

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Critically ill patients, including those in medical intensive care unit (MICU), are at increased risk for venous thromboembolism (VTE) such as deep vein thrombosis and pulmonary embolism (1). Many patients have multiple thrombosis risk factors such as advanced age, sepsis, heart failure, mechanical ventilation, paralysis and central venous catheters (2).
The true incidence of VTE in critically ill patients is unknown but is estimated to range from 5% to 80% (3, 4). Previous studies have shown regional variations in the incidence of VTE, and thus far, most population-based data on VTE epidemiology were predominantly from Caucasian populations (5, 6, 7). Incidence of VTE has been rarely reported in Asian populations (8, 9, 10) and more so in critically ill Korean patients. Also, a significant portion of VTE is left undetected in MICU (6, 11) and it contributes significantly to morbidity and mortality associated with critical conditions (3). Given these factors, the core of VTE management is prevention.
Preventative measures largely fall into two groups: pharmacologic prophylaxis, such as low molecular weight heparins (LMWH) and unfractionated heparins (UFH) and mechanical prophylaxis, such as graduated compression stockings (GCS) and intermittent pneumatic compression (IPC). Diverse modes of VTE prophylaxis have been reported to be used in 33% to 100% of the critically ill patients (12). However, the actual range and frequency of VTE prophylaxis administered to MICU patients are not well defined. Especially, VTE prophylaxis is predicted to be under-utilized in Asia because of the misconception that its incidence is lower in Asians compared to Caucasians (13). The objective of this multicenter observational study was to assess the actual use of VTE prophylaxis in Korean critically ill MICU patients.
MATERIALS AND METHODS
Study design
Consecutive medical patients over 40 yr of age and expected MICU stay of more than 48 hr were eligible for this observational cohort study. Patients from MICUs of 23 hospitals in Korea were enrolled between June 2009 and July 2011. Patients already on anticoagulation therapy before admission to MICU or those requiring anticoagulation for other reasons not related to VTE were excluded. Additional exclusion criteria were contraindication to mechanical prophylaxis, recent operation, plans for operation within a week, absence of written consent or current participation in other clinical trials.
Data collection
Patient data was collected at enrollment and at day 7 or day discharged from the MICU if the patient was discharged before day 7. For each patient, we recorded age, sex, height, weight, admitting diagnosis, VTE risk factors (14), bleeding risk factors and VTE prophylaxis. Thrombocytopenia was defined as platelet counts below 100,000/µL and renal insufficiency was defined as creatinine clearance below 30 mL/min. All diagnostic tests for VTE performed during the study period were recorded.
Statistical analyses
All data analysis was conducted using the Statistical Package for the Social Sciences (SPSS) version 19.0. The chi-square test was used to compare non-continuous parameters and the Mann-Whitney rank-sum test was used to compare continuous data. Probability of <0.05 was considered significant.
Ethics statement
The study protocol was reviewed and approved by the institutional review board (IRB) of each hospital (Seoul National University College of Medicine, IRB No.0906-080-284; Asan Medical Center, IRB No.2009-0203; Hallym University Sacred Heart Hospital, IRB No.2009-S017; Yonsei University College of Medicine, IRB No.4-2009-0149; Wonkwang University College of Medicine, IRB No.7303-355; Chonnam University College of Medicine, IRB No.E-2009-05-045; Seoul Paik Hospital, IRB No.SIT-2009-082; Pusan Paik Hospital, IRB No.09-058; Sanggye Paik Hospital, IRB No.09-41; Konkuk University School of Medicine, IRB No.KUH1010151; Nowon Eulji Hospital, IRB No.EMCIRB 09-30; Ajou University School of Medicine, IRB No.AJIRB-MED-OBS-09-111; Eijeongbu St. Mary's Hospital, IRB No.UC09OSME0063; Dongguk University Ilsan Hospital, IRB No.2009-1-29; Daejeon Eulji Hospital, IRB No.09-30; Wonju Christian Hospital, IRB No. CR309010; Pusan National University Hospital, IRB No.2009069; Ulsan University Hospital, IRB No.09-37; Seoul Paik Hospital, IRB No.SIT-2009-082; Seoul St. Mary's Hospital, IRB No.KC09OSME0193; Chonnam National University Hwasun Hospital, IRB No.HCRE 0940-4; Soonchunhyang University School of Medicine, IRB No.2009-51; Inha University College of Medicine, IRB No.2009-862; Kangdong Sacred Heart Hospital, IRB No.09-46; Yeouido St. Mary's Hospital, IRB No.SC09OSMI0075). Informed consent was waived by the IRB.
