

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Poisoning is the third leading cause of injury-related mortality in Korea, with more than 3,000 deaths due to toxic exposures being reported annually between 2005 and 2010 (1). More than 90% of these poisoning-related deaths were due to suicide attempts with insecticides (1). In the United States (US), poisoning is the second leading cause of injury-related morbidity and mortality and its incidence is rising (2). The National Poison Data System of the American Association of Poison Control Centers receives reports of more than 2.4 million human poison exposures and approximately 1,300 poisoning-related deaths annually (3). However, actual poisoning-related mortality would be much higher because it is known that only about 5% of US poisoning-associated mortality was reported to the poison control centers (2).
Emergency antidotes are administered in ED, generally in consultation with a poison information centre or toxicologist, shortly after patient presentation and without the benefit of sophisticated toxicology testing. The stocking of emergency antidotes at emergency departments (EDs) or hospital pharmacies can reduce the medical resources that would be needed to treat poisoning patients. It also shortens the period of therapy and in some cases save the patient from death, even in cases where the patient is already receiving optimal supportive care. This would ultimately reduce the burden on the social resources that is imposed by cases of poisoning (4). Many countries recognize that a nationwide antidote stocking and delivery system is an essential safety system that is maintained by cooperating governmental agencies, pharmaceutical agents, and national poison control centers (5, 6, 7, 8, 9). In 2009, the second US national consensus guidelines regarding antidote stocking were published. These guidelines indicate to hospitals which antidotes should be stocked and its quantities are recommended (5). Many countries also have their own antidote stocking guidelines (6, 7, 8, 9). However, in Korea, comprehensive guidelines regarding the antidotes are lacking.
This study was conducted to develop a list of emergency antidotes and estimate the quantities of these antidotes for the initial treatment of acute poisoning patients at EDs in Korea.
MATERIALS AND METHODS
This study consisted of three phases (Fig. 1). First, a panel of clinical toxicologists was established to make a recommendation list of emergency antidotes. Second, a multicenter epidemiological study was performed to identify the nationwide emergency antidote usage for acute intoxicated patients. Finally, the quantities of emergency antidotes were estimated on the basis of data recorded at the national emergency department information system (NEDIS) in Korea.
List of emergency antidotes
The panel of clinical toxicologists was made that comprised the research society for emergency antidotes stock and delivery system in Korea consisted of a diverse group of 13 professionals who represented various perspectives (Table 1). The principal investigator, who served as the chairperson, selected these experts on the basis of their clinical toxicology researches and professional experiences. The experts were first assigned particular antidotes to generate evidence-based summaries of the medical literature. They measured the usefulness of emergency antidotes for Korean poisoning patients. Each antidote was classified on the basis of its efficacy and the urgency with which it must be available when a case of acute poisoning presents at ED. The efficacy of a particular antidote was graded on the basis of its strength of evidence into one of three classes from class I, the strongest to class III, the weakest evidence. In terms of the urgency of availability, the antidotes were classified into three levels (A to C) on the basis of a WHO classification system (Table 2) (10). These panel members participated three times of Delphi survey for consensus of antidote classification among experts between August and October, 2009. Subsequently, a primary reviewer was allocated to each antidote. Each primary reviewer independently reviewed and revised the original antidote summary and created a standard summary to reassess each antidote. The primary reviewer could add articles to the original summary and provided a provisional antidote classification. The revised literature summary and the recommended classification were then presented to the entire panel. The panel deliberated in October, 2009. An iterative process was used to reach consensus regarding the efficacy and urgency of availability each antidote. Thus, after presentation of an antidote by the primary reviewer and discussion by the entire panel, a vote was taken to determine consensus. An antidote was recommended to be stocked if the panel consensus was affirmative for all questions. A consensus was defined as the full agreement of the eligible panel members. Each member could vote in one of three ways: agreement, disagreement, or strong disagreement. If one or more panel members expressed strong disagreement, the discussion was continued and final consensus was reached through the panel discussion.
