

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Patient-centered care encompasses the physician's response to the preferences of patients regarding treatment (1). Several studies have reported that patients generally prefer to be informed and involved in the decision-making (2, 3), and several medical specialties have evaluated patient preferences for participation in decision-making in their treatment management (4-9).
In the perioperative period, anesthesiologists have multiple options with regard to the choice of anesthetic method, monitoring and use of drugs to achieve the desired outcome. The choice of anesthesia depends on the patients' underlying disease, laboratory findings, general condition, surgery type and duration. Some patients have factors that could influence the choice of anesthesia, but some have no factors. Recently, anesthesiologists have made an effort to involve the patients or their families in the decision-making process regarding the anesthesia options, however there is a lack of data about the effect of patient involvement in the decision-making for the anesthetic method used for surgery.
The purpose of this prospective study was to evaluate the patients' decision-making preferences for selecting the anesthetic method, patient satisfaction regarding their involvement in the decision-making, and the preferred anesthetic methods of the patients. Additionally, we evaluated the change in the patients' decision-making preference after experiencing this decision-making process.
MATERIALS AND METHODS
Study population
All patients scheduled for elective surgery aged 20 yr and above were included in the study. The patients had no factors that could influence the choice of anesthesia for their surgery, and all surgeries were simple and performed in the upper and lower extremities. Patients were excluded based on the following criteria: an inability to consent to participate in the study, < 20 yr of age, > 100 kg, a Mallampati class IV oral opening, a history of alcohol or drug abuse, mental incompetence, preexisting coagulopathy, neuropathy or allergy to local anesthetic agents.
Explanation of anesthetic methods for surgeries
Patients undergoing simple surgeries involving the upper or lower extremities were included in this study. For a standardized description, only one anesthesiologist who is an assistant professor of Department of Anesthesiology explained to the patients and their families the physical status, preoperative study findings and possible anesthetic methods for their surgeries. The anesthesia method options were: ultrasound-guided brachial plexus block versus general anesthesia in cases involving upper extremities, and spinal anesthesia versus general anesthesia in cases involving the lower extremities. Patients received brochures about these anesthetic methods and listened to a detailed explanation regarding the advantages/disadvantages and complications of the two anesthetic methods for their respective operations. After receiving the pre-anesthesia information, patients participated in selecting the anesthetic method for their surgery.
Study design and measurement
The aim of this study was to evaluate the patients' decision-making preferences for selecting the anesthetic method and the level of patient satisfaction regarding the decision-making process. To evaluate the preferences, we reviewed the shared decision-making model conceptualized by Charles et al. (10, 11). This conceptualization highlights the importance of three components to the decision-making process: information exchange, deliberation and selection of treatment method. In this study, our anesthesiologists modified the decision-making model. In the information exchange stage, both the physician and patient shared information (i.e., the anesthesiologists explained the relevant information to the patients who participated in this study about the physical status, preoperative study findings, and two possible anesthetic methods for their surgeries; the patients provided information to the physicians regarding their decision-making preference, life style, needs and specific situations).
After sharing information and listening to a detailed explanation from an anesthesiologist of the two anesthetic methods, all patients deliberated and selected one of the following decision-making models: 1) I prefer to make a decision by myself with my family; active role, 2) I prefer to discuss and make a decision together with an anesthesiologist; collaborative role, or 3) I prefer to rely on the anesthesiologist's decision; passive role. Finally, the patients decided upon the anesthetic method with (collaborative and passive role) or without (active role) an anesthesiologist.
On the postoperative visit at 24 hr after the operation, each patient was asked about their level of satisfaction and feelings of respect regarding their involvement in the anesthesia decision-making for their surgery. Additionally, to evaluate the change in the patients' decision-making preference after being involved in this decision-making process, the patients were asked which decision-making models for their anesthesia they would prefer or choose if they were to undergo the same surgery again.
Statistical analysis
All analyses were performed using the SPSS software (ver. 12; SPSS, Chicago, IL, USA), and statistical significance was set at P<0.05. Using Pearson's chi-square test, associations among the preferred decision-making role in the selection of the anesthetic method were analyzed with respect to age, sex, education level and past anesthetic history. Using the McNemar-Bowker test, the differences between the patients' preferred decision-making role for anesthesia during the current surgery were compared with the preferred role for decision-making for anesthesia during future surgeries.
RESULTS
Of the 257 total patients, 179 (69.6%) preferred to play a collaborative role, 47 (18.3%) preferred an active role, and 31 (12.1%) preferred a passive role in the decision-making process in selecting their anesthetic method. Table 1 summarizes the demographic data of the subjects, the preferred decision-making role in selecting an anesthetic method, and the associations with age, sex, education level and past anesthetic history. These variables differed significantly with age. In contrast to patients aged 20-50 yr of age, those between 50 and 60 yr of age showed a tendency to prefer an active or passive role rather than a collaborative role. Other variables showed no significant differences.