RESULTS
Patient characteristics
Of the 844 patients enrolled in the study, 14 enrolled patients were excluded from the final analysis for the following reasons: 10 because the patient needed anticoagulation therapy from reasons other than VTE such as atrial fibrillation, acute coronary syndrome or renal replacement therapy, 2 because the patient underwent emergent surgery within 7 days of enrollment and 2 because informed consent was waived (Fig. 1).
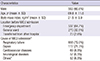
Baseline characteristics of the 830 patients are shown in Table 1. Patients were admitted to MICU for various reasons but the most common diagnosis on admission was respiratory failure (79%). Table 2 summarizes the risk factors for VTE and bleeding. Almost all patients (90%) had more than one risk factor for VTE before admission to MICU and 697 (84%) patients acquired new risk factors for VTE during their MICU stay. Patients had median of 4 risk factors for VTE (range, 0-8). The most common VTE risk factor was old age (age 65 yr and over) (71.2%) followed by presence of central venous catheters (63%). Bleeding risk factors were assessed before and after MICU admission and 374 patients (45%) had more than one risk factor for bleeding. The most common risk factor was thrombocytopenia (20.8%) followed by coagulopathy (18.9%).
VTE thromboprophylaxis
Among 830 MICU patients, 560 (67.5%) of the patients received VTE prophylaxis. Patients who received prophylaxis was significantly older (P<0.001), had heart or respiratory failure (P=0.009) and sepsis (P<0.001) compared with those not on VTE prophylaxis. Previous history of VTE, presence of malignancy, immobilization and estrogen use was not different between the two groups. Patients with recent bleeding were more likely to not receive any prophylaxis (P<0.001). However, presence of other bleeding risk factors such as history of hemorrhagic stroke, coagulopathy, thrombocytopenia and renal insufficiency did not differ between patients who received prophylaxis and those who did not receive any prophylactic treatment for VTE.
Pharmacologic prophylaxis was administered to 323 (38.9%) patients. LMWH were prescribed to a total of 239 patients and 104 patients received unfractionated heparin. In the LMWH group, only one patient was given dalteparin and all the other patients received enoxaparin. Most of the patients (207 patients, 64.1%) were started on pharmacologic VTE prophylaxis on the first day of MICU admission. Sixty patients (18.6%) started pharmacologic prophylaxis on the second day followed by 22 patients (6.8%) on the third day, 15 patients (4.6%) on the fourth day, 8 patients on the fifth day, 5 patients on the sixth day and 6 patients on the seventh day of MICU admission.
Mechanical prophylaxis was administered to 318 (38.3%) patients. Either GCS (n=165), IPC (n=169), or both (n=16) was used. Most of the patients (231 patients, 72.6%) were started on mechanical VTE prophylaxis on the first day of MICU admission and 44 patients (13.8%) started on the second day. One hundred twenty-six patients (39.6%) had bleeding risk factors.
Eighty-one patients (9.8%) received both pharmacologic and mechanical prophylaxis. These patients were more likely to be diagnosed with sepsis (25.9% vs. 13.8%) and treated with mechanical ventilation (92.6% vs. 49.1%), sedatives (81.5% vs. 36.4%) and central venous catheters (76.5% vs. 54.3%) compared with patients who did not receive any prophylaxis (P<0.001).
Diagnosis of symptomatic VTE
During ICU stay, 17 patients underwent diagnostic tests for suspected VTE and the results were positive in 8 patients (0.9%). For diagnostic tests, 15 patients underwent chest computed tomographic angiography, one patient had Doppler ultrasound of the lower extremities and one patient had venography. Among the 15 patients with chest computed tomography, 5 were diagnosed with pulmonary embolism. Deep vein thrombosis was diagnosed in one patient who underwent venography. Left ventricular thrombus and iliac vein thrombus was accidentally discovered in two patients.
Among 8 patients with confirmed VTE, 4 patients were male and 4 patients were female. All but one patient had risk factors for VTE before and after ICU admission. Three patients had risk factors for bleeding, one with coagulopathy and two patients with both coagulopathy and renal insufficiency. All of the patients were on VTE prophylaxis. Three patients were on both pharmacologic and mechanical prophylaxis, whereas 1 patient was on mechanical prophylaxis only and 4 patients were on chemical prophylaxis only.