Multicenter survey of antidote utilization
In the absence of a Korean epidemiological data about nationwide acute poisoning, estimates of antidote utilization frequency were based primarily on a multicenter epidemiological study. We performed a multicenter epidemiological study to find the antidote utilization for acute intoxication patients in EDs between June, 2010 and May, 2011. A clinical toxicologist in each hospital was responsible for the data collection at each ED. To identify cases of acute poisoning, 228 ICD-10 codes that define acute intoxication or poisoning were used. Inclusion criteria of the patient was over 16 yr of age, had been admitted to the ED during the study period, the diagnosis was acute poisoning. The following cases were excluded: adverse reactions and secondary drug effects; chronic poisoning; insect bites; and inert foreign body ingestions. A specific report form was designed to record the following data: personal data (age and sex); time and day of poisoning; type of intoxication (suicide, intentional, illicit drug abuse, and other); type of toxic compound(s); type of medical assistance before admittance to the ED; severity of symptoms on admittance; treatment; and patient's outcome and condition on discharge. Clinical severity was measured by using the Poisoning Severity Score, which allows the simple stratification of patients on the basis of the clinical effects of poisoning (11). This score grades severity as follows: none (score 0), no symptoms or signs related to poisoning; minor (score 1), mild, transient, and spontaneously resolving symptoms; moderate (score 2), pronounced or prolonged symptoms; severe (score 3), severe or life-threatening symptoms; and fatal (score 4), causing death. The needed case of emergency antidotes were defined the patients who showed moderate-to-severe symptoms after acute poisoning at ED.
Estimation of emergency antidotes stocking amount
The quantities of antidotes that should be stocked at the EDs in Korea were estimated on the basis of the number of poisoned patients whose data were entered into NEDIS. It was assumed that the poisoned patients identified in the nationwide multicenter epidemiological study were an appropriate sample of the population. NEDIS is a nationwide information and standardization system that records emergency treatment data from EDs in Korea. The NEDIS gathered the clinical data of emergency patients at the most of moderate-to-large sized hospitals in Korea. The data of these patients are collected from the EDs via the web and entered into the central server of the national emergency medical center. The minimum quantities of the emergency antidotes that would meet the immediate needs of acute intoxication patients and that should be stocked at ED were calculated on the basis of frequency of use, as indicated by the epidemiological study. The minimum stocking amounts was estimated on the basis of the initial antidote amount that is needed for the dose of treating an adult patient.
Statistical analyses
The chi-square test was used to compare proportions. Standard descriptive statistics were reported as means and standard deviations. Means were compared by using the 2-tailed Student's t-test and the Mann-Whitney U-test. All calculations were performed by using the statistical software package SPSS 20.0 (Statistical Package for the Social Sciences, Chicago, IL, USA). Differences were considered to be statistically significant if the P value was less than 0.05.
RESULTS
List of 18 emergency antidotes
The panel summarized the effectiveness of each antidote in clinical practice and its urgency of availability with the reviews of many articles and provisional recommendations (12, 13). Antidote effectiveness in practice was classified according to the solidity of the evidence showing effectiveness (Table 2). Thus, Class I evidence of effectiveness means that the effectiveness of the antidote is well documented; typically, it is clear that the antidote reduces the lethality of the poison. Class II evidence means that while the antidote is widely used, its effectiveness is not yet universally accepted because of a lack of research data. Class III evidence means its efficacy is questionable. The antidotes were also classified according to urgency of availability: the Class A antidotes should be immediately available (within 30 min); the Class B antidotes are required within 2 hr; and the Class C antidotes are required within 6 hr (Table 2). Using this classification system, the panel made recommendations regarding 36 antidotes could be effective at hospitals in Korea (Table 3).
The emergency antidotes that should be available immediately were determined by the consensus for the statue of recommendation. There were sixteen IA antidotes, namely, antidotes with well-documented effectiveness that are needed immediately. These were fomepizole (methylpyrazole), N-acetylcysteine, amyl nitrite, atropine, beta-blockers, calcium gluconate gel, digoxin-specific Fab antibody fragments, ethanol, folinic acid, glucagon, glucose (hypertonic), hydroxocobalamin, pralidoxime, sodium bicarbonate, sodium nitrite, and sodium thiosulfate. Four of the IA antidotes are used either in combination as a kit system (amyl nitrite, sodium nitrite, and sodium thiosulfate) or alone (hydroxocobalamin) to treat cyanide intoxication. Therefore, these three antidotes in a kit were considered as one antidote. There were four IIA antidotes, namely, antidotes that are immediately required but whose research data are insufficient or involve controversies regarding the universal usage of the drug. These were activated charcoal, diazepam, flumazenil, and neostigmine. Thus, the panel generated a list of 18 emergency antidotes that should be available immediately and should be stocked at EDs in Korea (Table 4).
