

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Endocrine disrupting chemicals (EDCs) are compounds existed in the environment, and mimic or interfere the effects of endogenous hormones such as estrogens, androgens, progestins, and thyroid, hypothalamic, and pituitary hormones (1). EDCs are lipophilic, resistant to metabolism, and able to bioconcentrate up the food chain. Therefore, they are stored in body fat and can be transferred to developing offspring via the placenta or the egg (2).
Bisphenol A (BPA), a monomer of polycarbonate plastics, is one of the highest-volume chemicals in commerce. Polycarbonates are used in numerous consumer products including food and water containers, baby bottles, metal can linings, medical tubing, and dental fillings. Small amounts of BPA can migrate from polymers to food, particularly when heated (3). BPA has been reported to have estrogenic actions including an uterotrophic effect (4), decreased sperm production (5), stimulation of prolactin release (6) and cell proliferation in a breast cancer cell line (7). In animal studies, prenatal and neonatal exposure to BPA has been linked to the early onset of sexual maturation (8). BPA acts as an adipogenic agent. An in vitro study showed that BPA triggers 3T3-L1 cells to differentiate into adipocytes (9); and perinatal and postnatal exposure of mice to BPA has been found to be associated with weight gain (10-13). BPA has also been associated with chronic disease in humans including cardiovascular disease, diabetes, and serum markers of liver disease (14).
Individuals' susceptibility to a wide range of adverse effects induced by exposure to EDCs is increased during the developmental period (embryonic, fetal, early postnatal, and pubertal), depending on the organ system. Developmental exposure to EDCs can lead to lifelong functional deficits and disease (15).
During infancy, bottle-feeding is thought to be an important source of exposure to BPA. In this study, we investigate infant exposure to BPA and the effect of bottle-feeding on serum BPA levels by measuring serum BPA levels in infants.
MATERIALS AND METHODS
Subjects
Healthy infants between the ages of six and 15 months were recruited from the outpatient clinic of the Department of Pediatrics at Korea University Ansan Hospital. We reviewed their birth records retrospectively and included them in this study according to the following criteria: 1) gestational age between 37 and 41 weeks, 2) birth weight between 2,500 and 4,000 g, and 3) no history of hospitalization. The subjects were divided into two groups: breast-fed and bottle-fed. Subjects who had never been bottle-fed were assigned to the breast-fed group (n=30), and those who had recently been bottle-fed for at least three months were assigned to the bottle-fed group (n=30).
Serum BPA level assay
Serum BPA levels were assayed with a competitive ELISA. A significant correlation (r=0.971) was confirmed between the BPA values measured by the high-performance liquid chromatography and the ELISA (16). Blood samples were collected from all subjects and stored at 4℃ (2.5 mL of blood per subject). The samples were centrifuged for 15 min at 4℃ and the sera were collected. The sera were kept at -70℃ until all samples were collected. Before the assay, the samples were filtered via a solid phase extraction method using a SEP-COLUMN (Strata, Phenomenex, Torrance, CA, USA). Serum BPA levels were assayed with a Supersensitive BPA ELISA KIT (Japan EnviroChemicals, Ltd., Osaka, Japan) according to the instructions provided. Briefly, a bottle of antigen-enzyme conjugate powder was reconstituted with buffer solution to prepare an antigen-enzyme conjugate solution. We mixed 0.1 mL of the conjugate solution and 0.1 mL of a BPA standard or sample in each well of an uncoated microplate. Aliquots (0.1 mL) of the mixture were dispensed into each well of a microplate coated with BPA monoclonal antibody and incubated for 60 min at room temperature (18-25℃). After washing, color solution (0.1 mL) was dispensed into each microplate well and then incubated for 30 min at room temperature. The reaction was stopped by the addition of stop solution (0.1 mL). The optical absorbance of the standards and samples was measured at a wavelength of 450 nm using a plate reader, and a standard curve was generated for the analysis. The quantity of BPA in each sample was calculated based on the absorbance reading and interpolation from the standard curve. All measurements were done in duplicate and averages were calculated. The intraclass correlation coefficient was 0.853 (P<0.001).
RESULTS
The clinical characteristics and serum BPA levels of subjects (n=60) are shown in Table 1. BPA was detected in every study sample. The mean age, body weight, birth weight, gestational age, and serum BPA levels of subjects were 9.9±3.2 months, 9.0±1.1 kg, 3.22±0.39 kg, 39.3±1.1 weeks, and 71.1±79.9 pg/mL, respectively.
There were no significant differences in serum BPA levels, age, body weight, birth weight, and gestational age between male (n=31) and female (n=29) infants (Table 2).
