

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Early diagnosis of rheumatoid arthritis (RA) is crucial because increasing evidence suggests that prompt treatment leads to a better outcome and prognosis (1-3). The results of these studies has recently led to the development of the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) criteria, a new approach to classifying RA and initiating treatment at an earlier stage (4).
Unlike the 1987 ACR criteria, the presence of rheumatoid nodules and typical changes on X-rays, which both reflect long-standing disease, are not included in the new criteria, although serological markers and acute phase reactants are now included. Regarding joint involvement, ambiguous judgment of symmetric distribution and involvement of three or more joints are no longer necessary data points, whereas the number and sites of joint involvement with clinical evidence of synovitis have decisive influence on the diagnosis according to the new criteria (4). However, it is not easy to assess whole body joint swelling and tenderness during a short interview, and the possibility of over- or underestimating the extent of joint involvement always exists since detection during the physical examination depends on patient complaints of joint symptoms. Furthermore, some patients may have already taken anti-inflammatory agents before seeing their rheumatologists, which can make it difficult to observe active arthritis on physical examination. In these circumstances, the diagnosis will require some imaging modality to provide more objective information to complement the clinical assessment.
Bone scintigraphy (BS) that utilizes Tc-99m phosphonate compounds has high sensitivity but low specificity for the detection of bone and joint disease. In other words, using this test, we can easily identify active arthritis in patients, although the results are not specific for RA. For many years, the importance of BS for measuring joint inflammation in RA patients has been emphasized (5, 6). Several previous studies have also confirmed that BS has a high rate of clinical utility in rheumatology (7). Moreover, increased blood pool activity of the involved joints on BS correlated with inflammatory synovitis, which is an early sign of RA (8). Hence, we thought that BS, especially in the blood pool phase, might be useful in suggesting early joint involvement in RA and would be even more meaningful when applied using the new 2010 criteria.
In the current study, we evaluated how BS could supplement the 2010 criteria in the diagnosis of RA during the initial work-up of patients with joint symptoms.
MATERIALS AND METHODS
Participants
Among the 737 patients who first visited the rheumatology department of our university hospital from August 2009 to August 2010 for their joint symptoms, 156 patients who underwent BS and screening laboratory and radiologic tests to confirm RA diagnosis were analyzed retrospectively (Fig. 1). BS had been performed for patients with synovitis to detect subclinical joint involvement or to prove active inflammation in the involved joints, and it was also performed for patients with non-inflammatory joint pain to rule out the possibility of RA (e.g., fibromyalgia).
We divided the patients into two groups according to the presence or absence of arthritis on physical examination by rheumatologists on initial presentation; Group I is the patients with arthritis and group II is the patients without arthritis on initial physical examination. In addition, group I patients were divided into two subgroups based on the 2010 criteria score (≥6 and <6).
Demographic features including the age, sex, and clinical manifestations of RA, including the symptoms, duration, and counts of the involved joints, were evaluated. Inflammation was assessed by determining the levels of C-reactive protein (CRP) and the erythrocyte sedimentation rate (ESR), and auto-antibodies of the rheumatoid factor (RF) as well as anti-citrullinated protein antibody (ACPA) were measured. The normal upper limits of the above tests in our hospital were 0.3 mg/dL, 10 mm/hr for men and 20 mm/hr for women, 15 IU/mL, and 25 U/mL, respectively.
The gold standard diagnosis of RA was defined by the rheumatologists as any RA disease for which a disease-modifying anti-rheumatic drug (DMARD) was prescribed within three months of the first visit.
Imaging protocols and evaluation of the diagnostic validity of bone scintigraphy
BS was performed using intravenous (IV) injection of 740 MBq of technechium-99m hydroxymethylene diphosphonate (99mTc-HDP). Regional images were obtained about five minutes post-injection for the joints of interest, i.e., joints identified by the patients' complaints of pain (the "blood pool" phase). Regional images of the identical fields at the blood pool phase and whole body images were also obtained three to four hours after injection (the "bone" phase). Two highly experienced nuclear medicine physicians interpreted BS in consensus. They were blind to the clinical data and results of the laboratory tests.
Patients with two or more areas of fusiform increased radiotracer uptake on the blood pool phase with or without increased periarticular bone uptake on the bone phase in the predilection site of the joint including hands and/or feet were considered to be diagnostic for RA in "BS only" diagnosis (Fig. 2). In the "BS-assisted" diagnosis, the number and location of joints with abnormal fusiform accumulation of the radiotracer around the joints on the blood pool phase with or without increased periarticular bone uptake on the bone phase were assessed and used as the reference for joint involvement during the diagnosis of RA by a physician on the basis of the 2010 ACR/EULAR criteria.
Statistical analysis
Patient characteristics were presented as the mean with standard deviation (SD). To compare the three sets of conditions, BS only, 2010 criteria, BS-assisted 2010 criteria in the diagnosis of RA, the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and receiver operating characteristic (ROC) curves with corresponding areas under the curve (AUC) were calculated in two groups according to the presence or absence of arthritis on physical examination. The diagnostic validity of the BS-assisted diagnosis was also calculated in the two subgroups divided by the 2010 criteria score (≥6 and <6).
