiGeorge syndrome critical region gene 2) is a putative adhesion receptor that is expressed in the embryo during early development and is believed to play a role in the development of the nervous system (28). Generally, mutations in this gene are associated with DiGeorge syndrome and velocardiofacial syndrome. The manifestations of this syndrome are immune deficiencies, cardiac anomalies, renal anomalies, eye anomalies, hypoparathyroidism, skeletal defects, and developmental delay (29). Recently, additional reports have associated this gene with schizophrenia and shown it to be a novel marker for pancreatic beta cell-specific proteins (30). Thus far, there has been no report about the relationship between DGCR2 and cancer biology. In the present study, we showed that DGCR2 expression is associated with survival in MIBC. DGCR2 is likely to be associated with neuroendocrine differentiation of bladder tumors, which would mean it could be associated with poor prognosis in cancer patients. Interestingly, the present study is the first to examine the relationship between DGCR2 and survival in cancer patients.
Taken together, USP 18 and DGCR2 are associated with survival in cancer patients. Our results show that these two genes could be important prognostic markers in MIBC. Further studies, including a functional study, are necessary to consolidate these results.
In conclusion, decreased expressions of USP18 and DGCR2 were significantly associated with a longer rate of cancer-specific survival, and also the combination of these two genes was correlated with longer survival rates in MIBC. Thus, the combination of USP18 and DGCR2 expression is a reliable predictor for cancer-specific survival in MIBC.



 XML Download
XML Download