Multicenter study data analysis
The eleven EDs participated which were belonged to regional emergency medical centers or university hospitals in different regions of Korea (Fig. 2). There were three hospitals in Seoul and the Gyeonggi region, two in Gangwon, two in Daejeon and Chungcheong, two in Gyeongsang, one in Jeolla, and one in Jeju. Totally 4,870 cases were identified and these cases represented 0.6%-1.3% of the each hospital admitting patients at the 11 EDs during the study period. The mean age was 42 yr (range 16-95, standard deviation±21) and the most prevalent age was the forties (18.0%). Females accounted for 57.5% of the cases. Multiple toxic substances were involved in 21.9%. Regarding the type of intoxication, 66.8% were intentional self-intoxications, 28.4% were unintentional cases, 1.0% was suspected to be due to adverse drug events, and 3.8% were unknown.
Compared to the unintentionally poisoned patients, the intentionally poisoned patients were more likely to be older (45 vs. 37 yr, P=0.01) and female (58.7% vs. 54.5%, P=0.01). Many (58.9%) of the patients were poisoned at home and 28.0% were directly transported to the ED by the national 119 rescue services. The intentionally poisoned patients were transported to the ED more frequently by the national 119 rescue services after intoxication (31.2% vs. 21.3%, P<0.001). In 92.6% of cases, the route of poison administration was through oral ingestion. Oral route was more frequent in intentional patients (96.7% vs. 82.0%, P<0.001). There were two main categories of poisoning substances, namely, pharmaceutical products (53.8%) and agricultural products (22.7%). Chemicals, household products, plant poisons, and animal bites accounted for 9.9%, 7.5%, 5.6%, and 0.1% of the cases respectively. In 0.1% of the cases, the causative substance was unknown. The drugs that were most frequently involved were benzodiazepines (42.1%), acetaminophen (13.6%), anticholinergic sleep inducers (2.2%), tricyclic antidepressants (3.1%), beta-adrenergic blockers (1.7%), opioids (1.6%), methemoglobinemia-inducing agents (1.3%), and calcium channel blockers (0.5%). In the agricultural products, the most frequently involved substances were organophosphate insecticides (19.4%), dipyridylium herbicide (13.9%), glyphosate herbicide (6.8%), and carbamate insecticides (5.6%). In the household products, the most frequently involved substance was sodium hydroxide (28.8%) in cleaning products. In the chemical agents including gases, the most frequently involved agents were carbon monoxide (49.8%), cyanide (6.9%), hydrofluoric acid (3.7%), and toxic alcohols (3.5%). In the plant poisons and animal bites, the most frequently involved agents were mushrooms (28.5%) and snake bite (20.2%). Compared to the unintentionally poisoned patients, the intentionally poisoned patients were more likely to be poisoned by pharmaceuticals (57.2% vs. 45.8%, P<0.001) and agricultural products (26.8% vs. 13.1%, P<0.001).
In treatment, 55.2% of the patients were initially treated at the ED and the remaining 44.8% were managed previously by prehospital emergency medical services or primary care hospitals. On arrival at the ED, 8.7% of the patients were asymptomatic. Less asymptomatic patients were in the intentionally poisoned patients (6.4% vs. 14.8%, P<0.001). More than half of cases (53.1%) exhibited minimal toxicity but there was no significant difference (54.1% vs. 60.7%). In 22.3% of cases, the toxicity was moderate; this was more common in intentionally poisoned cases (25.7% vs. 16.9%, P<0.001). In 11.3% of cases, the toxicity was more severe in intentionally poisoned patients (13.3% vs. 7.3%, P<0.001). In total, 0.4% of the cases died. There was no significant difference between intentionally and unintentionally poisoned patients in terms of fatality rates (0.5% vs. 0.2%).
In 71.6% of the cases, the poisoning was managed by general supportive therapies. Another 32.0% was treated by gut decontamination, 23.6% received activated charcoal, and 2.1% underwent forced renal elimination. Only 4.7% of the patients actually received antidotes. These were N-acetylcysteine (n=49), pralidoxime and atropine (n=47), flumazenil (n=29), antivenin (n =25), methylene blue (n=14), atropine (n=4), naloxone (n= 3), vitamin K1 (n=3), high fractional oxygen inhalation (n=3), and others. Of the patients who received an antidote, 64.5% arrived with moderate to severe toxicity at the hospital and 3.1% died of moribund state at hospital discharge.