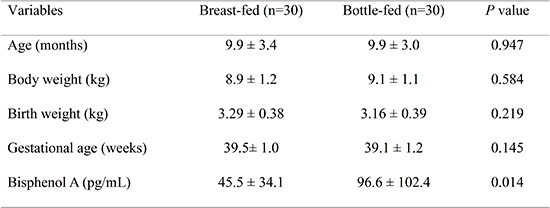
Serum BPA levels were significantly higher in the bottle-fed group (n=30) compared to the breast-fed group (n=30) (96.6±102.4 vs 45.5±34.1 pg/mL, P=0.014). There were no significant differences in age, body weight, birth weight, or gestational age between the breast-fed and bottle-fed infants (Table 3). No significant correlations were found between BPA and age, body weight, birth weight, and gestational age (Table 4).
DISCUSSION
To the best of our knowledge, this study is the first attempt to measure serum BPA levels in infants. In this study, we demonstrated that serum BPA levels were higher in bottle-fed infants than in breast-fed infants.
It was of interest that BPA could be detected in all study samples. An important source of human exposure to BPA is thought to be the ingestion of food and drink that has been in contact with polycarbonate plastic containers (17). Once administered orally, BPA is very rapidly metabolized with a biological half-life of approximately six hours and nearly complete elimination within 24 hr (18). However, because of the continuous and widespread human exposure, BPA has been detected in a variety of human samples at much higher levels than would be expected based on the assumption that BPA is very rapidly metabolized and ingested only infrequently. Over 92% of the 2,517 participants in the US 2003-2004 National Health and Nutrition Examination Survey had detectable concentrations of BPA in their urine (19). In other studies that measured serum BPA levels, BPA was detected in every human sample (20, 21).
Until recently, BPA had been considered to have very weak estrogenic activity in in vitro and in vivo test systems (22, 23). Thus, BPA was previously not believed to pose a threat to human health. However, molecular studies have revealed a variety of pathways through which BPA can stimulate cellular responses at very low doses (24, 25). BPA at environmentally relevant doses is considered to pose risks to human health. The fact that we detected BPA in all infant serum samples suggests that developmental exposure to BPA is almost ubiquitous. Developmental exposure to EDCs is thought to be more harmful to human health than exposure in other periods of life because small changes in the developmental environment can induce phenotypic changes affecting an individual's response to his/her later environment (26).
In this study, serum BPA levels were significantly higher in bottle-fed infants than in breast-fed infants (96.6±102.4 vs 45.5±34.1 pg/mL, P=0.014). It is well-known that BPA can migrate from polymers to food or drinks. High temperature as well as acidic and alkali solutions cause polymer degradation via hydrolysis, resulting in increased BPA migration (27). After a sequence of washing and rinsing, new polycarbonate bottles were found to have leached BPA into the bottle contents after incubation at room temperature for seven days (3). Previous laboratory studies have shown that BPA is released from polycarbonate bottles after simulated normal use (3, 28). In a human study, urinary BPA concentrations increased by 69% after subjects used polycarbonate drinking bottles for one week (29). The results of the present study suggest that baby bottles release a considerable amount of BPA into the baby bottle contents, thereby significantly increasing the amount of BPA in the serum of infants who ingest formula from these bottles. Thus, it is assumed that bottle-feeding increases the risk of developmental exposure to BPA.
It has been reported that serum BPA levels are higher in males than in females and are positively correlated with testosterone levels (20). The gender differences in serum BPA levels are possibly due to differences in the androgen-related metabolism of BPA (20). We found no gender differences in serum BPA levels in this study. In infants, serum androgen levels are quite low, and gender differences can be neglected. Accordingly, it is presumed that the effects of androgen on the metabolism of BPA were too slight to result in gender differences in serum BPA levels in this study.
Children have been found to have higher urinary BPA levels than adolescents and adults (19), consistent with animal evidence of fetuses and infants' reduced ability to clear BPA due to reduced glucuronization (30). Thus, we predicted that age would be negatively correlated with BPA levels. However, in this study, age was not significantly correlated with serum BPA levels. This lack of correlation may be due to the fact that all infants who participated in this study were within the narrow age range of six to 15 months.
We excluded infants who had been hospitalized in order to exclude BPA exposure from medical tubing. However, previous BPA exposure from other sources, including maternal exposure, a weaning diet, drinking water, and the home's surroundings were neither assessed nor controlled for in this study. Another possible limitation of this study is that the sample size was relatively small. Therefore, large-scale and controlled studies are necessary to confirm our findings.
In conclusion, infant exposure to BPA is almost ubiquitous, and bottle-feeding seems to increase the risk of infant exposure to BPA. Establishment of health policies to reduce or prevent BPA exposure in infants is necessary.
 XML Download
XML Download