RESULTS
Clinical and demographic features of the participants
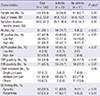
The clinical and demographic characteristics of the study population are shown in Table 1. A total of 156 patients with joint symptoms were included. Seventy-five (48.1%) of the 156 patients had active arthritis (Group I), while the remaining 81 patients did not have arthritis upon physician examination of their first visit (Group II). The sex, age, and symptom duration were not different between them. Among patients in Group I and in Group II, 56 (74.7%) and five (6.2%) had RA, respectively. The positivities for RF, ACPA, CRP, and ESR, as well as the findings of BS, were significantly different between the two groups.
Diagnostic validity of BS only and BS-assisted diagnosis
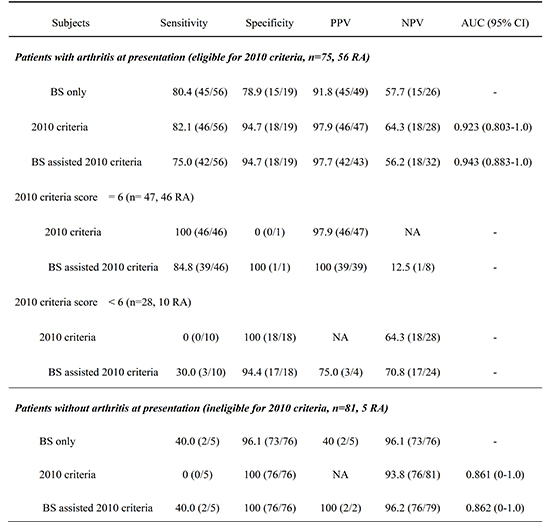
We analyzed the diagnostic validity regarding the diagnosis of RA by group analysis according to the presence of arthritis upon initial presentation. For Group I patients with arthritis (n=75) who were eligible according to the 2010 criteria, the sensitivity (80.4%, 45/56) of the BS only diagnosis was comparably higher than the corresponding statistics of the 2010 criteria assessed by physician only (82.1%, 46/56) with lower specificity (78.9%, 15/19 and 94.7%, 18/19, respectively). The sensitivity of the BS-assisted 2010 criteria (75.0%, 42/56) was slightly lower, and the specificity (94.7%, 18/19) was the same compared to the 2010 criteria assessed by a physician only. The AUC of the ROC curves was comparable or even higher in the BS-assisted diagnosis than in the diagnosis using the 2010 criteria assessed by physician only (0.943 in BS assisted diagnosis vs 0.923 in physician only). The McNemar test found no statistically significant difference between the gold standard and BS only diagnosis (P=0.118), and there were statistically significant differences for the 2010 criteria assessed by physician only (P=0.001) and BS-assisted 2010 criteria (P=0.012). However, in the PPV of the 2010 criteria assessed by physician only, one of the most important factors of the diagnostic test in discriminating true positives from positive test results was the highest, followed by the BS-assisted diagnosis and the BS only diagnosis: 97.9% (46/47), 97.7% (42/43), and 91.8% (45/49), respectively.
We further classified group I patients into two subgroups according to the 2010 criteria score (≥6 and <6) to determine a suitable subject to examine BS. In the subgroup with a 2010 criteria score of 6 or higher (n=47, 46 RA), there was no benefit to the sensitivity of the BS-assisted diagnosis (84.8%, 39/46) than the 2010 criteria assessed by rheumatologists only (100%, 46/46). However, their PPVs were comparable (100%, 39/39 and 97.9%, 46/47, respectively). In the subgroup with arthritis and a 2010 criteria score under 6 (n=28, 10 RA), three more RA patients could be detected by BS-assisted diagnosis. Moreover, the PPV of the BS-assisted diagnosis was sufficiently higher (75.0%, 3/4) to discriminate the RA patients from the non-RA patients in this subgroup.
Group II patients (n=81, 5 RA) without arthritis and who were not eligible according to the 2010 criteria, BS-assisted diagnosis identified two cases of RA, whereas the 2010 criteria assessed by physician only failed to identify any patients with RA. Also, the AUC of the ROC curves showed good results in the discrimination of true RA patients using BS-assisted diagnosis (0.862 in the BS-assisted diagnosis vs 0.861 in physician only). The PPV of the BS-assisted diagnosis was also sufficiently higher (100%, 2/2) to discriminate between the RA patients from the non-RA patients in this group (Table 2). The McNemar test found no statistically significant difference among the gold standard and the BS only diagnosis (P=1.000) as well as the 2010 criteria assessed by physician only (P=0.250) and the BS-assisted 2010 criteria (P=0.063).