Of the all patients, 48.0% were discharged without toxicity symptoms from the EDs. 18.9% were admitted to the intensive care unit, while 48.2% were hospitalized. 3.2% (157 patients) died. Compared to the unintentionally poisoned group, the intentionally poisoned cases were significantly more likely to have death as outcomes (4.0% vs. 0.8%, P<0.001).
The 4,870 acute poisoning patients were then stratified according to clinical severity by using the poisoning severity score. The 1,951 (40.1%) patients with moderate, severe, or fatal poisoning were deemed to have been potentially eligible for antidote treatment. Of these, 855 (17.6% of the total patients) would have been eligible for treatment with antidotes that matched the poisons. Of these, 719 (14.8%) would have been eligible for emergency antidotes. However, only 92 (1.9%) actually received emergency antidotes other than activated charcoal (Fig. 1).
Estimation of the stocking amount at EDs
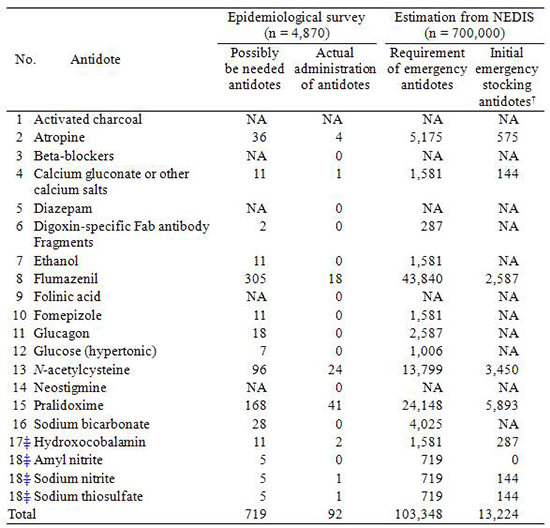
The numbers of adult doses of the 18 emergency antidotes that should be stocked by EDs were estimated extrapolating the data from the multicenter epidemiological study to the NEDIS data (Table 5). The NEDIS is the largest and representative data system about the patients who admitted at Korean EDs. The injury surveillance report, which is generated by the Korea Centers for Disease Control and Prevention, is a comprehensive nationwide epidemiological surveillance analysis including poisoning patients. The NEDIS data showed that every year between 2,400,000 and 2,900,000 patients visit about the 124 EDs throughout Korea that participate in NEDIS. The overall frequency of poisoning cases exceeds 1.7% and more than 700,000 patients presented with acute poisoning each year. It was assumed that the cohort of poisoning patients in the epidemiological study was a good sample of the poisoning cases recorded in NEDIS. Extrapolation of these two frequencies to the 700,000 poisoning patients recorded in NEDIS data.
The ideal and minimum quantities of the 18 emergency antidotes that should be stocked by the 124 NEDIS-participating EDs to treat acute intoxication patients were calculated on the basis of the epidemiological data. It was estimated that 103,348 (14.8%) adult doses of the 18 emergency antidotes should be available for possible emergency treatment. Of these, 13,224 (1.9%) adult doses (575 of atropine, 144 of calcium gluconate or other calcium salts, 2,587 of flumazenil, 3,450 of N-acetylcysteine, 5,893 of pralidoxime, 287 of hydroxocobalamin, 144 of sodium nitrite, and 144 of sodium thiosulfate) would be needed and should be stocked at EDs in Korea for maintaining the present level of initial treatment with emergency antidotes.
DISCUSSION
In this study, we made the list of 18 emergency antidotes that should be stocked at EDs in Korea and estimated that about 13,224 adult doses of emergency antidotes (575 of atropine, 144 of calcium gluconate or other calcium salts, 2,587 of flumazenil, 3,450 of N-acetylcysteine, 5,893 of pralidoxime, 287 of hydroxocobalamin, 144 of sodium nitrite, and 144 of sodium thiosulfate) would be needed for maintaining the present level of initial treatment with emergency antidotes at EDs in Korea. To the best of our knowledge, this is the first study to make the list of emergency antidotes stocked at EDs and estimate the stocking amount of antidotes at EDs in Korea.