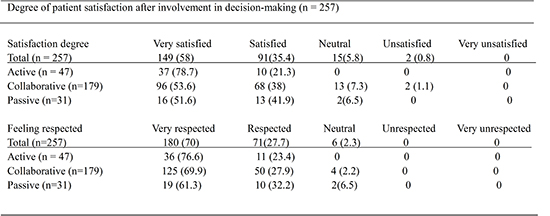
Table 2 shows the degree of patient satisfaction, the feeling of being respected in the decision-making process. Although 31 (12.1%) patients chose a passive role, they were asked questions about satisfaction and feeling respected, also. Table 3 shows the preferred anesthetic methods of the patients who choose a collaborative role and an active role. Because 31 patients (18 upper extremity, 13 lower extremity patients) who chose a passive role were excluded, 226 patients was the total number of patients of this result. Table 4 shows the difference between the patients' preferred decision-making role for the current use of anesthesia and the changed preference for a role in selecting anesthesia in the future.
DISCUSSION
The pioneer of patient-centered care, Dr. Harvey Picker, stated that understanding and respecting patients' values, preferences, and expressed needs are the foundation of patient-centered care (12, 13). Patient-centered care customizes the treatment recommendations on the basis of informed shared decision-making, development of patient knowledge, enhancement of skills needed for self-management of illness and preventive behaviors (10). The traditional clinician-centered and disease-focused approaches to illness are believed to be less effective than patient-centered, biopsychosocial approaches, especially for patients with chronic disease (14).
To date, several studies of patient-centered care in the treatment of oncological diseases have been performed. In one study, only 44% of breast cancer patients preferred to select their treatment collaboratively, and 34% preferred to delegate the decision-making responsibility to their physicians (15). Davisons et al. (16) and Rotenbacher et al. (17) described high preferences for a passive role in decision-making in patients with cancer. In contrast, this study demonstrated that the majority of patients preferred a collaborative role (69.6%) to a passive role (12.1%) in the decision-making process for selecting an anesthetic method. Furthermore, 18.3% of patients preferred an active role. Although it is difficult to compare our results with those in previous studies that included cancer patients, these differences in decision-making roles might be influenced by the fact that we surveyed healthy patients, and their choices were not likely to affect their lives.
Over the last decade, preoperative anxiety has been studied as an important issue for patients scheduled for surgery. In non life-threatening procedures, anesthesia (62%) is the main source of preoperative anxiety in patients, rather than surgery (15%) (18). Preoperative anxiety and fear in patients can complicate the management of anesthesia and the postoperative period, which can be attributed mostly to the lack of information about anesthesia (19). A study evaluated patients' satisfaction about a preanesthetic interview by anesthesiology resident, and reported that 39% of patients were very satisfied and 50% of them were satisfied with the interview, even though the duration of the interview was relatively short (20). In the present study, our patients received detailed information about two anesthetic methods, had discussions with an anesthesiologist and were involved in the decision-making regarding the anesthetic method selected. Our patients were very satisfied (58%) and satisfied (35.4%), and felt very respected (70%) and respected (27.7%) after involvement in the decision-making process. Interestingly, a higher percentage of active role patients were very satisfied (78.7%) and felt very respected (76.6%) than collaborate or passive role patients. Furthermore, the patients expressed a change in preference for assuming an active role (49.4%) and a collaborative role (43.6%) in the decision-making process for their future anesthesia needs. These results suggest that an increase of an active role for their future anesthesia needs may mean an increase of very satisfied and felt very respected patients.
Most procedures on extremities can be performed using regional anesthesia with light sedation (21). However, Shevde and Panagopoulos (22) reported that 69% of patients expressed a preference for general anesthesia over regional anesthesia. Another study reported that 49.3% of all respondents expressed a preference for general anesthesia over regional anesthesia (23). Our study showed that 64.3% of patients requiring surgery on an upper extremity expressed a preference for general anesthesia over a brachial plexus block, and 51.3% of patients requiring surgery on a lower extremity preferred general anesthesia over spinal anesthesia. These results regarding general anesthesia preferences might reflect the patients' concern about pain at the puncture site and the fear of needles because many of them showed the fear during a discussion with the anesthesiologist, especially, when choosing between general anesthesia and the brachial plexus block. Moreover, our results underline the fact that there might be a difference in preference for anesthetic methods between healthy patients and anesthesiologists. Thus, to improve patient-centered care, anesthesiologists should understand and be aware of this difference when informing and discussing the options for anesthesia with patients.
In conclusion, almost all patients who were informed of their choices for anesthesia and involved in the decision-making process were satisfied and felt respected; the majority of patients preferred a collaborative role. Furthermore, a greater number of patients expressed a preference for assuming an active role in the decision-making process for future anesthesia needs. This study provides important information for anesthesiologists and other physicians regarding patient-centered care in a department of anesthesiology.


 XML Download
XML Download