

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Endometrial carcinoma is one of the most common gynecologic cancers detected in Europe and the United States (1), and its incidence is increasing in Korea and other Asian countries due to higher fat diets and longer life spans. Exploratory laparotomy through a midline incision, total abdominal hysterectomy (TAH), bilateral salpingo-oophorectomy, peritoneal washing, and dissection of the pelvic or both the pelvic and para-aortic lymph nodes constitute the standard procedures used for the surgical staging of endometrial carcinoma (2). Recently, due to advances in the use of laparoscopic surgical techniques, laparoscopy has been reportedly used for both the exact staging and the effective treatment of endometrial carcinoma. It has also been demonstrated that laparoscopic surgery results in shorter hospital stays, earlier recovery times, and a better quality of life (3, 4, 5).
Obesity is a common risk factor for uterine neoplasia, and accounts for more than half of the patients with endometrial cancer (6, 7). Obesity also greatly increases the risk of developing endometrial cancer by as much as 40%. An earlier study reported that obesity is associated with a two- to five-fold increase in the risk of endometrial cancer in both pre- and postmenopausal women (8). There is also a linear increase in the endometrial cancer risk with an increasing body mass index (BMI) (9). However, the influence of a high BMI on the prognosis of endometrial carcinoma remains controversial. Obesity has been associated with a worse prognosis of endometrial carcinoma in several published studies, although there was no association in other and in Korean population studies (10, 11, 12, 13, 14). Obesity was once a contraindication for advanced laparoscopic procedures (15, 16), although this has recently been reconsidered (17). Improved instrumentation and techniques have allowed the safe use of many advanced laparoscopic procedures in women with a high BMI (18, 19, 20, 21, 22). However, there are few reports regarding the feasibility of laparoscopic hysterectomy and dissection of the pelvic or both the pelvic and para-aortic lymph nodes in obese Korean women. Therefore, study attempted to evaluate the feasibility and survival outcome of laparoscopy in obese Korean women with endometrial cancer.
MATERIALS AND METHODS
The medical records of all patients with uterine cancer who were treated at Asan Medical Center between January 1999 and August 2012 were retrospectively reviewed after we received institutional review board approval. In total, 555 patients with endometrial cancer were identified and all had undergone surgery at Asan Medical Center. Of these patients, 270 underwent open surgery and 285 underwent laparoscopic surgery. Four patients did not receive adequate follow-up examinations following surgery, and the medical records of three other patients were missing. As a result, 278 patients with early-stage endometrial cancer were eligible for inclusion in study. All of these patients were diagnosed using pelvic examinations and imaging modalities. They were divided into three groups, non-obese (BMI<25.0), overweight (BMI 25-27.99), and obese (BMI≥28.0), which is more strict and higher classification than the proposed International Obesity Task Force (IOTF) classifications for BMI in Asia (23, 24). The Korean Ministry of Health and Welfare and IOTF defined obesity in Korea and Asia as BMI≥25, however, we defined obesity as BMI≥28.0 in our study in order to reach global standard and to truly evaluate the feasibility and safety of laparoscopic surgery in obese women. Board-certified gynecologic oncologists performed the surgical procedures in all patients.
One of our patients in whom we performed laparotomy due to stromal adenocarcinoma with adenosquamous features, was included in our study cohort because most of the procedure was finished at the time of the frozen section was sent.
Laparoscopic pelvic lymphadenectomy was not performed in patients diagnosed with stage IA tumors and who had grade 1 differentiation with favorable histological findings. Therefore, pelvic lymphadenectomy was performed in patients with differentiation of grade 2 or above in stage IA, and unfavorable histological types, such as type II endometrial cancer, regardless of the stage and differentiation of the grade. Para-aortic lymphadenectomy was performed in patients with serous, adenosquamous, clear-cell or grade 3 tumors and in tumors with frozen sections demonstrating >50% myometrial invasion. If grossly enlarged lymph nodes were not seen or if no metastases in the pelvic lymph nodes were found on analysis of the frozen sections, para-aortic lymphadenectomy was performed on the areas below the inferior mesenteric artery. Para-aortic lymphadenectomy above the infra mesenteric artery (IMA) was performed when there was an extra-uterine lesion seen on frozen sections or type II histology detected on the pre-operative dilation & currettage (D&C) biopsy. In our study, there were 12 patients who underwent para-aortic lymphadenectomy above the IMA.