Our expert panel initially reviewed more than 40 antidotes that were derived from the list of antidotes that were recommended by the World Health Organization International Programme on Chemical Safety, US expert consensus guidelines, and other sources (4, 6, 7, 8, 9, 13, 14, 15, 16, 17, 18). The panel members reviewed these recommendations in the unique aspects of the poisoning epidemiology in Korea and classified the effectiveness and urgency of availability of each antidote. Urgency of antidote availability was determined on the basis of several time-based classification systems (8, 12). The classifications were based on the stocking model where only the antidotes that are immediately required (within 30 min) are stocked at the ED.
Finally, the panel recommended 18 emergency antidotes that should be stocked at the EDs. The two treatment options for cyanide intoxication, a combination of amyl nitrite, sodium nitrite, and sodium thiosulfate, were counted as one antidote. Ethanol and fomepizole, which are both used for toxic alcohol exposure, were counted separately because while ethanol can be stocked in all hospitals, fomepizole can only be available in limited numbers of principal deposits due to high cost. Fewer and different emergency antidotes were identified relative to the routine stock of 24 antidotes that are stocked by EDs in the US (19). This reflects the clinical experiences of the panel members and factors that characterize the poisoning epidemiology in Korea. The panel also recommended four antidotes that have Class II effectiveness because they are universally accepted as being effective despite the supporting research being limited.
As indicated above, more than two different antidotes can be used to effectively treat toxic alcohol exposure (ethanol and fomepziole) and cyanide toxicity (hydroxycobalamin and an amyl nitrite/sodium nitrite/sodium thiosulfate-based kit). In both cases, the panel designated a preferred agent, although both agents were recognized as being equally acceptable. The preference was determined in the same manner as the decision to recommend stocking an antidote, namely, by group debate until a consensus without any votes of strong disagreement was reached. Fomepizole was preferred over ethanol because a commercially available 10% solution is not available in Korea, which means that a 10% solution must be compounded from a 95% solution of ethanol. Fomepizole thus has the advantages of simplicity of use, the lack of need to compound in the pharmacy, reduction in medication errors, the potential to avoid hemodialysis, and the greater anticipated safety in children. However, fomepizole is too expensive to be stocked by every hospital. Hydroxocobalamin was preferred over the conventional cyanide antidote kit because of its wider indications, ease of use, and anticipated safety in widespread use. However, hydroxocobalamin is also quite expensive at present.
The decision to stock certain antidotes is, by its nature, somewhat arbitrary. Although the list generated by the present study was based on published recommendations (13, 20), it is not intended to be a definitive list of antidotes and doses that must be carried by every ED. Rather, the analysis in the present study is intended to provide emergency physicians with some of the tools needed to help make these stocking decisions. Antidotes vary with regard to efficacy and redundancy. Several antidotes, including chelating agents, and exotic agents, were excluded because they were either unlikely to be administered annually anywhere in Korea or they were unlikely to be given empirically in smaller centers within 4 hr of presentation. Thus, some EDs may elect not to carry some of the antidotes that were included on the list. The frequency was adjusted with the data of the US national database which collects information reported to approximately 65 poison centers, and is estimated to reflect 95% of the US population (21). Cases that involved the use of an antidote and a call to a poison centre were collected and divided by the population base serviced during that interval. The US national database collects the information that is involved the use of an antidote within the initial 1-4 hr window and in this database, commonly administered antidotes as more than once/year/100,000 population included N-acetylcysteine, activated charcoal, naloxone, flumazenil and NaHCO3 (22). In this study, we estimated commonly administered antidotes as more than once/year/100,000 population in Korea with a population of about 49 million which included pralidoxime, N-acetylcysteine, flumazenil, and atropine. Activated charcoal and NaHCO3 were precluded from this survey. This result could be originated from that pesticides were the most prevalent cause of severe poisoning in Korea (1).
