

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of obesity has increased rapidly in children and adolescents over the past few decades worldwide (1, 2, 3). There are concerns that childhood obesity-associated complications including metabolic syndrome and non-alcoholic fatty liver disease (NAFLD) might have increased accordingly.
Metabolic syndrome in children and adolescents has been defined to date using various criteria including those by Cook et al. (4), de Ferranti et al. (5), Weiss et al. (6), Cruz et al. (7), Ford et al. (8), the USA National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATPIII) from the National Health and Nutrition Examination Surveys III (9), and the International Diabetes Federation (IDF) in 2007 (10). All of these criteria share the components of abdominal adiposity, hypertension, hypertriglyceridemia or dyslipidemia, and fasting glucose intolerance or diabetes mellitus but have various cutoffs that define the normal and abnormal ranges of each component. As such, the prevalence of metabolic syndrome in children and adolescents may differ upon the use of different criteria and cutoffs (11). To date, most studies on the prevalence of childhood metabolic syndrome were based on general population samples or overweight and obese samples (11).
NAFLD, a hepatic manifestation of the metabolic syndrome related to insulin resistance in obesity, is associated with metabolic syndrome in obese children and adolescents (12, 13, 14). Among the NAFLD spectrum, non-alcoholic steatohepatitis (NASH) usually receives much attention because it can progress to liver cirrhosis, even in children (15). The prevalence of NAFLD has also been evaluated in pediatric studies that mainly focused on the prevalence within the general population or in obese patients (16, 17).
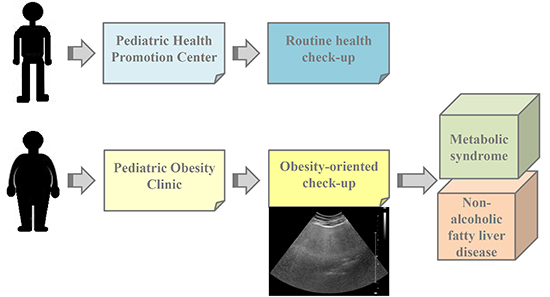
Since obesity-related complications such as metabolic syndrome and the NAFLD spectrum are important health-related issues associated with increased long-term morbidity and mortality, the need for routine check-ups to detect and diagnose these complications has arisen even in children. However, there were no routine health check-up data by health promotion centers or obesity clinics to prevent, diagnose, or treat metabolic syndrome and NAFLD in obese children to date. Such a need resulted in the recent development of pediatric health promotion centers and pediatric obesity clinics, and these 2 pediatric units have been operating independently within our tertiary medical center since 2006.
Therefore, the aim of this study was to evaluate the efficacy of health check-ups in children to detect metabolic syndrome and NAFLD as complications of childhood obesity, comparing the pediatric health promotion center that provides routine health check-ups with that in the pediatric obesity clinic that provides obesity-oriented check-ups, and also to evaluate better diagnostic criteria for metabolic syndrome and better diagnostic modality for NAFLD in children.
MATERIALS AND METHODS
Subjects
A total of 396 children and adolescents who visited 2 different units of the Seoul National University Bundang Hospital, a community-based tertiary medical center, between March 2006 and February 2012, were included: a pediatric health promotion center (n=218) and a pediatric obesity clinic (n=178). The subjects were also divided into three groups according to obesity status: normal weight, overweight, and obesity. Children with underlying organic disease or drug history within the prior 3 months were excluded from the study.
Anthropometric data collection
Body weight was measured to the nearest 0.1 kg and height was measured to the nearest 0.1 cm. Body mass index (BMI) was calculated as body weight (kg) divided by the height squared (m2). BMI percentile was determined according to Korean national growth charts (18, 19). Obesity was defined as a BMI>the 95th percentile for the child's age and gender, while overweight was defined as BMI in the 85th-95th percentiles. Normal body weight was defined as a BMI<the 85th percentile for each child's age and gender.
Abdominal circumference (AC) was measured using a tapeline at the child's maximum waist girth in a standing position. Abdominal obesity was defined as AC>the 90th percentile for the child's age and gender.
Blood pressure (BP) was measured at least twice in a resting state by the same examiner, following international recommendation (20). Hypertension was defined as repeatedly measured blood pressures>the 90th percentile for the child's age and gender.
Laboratory tests
Serum levels of triglycerides (TG), total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, γ-glutamyl transpeptidase (γGT), fasting glucose, and insulin levels were measured after at least a 12-hr fasting period at the first visit. Insulin resistance was determined by the homeostatic model assessment of insulin resistance (HOMA-IR: [insulin×glucose]/22.5).
Diagnostic criteria of metabolic syndrome
The definition of metabolic syndrome in children and adolescents in this study was based on the NCEP-ATPIII and IDF criteria (9, 10). According to the NCEP-ATPIII criteria, metabolic syndrome was diagnosed when the child met >3 of the following 5 characteristics: 1) AC exceeding the 90th percentile for the child's age and gender; 2) serum TG ≥110 mg/dL; 3) HDL cholesterol <40 mg/dL; 4) systolic BP or diastolic BP exceeding the 90th percentile for the child's age and gender; and 5) fasting blood glucose ≥110 mg/dL or presence of diabetes mellitus (9).