Clinical outcomes
At day 7, 55 patients (6.6%) had died, 548 patients (66%) were still in the MICU and 227 patients (27.3%) were discharged from ICU. Among the non-survivors, 16 patients (29.1%) did not receive any prophylaxis for VTE. The cause of death in all 55 patients was associated with the underlying disease and not VTE.
DISCUSSION
Critically ill patients face an increased risk of VTE and VTE occurrence is known to be associated with significant morbidity and mortality (15). According to the current guidelines, routine prophylaxis of VTE with LMWH or UFH is recommended to critically ill patients admitted to ICU and mechanical thromboprophylaxis is recommended for those who are bleeding or are at high risk for major bleeding (16). However, despite compelling evidence suggesting routine thromboprophylaxis for critically ill patients, prophylaxis rates as low as 33% have been reported in previous studies (12, 17). Unfortunately, thromboprophylaxis rates of critically ill Asian patients are not well studied compared to the Western population. Parikh et al. (18) studied the current VTE prophylaxis methods in Asian patients admitted to MICU, but the study only included patients in whom decision to give VTE prophylaxis had already been taken. Therefore, actual use of thromboprophylaxis in real practice settings could not be assessed.
The results of this prospective observational study of 830 MCU patients show that routine thromboprophylaxis in Korean critically ill medical patients are still significantly underused. Only 67.5% of the patients received any form of thromboprophylaxis. Although 45% of our study population had risk factors for bleeding and 3% of the patients had more than one bleeding risk factors, according to the 9th American College of Chest Physicians Consensus Conference on Antithrombotic Therapy guidelines (16), mechanical prophylaxis measures should have been considered.
Relatively low rate of thromboprophylaxis may be associated with the previous belief that the incidence of VTE is low in Asian population. However, yearly increasing incidence of VTE has been reported in the Korean population (19). The current Korean guidelines (20, 21) recommend immediate stratification of thrombotic risk and emphasizes on the primary prevention of VTE. The guidelines also specify that since the majority of patients admitted to the ICU have multiple risk factors for VTE, pharmacological or mechanical prophylaxis should be given. Also, underestimation of the risk of VTE and fear of bleeding complications have been discussed as a possible explanation for underutilization of prophylactic therapy (22).
Since the main purpose of this study was not to assess VTE prevalence, diagnostic tests were performed only when VTE was clinically suspected. Diagnosis of VTE in critically ill patients are challenging because many patients are on sedatives and mechanical ventilation and therefore they are not able to communicate their symptoms. Also diagnostic modalities to diagnose VTE are limited in these subjects. Potential risk of transfer and risks of development of contrast-induced nephrotoxicity cannot be dismissed in many cases. Illustrating this, only 17 patients (2%) in our study underwent diagnostic tests for VTE. Interestingly, all of the patients diagnosed with VTE in this study were under thromboprophylaxis. Development of VTE is known to be high despite thromboprophylaxis. Ibrahim et al. (23) reported that 23.6% of the ventilated MICU patients developed VTE even after 100% employment of prophylaxis.
The study has certain limitations. First, factors influencing the physician's decision making, regarding thromboprophylaxis methods, were not assessed. Overestimations of bleeding, negligence and lack of consensus guidelines have been suggested as a possible explanation for underutilization of VTE prophylaxis (24). Second, patients were followed up only until 7 days after MICU admission and thus long-term outcomes could not be assessed. Third, although it might be associated with underutilization of thromboprophylaxis, complications related to thromboprophylaxis, such as bleeding events were not recorded.
However, to the best of our knowledge, this is one of the few multicenter studies to report the actual use of VTE prophylaxis in critically ill Asian patients. Also most of the studies are conducted in mixed ICU or surgical ICU and studies targeting only patients in MICU are rare. Hopefully, the results of this study will shed some light on the issue of adequate and effective prevention of VTE in MICU.
Our data show that 90% of Korean patients admitted to MICU are at risk for VTE and that the recommended VTE prophylaxis is underutilized, since only 67.5% of eligible patients received either chemical or mechanical prophylaxis. Further studies are needed to clarify the role and efficacy of VTE prophylaxis in Korean critically ill patients.


 XML Download
XML Download