The survey data of the present study showed that about 45% of the patients who visited the 11 surveyed hospitals were transferred from other hospitals. The present study is based on the assumption that moderate-to-severely poisoned patients will be admitted to EDs that can provide specialized treatment for poisoning. In Korea at present, there is a shortage of clinical toxicologists and hospitals that can treat poisoned patients appropriately. As a result, the most severe cases of poisoning are transferred to higher levels of hospitals that have a clinical toxicologist. Korean EDs are categorized into three levels: regional emergency medical centers, local emergency centers, and local emergency facilities. Their numbers slightly vary every year: at the end of 2011, there were 452 EDs (142 regional and local emergency medical centers, 313 local emergency medical facilities). Local emergency facilities are designed to treat no serious patients. Local emergency medical centers are always on standby with equipped staff on duty to care for emergency patients with more than one specialist in charge. Each metropolitan city or province is appointed one regional emergency medical center that is designed to treat critically ill patients from each region. Thus, moderate-to-severely poisoned patients are usually transferred to local and regional emergency medical centers. Including all regional emergency medical centers, 140 regional and local emergency medical centers participated in NEDIS in 2010; by the end of 2011, 142 emergency medical centers were participating. In 2010, more than 10,000,000 patients were admitted to more than 590 EDs in a year. Of these, about 4,000,000 patients visited the 140 NEDIS-participating EDs. It is usual situation that most of the moderate-to-severely poisoned patients visited or were transferred to NEDIS-participating EDs. The poisoned patients who are recorded in NEDIS are thus likely to be the most of moderate-to-severely poisoned patients who need emergency antidotes for acute treatment at EDs.
In the present study, two categories of poisoning materials were frequently involved in the poisoning cases identified by the epidemiological study. One was pharmaceuticals which were more frequently involved poisoning agents in urban area. The other was agricultural products which were more commonly involved in rural area poisoning cases. This finding was similar to other report (23). Benzodiazepine group drugs were the most prevalent poisoning drugs, like in Europe, where the benzodiazepines are frequently detected (24). Organophosphate insecticides followed by dipyridylium herbicides were the most commonly involved agricultural products.
Antidotes seemed to be infrequently used to treat acute poisoning in the EDs: less than 5% of the poisoned patients were administered 36 antidotes. This actual administration rate is quite low and there was a lack of concrete evidence for appropriateness in antidote usage in this study. Given this limitation, the poisoned patients identified by the epidemiological study were stratified on the basis of the clinical severity of poisoning by using the poisoning severity score (11). This is used to classify acute poisoning cases regardless of the type and number of agents involved. It takes into account the overall clinical course and should be based on the most severe symptoms only including both subjective symptoms and objective signs. Therefore, it is normally a retrospective process that requires follow-up of cases. If the grading is undertaken at any other time such as on admission, the time point of the data on which the grading is based must be stated clearly. In the present study, the data were from a data warehouse that prospectively gathered the poisoning severity data and from a retrospective chart review. These data showed that 33.6% of the patients had moderate or severe toxicity and that 0.4% of patients died. Present study included only poisoned patients without other exposed cases to toxic substance.
In deciding the type and number of antidotes which should be stocked, the incidence of poisonings that require special antidotes should be taken into consideration. Antidotes needed immediately (within 30 min) must be stocked at all hospitals and antidotes needed within 2 hr can be stocked at certain main hospitals; patients can be taken to these hospitals for treatment or the antidotes can be transported within the time limit to the health facilities at which treatment is provided (25). Antidotes needed within 6 hr may be stocked at central regional depots, provided that there are adequate facilities for transporting them within the time limit (25).
This study had several limitations. First, the efficacy of some of the antidotes that were deemed essential in this study is supported by only limited epidemiological evidence in Korea. Second, the results are based on a survey of acute poisoning. It is conceivable that those completing the survey may have underestimated the minimum amount of antidote that should be administered. Third, the recommended stocking quantities of the antidotes were based on the clinical severity of the poisoned patients. The data precluded correcting the occasional inappropriate or unnecessary use of certain antidotes, and for antidote not being administered due to lack of availability. Fourth, the recommended stocking amount was based on the incorporation of the depot model for expensive and infrequently used antidotes. However, we could express the model in this study. Lastly, it was designed to only estimate how much of each antidote should be stocked for the initial adult doses when treating acutely poisoned patients. These estimations do not consider the antidote needs in the case of a mass casualty event.
Conclusively, the list of 18 emergency antidotes that should be stocked at EDs in Korea was recommended by a panel of clinical toxicologists with multiple specialties. It was estimated that about 13,000 adult doses (575 of atropine, 144 of calcium gluconate or other calcium salts, 2,587 of flumazenil, 3,450 of N-acetylcysteine, 5,893 of pralidoxime, 287 of hydroxocobalamin, 144 of sodium nitrite, and 144 of sodium thiosulfate) would be needed for the initial antidote treatment of poisoned patients at EDs every year in Korea. Future research should focus on determining the entire treatment quantities that are needed, the different kinds of antidotes that are required in rural and urban areas, and the future development and implementation of evidence-based guidelines.





 XML Download
XML Download