According to the IDF criteria, metabolic syndrome was defined as the presence of abdominal obesity (increased AC exceeding the 90th percentile for the child's age and gender in children <16 yr of age and AC >90 cm in boys and 80 cm in girls >16 yr of age) and more than 2 of the following 4 characteristics: 1) serum TG ≥150 mg/dL in all ages; 2) HDL cholesterol <40 mg/dL in most children and HDL cholesterol <50 mg/dL in girls >16 yr; 3) systolic BP ≥130 mmHg or diastolic BP ≥85 mmHg; and 4) fasting blood glucose ≥100 mg/dL or presence of diabetes mellitus (10).
Diagnosis of NAFLD and radiological evaluation of fatty liver
Diagnosis of NAFLD was based on serum aminotransferase levels or abdominal USG findings in each patient. NASH was diagnosed when serum aminotransferase levels were abnormally elevated and fatty liver was detected on USG in the same patient. Patients with other causes of liver diseases were excluded from the study.
Serum levels of aspartate aminotransferase and alanine aminotransferase (ALT) were measured using TBA-200FR NEO (Toshiba Medical Systems Corporation, Tokyo, Japan), and levels exceeding 40 IU/L were considered abnormal.
The presence and the severity of fatty liver were evaluated in all subjects using abdominal USG. The degree of fatty liver on abdominal USG was defined as mild, moderate, or severe (21).
Statistical analysis
The results are expressed as mean±standard deviation (SD). The data were analyzed using the SPSS 18.0 software program (SPSS Inc., Chicago, IL, USA). Frequency data were compared using the chi-square test. Student's t-test was used to compare the means of continuous data in the 2 groups. P values<0.05 were considered statistically significant.
RESULTS
Patient characteristics
A total of 396 children and adolescents (259 boys, 137 girls; 5-19 yr of age; mean±SD=13.9±2.8 yr) visited the pediatric health promotion center (n=218) and the pediatric obesity clinic (n=178) for health check-ups.
The subjects' clinical features and laboratory findings are listed in Table 1. Other than serum γGT level, all clinical and laboratory parameters of obesity, metabolic syndrome, and NAFLD showed statistically significant differences between those who visited the pediatric health promotion center and those who visited the pediatric obesity clinic (Table 1).
Comparison of metabolic syndrome criteria between the 2 units
Significant differences were observed in the prevalence of each component of metabolic syndrome between patients visiting the pediatric health promotion center and those visiting the pediatric obesity clinic comparing the NCEP-ATPIII and IDF criteria as listed in Table 2. The prevalence of definite metabolic syndrome was 3.7% in the patients who visited the pediatric health promotion center and 33.1% in those who visited the pediatric obesity clinic according to NECP-ATPIII criteria, and 3.2% and 23%, respectively, according to IDF criteria (Table 2).
The prevalence of NASH was 4.1% among patients who visited the pediatric health promotion center. The prevalence was 56.2% in those who visited the pediatric obesity clinic according to the presence of fatty liver on USG and abnormal serum ALT levels (Table 2).
Prevalence of metabolic syndrome and NAFLD according to obesity status
When we reevaluated the prevalence of metabolic syndrome and each risk factor according to obesity status, significant differences were observed in the prevalence of each criterion of metabolic syndrome by the NCEP-ATPIII and IDF criteria and the prevalence of NAFLD among children and adolescents who were of normal weight, overweight, and obese (Table 3). The prevalence of abdominal obesity, hypertension, hypertriglyceridemia, and fasting glucose intolerance or diabetes mellitus was significantly different among the 3 body weight groups according to NCEP-ATPIII and IDF criteria (Table 3). The prevalence of definite metabolic syndrome was significantly different among the 3 groups according to the 2 criteria sets with a lower detection rate of metabolic syndrome in overweight or obese children and adolescents by the IDF criteria than that by the NCEP-ATPIII criteria (Table 3).
The detection rate of fatty liver on USG was significantly different among the 3 body weight groups (P<0.001) (Table 3). The prevalence of abnormally elevated serum ALT levels was also different among the 3 groups (P<0.001) (Table 3). The prevalence of NASH based on both USG findings and serum ALT levels was 1.6% in normal-weight children, 36% in overweight children, and 59.4% in obese children and adolescents (P<0.001) (Table 3).
DISCUSSION
According to recent data, the prevalence of overweight and obesity
and trends in BMI in childhood have increased remarkably compared with the past data in Korea and other countries (1,2,3,22). Consequently, a significant increase in the prevalence of obesity-related complications including metabolic syndrome has been reported worldwide, even in children and adolescents, not only in the general population but also in the obese population (11). These trends suggest that childhood obesity and its complications have become one of main public health problems, and early detection and the prevention of obesity-related disorders are required to promote health even in childhood.
