

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Radiofrequency catheter ablation is a common technique used worldwide to treat typical atrial flutter. Complications related to catheter ablation include vascular thrombosis, complete atrioventricular block, and cardiac tamponade. Acute coronary artery occlusion is a rare but potentially serious complication of the procedure, and has not been previously reported in Korea.
We report a case of acute right coronary artery thrombosis and ST-segment elevation myocardial infarction occurred immediately after radiofrequency catheter ablation of typical atrial flutter, which was successfully treated with immediate coronary intervention.
CASE DESCRIPTION
A 53-yr-old man with persistent atrial flutter (Fig. 1) was admitted on August 20th 2012, to undergo radiofrequency catheter ablation. He was given intravenous heparin continuously until 6 hr before the procedure. Transesophageal echocardiogram did not show evidence of intracardiac thrombus two days before the procedure. After obtaining informed consent, he was brought to our electrophysiology laboratory after fasting for 8 hr. Under local anesthesia using lidocaine after sterile draping, two quadripolar electrode catheters (St. Jude Medical, Inc., St. Paul, MN, USA) were positioned to record the activity of the bundle of His and the right ventricular apex. The high right atrium (RA), mid RA, and coronary sinus (CS) were mapped with a deflectable duo-decapolar catheter (St. Jude Medical) (Fig. 2A). Intracardiac electrograms were recorded using a Prucka CardioLab™ electrophysiology system (General Electric Health Care System, Inc., Milwaukee, WI, USA). His baseline intracardiac electrogram showed typical counterclockwise atrial flutter (Fig. 2B). A 7Fr, 4mm-tip irrigation ablation catheter (St. Jude Medical, Inc., St. Paul, MN, USA) was inserted through an 8Fr, 60 cm-long RAMP sheath (St. Jude Medical, Inc., St. Paul, MN, USA). Radiofrequency current was applied to the posteroseptal side of the cavotricuspid isthmus, with temperature limit of 35℃ and power of 30-35 W (Fig. 2A). As atrial flutter persisted after enough ablation, we started making ablation lines at the posterolateral side of the isthmus. Atrial flutter was suddenly terminated while making the first ablation line at the posterolateral side. To ensure successful ablation, radiofrequency energy was delivered six more times. Bidirectional isthmus block was confirmed. During the procedure, the patient complained of chest pain, but we considered it to be related to the ablation itself, because there was no change in the electrocardiogram and because the pain was not severe.
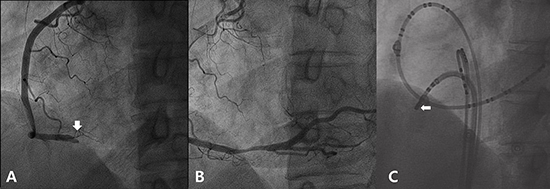
When he returned to the ward, he reported worsening chest pain. We obtained a 12-lead electrocardiogram, which showed ST-segment elevation in leads II, III, aVF, and V5-6 and ST depression in leads I, aVL, and V1-4, suggesting acute myocardial in farction of the inferior wall (Fig. 3). He was immediately brought to the catheterization laboratory. Coronary angiography showed total occlusion at the distal portion of the right coronary artery, which was close to the area of ablation (Fig. 4). We aspirated red thrombi from the artery. After intracoronary injection of abciximab, balloon dilatation with a 3.0×20 mm balloon with a maximum pressure of 10 ATM was done with 20% residual stenosis. His chest pain was immediately relieved. After an hour, the elevated ST segments in leads II, III, aVF, and V5-6 returned to baseline. Cardiac troponin I peaked at 145.92 ng/mL 10 hr later.
The patient did not experience chest pain up to the time of discharge. However, approximately 21 hr after the completion of radiofrequency ablation, atrial flutter recurred. As it did not return to sinus rhythm with intravenous amiodarone, and because he developed hypotension 2 hr later, we performed electrical cardioversion with 70 J to achieve sinus conversion. To maintain the sinus rhythm, oral amiodarone 200 mg once daily was prescribed. Five days later, he was discharged without any symptoms as sinus rhythm persisted. After a year, he is still in sinus rhythm and has not experienced any kind of chest pain.
DISCUSSION
To our knowledge, there have been five similar cases of right coronary artery occlusion during or after cavotricuspid isthmus ablation for typical atrial flutter (1-5), but the exact mechanism is still unclear. After reviewing the literature, we suggest several hypotheses for the mechanism of coronary artery occlusion in this patient.
There was one case of a man who died of heart failure and pneumonia 3 weeks after an isthmus ablation for typical atrial flutter in whom right coronary artery histology showed an intramural hematoma adjacent to the ablation site (1). The anatomical proximity of the right coronary artery to the cavotricuspid isthmus (6) and evidence of inflammatory changes in the right coronary artery after radiofrequency ablation in young pigs (7) implies the possibility of direct thermal injury to the right coronary artery wall from the radiofrequency energy used in cavotricuspid isthmus ablation. This injury could result in partial tearing of the vascular wall, formation of an intramural hematoma, and rupture into the vascular lumen. Considering the tip of the ablation catheter was close to the occlusion site of the right coronary artery (Fig. 4), this could have been the cause of myocardial infarction in this case.
Simon et al. (8) reported three cases of coronary artery vasospasm during radiofrequency ablation in the left atrium, all of which were resolved with intracoronary or intravenous nitrate infusion. A study by Yamashita et al. showed vasoconstriction of the right coronary artery shortly after left atrial catheter ablation for atrial fibrillation. Although these were different ablation sites than our case, they raise possibility of similar phenomena occurring with radiofrequency ablation of other sites. Based on a number of case reports from Japan (9-13), intracoronary thrombosis concomitant with severe vasospasm of the coronary artery may be another explanation for myocardial infarction in Cthis patient. However, an ergonovine provocation test was not performed to diagnose coronary artery spasm because he denied previous chest pain, suggesting variant angina, and because he needed urgent coronary revascularization.
Although thromboembolism can also induce coronary artery occlusion theoretically, the possibility is very low in this case because we confirmed the absence of a left atrial thrombus and continued intravenous heparin until 6 hr before the procedure.
Whatever the real mechanism is, it seems clear that this is an example of collateral damage during radiofrequency ablation, as are other complications like atrioventricular block or cardiac tamponade. To avoid this potentially fatal complication, novel techniques to precisely target the lesion with minimal radiofrequency energy while preventing injury to adjacent structures are essential. Although it is not clear if the patient in this case had underlying atherosclerotic disease in the coronary arteries, no other lesion was seen on coronary angiography except the one close to the ablation site, and he did not experience any kind of chest pain. Physicians should always be aware of this kind of complication, even in patients without known coronary artery disease, and monitor the 12-lead electrocardiogram during the procedure, especially when the patient complains of chest pain.



 XML Download
XML Download