DISCUSSION
Our results indicate that the BS only or BS-assisted diagnosis did not show a noticeable increase in sensitivity in the evaluation of patients with arthritis compared to the 2010 criteria assessed by physicians only. However, in patients without arthritis who were not eligible according to the 2010 criteria, BS-assisted diagnosis can help to detect RA with high PPV. The AUC of the ROC curve showed better discrimination of true RA patients in BS-assisted diagnosis than using the 2010 criteria assessed by the physician only in both groups (with or without arthritis at the initial physical examination). Moreover, among patients with arthritis who did not satisfy the 2010 classification criteria (score<6), BS assisted diagnosis identified additional true RA patients with high PPV, which could be valuable support in daily clinical practice. Therefore, BS-assisted diagnosis seems to be helpful in the diagnosis of RA among patients who do not satisfy the 2010 criteria (score<6) as well as suspect patients who are ineligible for the 2010 criteria due to dubitable arthritis at clinical presentation.
To keep pace with the new paradigm for early diagnosis and management of RA, there is also a need for more sensitive imaging modalities that can allow clinicians to carefully track the development of early joint inflammation and damage. Several other modalities have also been studied for the efficacy of evaluating early changes in RA but require further development. Ultrasonography (US) is primarily designed to depict synovial inflammation rather than to directly assess bone destruction (8); it has intra- and interobserver reliability of measures (9) but lacks standardization. Magnetic resonance imaging (MRI) can also be used to detect inflammation outside (synovitis) and inside (osteitis/bone marrow edema) the cortical bone lining, as well as bone edema and erosions (10, 11), but it is expensive and has limited performance regarding all joints of interest.
However, BS has several advantages over the aforementioned modalities, which are high sensitivity, good availability, low cost, and ability to image the entire body (12). The latter seems most important in RA patients where whole body imaging makes it possible to show widespread joint involvement. BS is a highly sensitive technique that has been used in the diagnosis and management of skeletal pathology for nearly 3 decades (13). In contrast, our results of "BS only" diagnosis have relatively low sensitivity. This discrepancy probably occurred because we defined RA not when increased radiotracer uptake was seen on the "blood pool phase" and/or the "bone phase" but only when the uptake was corresponding to the predilection site of the joint involvement of RA. Because 99mTc-HDP binding depends on the osteoblast activity and on the bone remodeling rate, it is not specific for a particular disease process (12). Fisher et al. (14) also argued about the lack of specificity of BS and their minor role in the evaluation of polyarthralgia. In that respect, single photon emission computed tomography/computed tomography (SPECT/CT), a type of the hybrid imaging modalities combining a high-resolution structural image and a functional radionuclide scan image, might improve the specificity through accurate localization of the foci of abnormal uptake and additional structural information (12). However, further studies are required for the exact impact of SPECT/CT compared to planar BS, and SPECT/CT currently has limited accessibility in many facilities. Therefore, our current study using planar BS in the evaluation of RA patients is still significant.
In a real practice setting, however, BS itself cannot be a diagnostic tool for RA because rheumatologists make clinical decisions using a combination of clinical experience, diagnostic criteria, laboratory results, and imaging findings for the gold standard diagnosis of RA. In other words, it is impossible to judge the absolute role of BS alone in the diagnosis of RA. Therefore, we evaluated the diagnostic value of BS as a supplemental tool to the 2010 ACR/EULAR classification criteria ("BS assisted" diagnosis). In this instance, BS was used as an objective indicator of joint involvement during evaluation of the 2010 criteria to replace the subjective measure of physician judgment.
The sensitivity and specificity of the 2010 criteria have been reported to range between 62%-74% and 71.4%-78%, respectively (15-17). The sensitivity values of our 2010 criteria assessed by physician only and by physician with BS assistance were comparable or even slightly higher than those obtained in other studies. Here, our specificity value was much higher than previous studies. The reason for this high specificity was that all the patients were enrolled from our tertiary academic rheumatology department and were assessed by rheumatologic experts. Therefore, the proportion of RA patients as well as non-RA patients with clear-cut clinical manifestations was relatively high, and the patients with undifferentiated arthritis who could be confused with RA was relatively low.
This study has a limitation. We restricted this study to patients who visited our clinic with joint symptoms and for whom laboratory and BS data were available. Therefore, the prevalence for RA might be higher than in the general population. In other words, the diagnostic validity of the 2010 criteria with or without BS assistance might be lower in the general population. However, a benefit is that this type of selection criteria reflects cases encountered in a real practice setting. Therefore, additional investigation is needed to assess which subgroup and clinical setting will allow the 2010 ACR/EULAR classification criteria, assisted by BS, to have better cost-effectiveness and diagnostic performance.
In conclusion, the diagnostic validity of BS-assisted diagnosis of RA on the basis of the 2010 ACR/EULAR classification criteria seems to be comparable to the diagnosis of physicians only for patients with arthritis. Moreover, it can provide valuable information about the number and location of whole body joint involvement, especially for patients who do not satisfy 2010 criteria as well as those who are ineligible for the 2010 criteria due to dubitable arthritis upon initial work-up.


 XML Download
XML Download