In the present study, we compared the prevalence of metabolic syndrome using anthropometric measurements and biochemical tests between patients visiting the pediatric health promotion center for a routine health check-up regardless of obesity status and overweight or obese children visiting the pediatric obesity clinic for a check-up. As a result, the detection rate of definite metabolic syndrome was 3.7% among patients visiting the pediatric health promotion center and 33.1% among those visiting the pediatric obesity clinic according to the NECP-ATPIII criteria and 3.2% and 23%, respectively, by the IDF criteria in our study. Previous reports have shown that the prevalence of metabolic syndrome in the general population varied according to definitions and population as follows: 2.0%-21% in children and adolescents in North America, 9.3%-22.6% in Latin America, 3.7%-14.1% in Asia-Australasia, and 1.4-21% in Europe (11, 23, 24). On the other hand, the prevalence of metabolic syndrome in the overweight or obese population was 22%-39% in children and adolescents in North America, 17.4%-36.1% in Latin America, 10.3%-41.8% in Asia, and 10.9%-31.9% in Europe (11, 25, 26). These data in the general population were similar to the detection rate of metabolic syndrome in our pediatric health promotion center, and the data on obese children and adolescents were similar to that of the pediatric obesity clinic in our medical center, indicating that these 2 units may represent the general and obese populations of Korean children and adolescents, respectively. This is why we reevaluated the prevalence of metabolic syndrome and each risk factor according to obesity status, which revealed a metabolic syndrome prevalence of 1.1% in normal-weight children, 10.7%-20% in overweight children, and 28.6%-37.6% in obese children and adolescents, and it dramatically increased according to obesity status.
Regarding each component of metabolic syndrome, significant differences were also noted between the 2 units by the 2 different criteria in our study. In addition, when the prevalence of each component was reevaluated according to obesity status, the prevalence of abdominal obesity, hypertension, hypertriglyceridemia, and fasting glucose intolerance, but not HDL cholesterol, was significantly different among the 3 groups in our study.
In the present study, we used 2 relatively new but different criteria for metabolic syndrome: the NCEP-ATPIII and IDF criteria. The detection rate of metabolic syndrome by the IDF criteria was lower in overweight or obese children and adolescents than that of the NCEP-ATPIII criteria, and the IDF criteria failed to diagnose metabolic syndrome in some children, mainly due to the higher cutoff point for hypertriglyceridemia (9, 10, 27). Moreover, the IDF criteria were more difficult to apply because of different cutoff and standard values for abdominal obesity, hypertension, and HDL cholesterol in various age groups (10). Thus, the NCEP-ATPIII criteria were more applicable in health check-ups in pediatric populations, especially overweight and obese children and adolescents. However, the IDF criteria may still have priority over the NCEP-ATPIII criteria in terms of glucose intolerance due to the higher detection rate using a lower cutoff value.
With regard to the epidemiology of NAFLD, a recent study reported that its prevalence might be 3%-10% in the pediatric population and up to 40%-70% in obese children and adolescents and that it is continuously increasing (28, 29). In our study, the prevalence of NAFLD was 8.7% among patients visiting the pediatric health promotion center and 71.9% among those visiting the pediatric obesity clinic, on the basis of USG findings, and 5.9% and 61.8%, respectively, on the basis of liver enzymes, whereas the prevalence of NASH according to fatty liver on USG and elevated liver enzymes was 4.1% and 56.2%, respectively. Considering obesity status regardless of unit, the prevalence of NAFLD and NASH was 3.7%-4.8% and 1.6%, respectively, in normal-weight children, 40%-50.7% and 36% in overweight children, and 64.7%-75.2% and 59.4% in obese children and adolescents, respectively, according to screening modality. These results were similar to previous data on the prevalence of NAFLD in the pediatric population that reported a prevalence of 3%-3.2% by liver enzymes and 9.6% by USG, and a prevalence in overweight and obese children of 10%-80% by liver enzymes and 15%-44% by USG (15). Moreover, our data suggest that the detection rate of NAFLD by USG was higher than that of liver enzymes; thus, the application of USG as a screening tool with a purpose of a health check-up may be recommendable in overweight or obese children and adolescents who visit the health promotion center or obesity clinic despite higher cost because measuring liver enzymes alone could lead to overlooking the diagnosis of NAFLD (28). Therefore, this approach should be BMI-oriented and based on patient obesity status considering cost-effectiveness.
The present study has some limitations. First, there may be a sort of selection bias because our study merely included the patients who visited a tertiary medical center even though it is community-based. Second, the detection of NAFLD is based on USG and liver enzymes in our study just as other epidemiologic studies, although the gold standard of diagnosis is liver biopsy. Further research evaluating the effect of obesity-oriented approach in pediatric population and the development of preventive and therapeutic strategies for obese children based on this approach is required.
In conclusion, the prevalence of metabolic syndrome and NAFLD was higher among the patients visiting the pediatric obesity clinic that targeted overweight and obese children than that among the patients visiting the pediatric promotion center that offered routine health check-ups for healthy children. That means that obesity-oriented check-ups in overweight and obese children more effectively detect metabolic syndrome and NAFLD than routine check-ups in healthy children without any clinical indications. As such, the introduction of obesity-oriented approach and the application of proper diagnostic criteria and modalities is necessary in terms of health prevention in overweight or obese children and adolescents.



 XML Download
XML Download