A drain was inserted in all of the patients who underwent lymphadenectomy and in six of the 31 patients who underwent simple hysterectomy. Patient age, parity, BMI (kg/m2), histological type, International Federation of Gynecology and Obstetrics (FIGO) surgical stage (25), the number of harvested lymph nodes, operative time, post-operative hospital stay (calculated from the date of surgery to the date of discharge), estimated blood loss (EBL), need for intra-operative or post-operative blood transfusion, intra-, post-operative, and long-term complications, conversion to laparotomy, disease recurrence, and death were recorded as clinical parameters. Conversion to laparotomy, ureteral, bowel, bladder, and vascular injuries, an EBL>1,000 mL, and blood transfusion were considered intra-operative complications. The surgical staging was determined according to the FIGO 2009 staging system (25). The dates and locations of any recurrences were recorded. Overall survival (OS) was calculated from the date of surgery to the date of the last follow-up examination or a patient's death. Disease-free survival (DFS) was calculated from the date of surgery to the date of recurrence or to the last follow-up examination in patients who did not develop recurrence. Statistical analyses were performed using SPSS (version 12.0). The Kaplan-Meier method was used to determine the recurrence rate, DFS, and OS for all patients. The log-rank test was also used to compare survival outcomes. Statistical significance was defined as P<0.05.
RESULTS
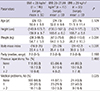
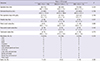
Patient age, height, parity, and history of previous laparotomies were similar in the three patient groups (Table 1). Obese patients demonstrated more medical problems than the non-obese and overweight group patients (P=0.025). Disease characteristics, procedures, and adjuvant treatments for the study subjects are indicated in Table 2. There were no significant differences between the non-obese, overweight, and obese groups in terms of the surgical stage, histology, procedure, and type of adjuvant therapy. The majority of women in the three groups were diagnosed with stage I endometrioid tumors. There were no differences between the non-obese, overweight, and obese patient groups in terms of the proportions of women who required lymphadenectomy (86.8% vs. 93.8% vs. 95.7%, respectively, P=0.067). Lymphadenectomies had not been performed on 22 of the study patients (11.1%).
There were no significant differences between the non-obese, overweight, and obese groups in terms of the operative time (180.7 vs. 182.8 vs. 184.5 min; P=0.124), hospital stay (7.9 vs. 8.4 vs. 8.2 days; P=0.831), EBL (233.3 vs. 244.6 vs. 261.6 mL; P=0.739), post-operative drop in Hb (1.9 vs. 2.0 vs. 1.9 g/dL; P=0.748), and the total number of harvested lymph nodes (28.9 vs. 27.6 vs. 28.3; respectively; P=0.770; Table 3).
The median follow-up time for the non-obese, overweight, and obese patient groups were 71.7 (range, 8.3-152.4), 75.9 (range, 6.3-131.1), and 80.8 months (15.4-139.5) (P=0.460). In total, the median follow-up time for the 278 patients was 74.1 months (range, 6.3-152.4). The rates of recurrence, death, disease-free survival, and overall survival were similar in the three groups (Fig. 1).
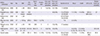
All of the patient groups were similar in terms of their need for intra-operative blood transfusion and the incidences of intra-, post-operative, and long-term complications. There were no complications related to the insertion of the laparoscopic trocars. Among the non-obese patients, two developed intra-operative complications including, respectively, small-bowel injury that required bowel repair and bladder wall weakening because of dissection from the uterus with severe adhesion that required reinforcement. Three, overweight women developed intra-operative complications, including, respectively, bladder-wall weakening due to dissection from the uterus that required reinforcement, EBL more than 1,000 mL, and conversion to laparotomy due to cervical stromal invasion by endometrioid and adenosquamous tumors, was all of which were noted on the frozen sections. One obese woman developed intra-operative complications including left, internal, iliac-vein injury that required primary repair with EBL more than 1,000 mL (Table 4).
DISCUSSION
The words, "small" and "lean", have always been used to describe Asian populations, and the prevalence of obesity in Korea, and in Asia in general, is lower than elsewhere in the world. However, the incidence of obesity and related diseases are increasing (23). The incidence of endometrial cancer is also increasing in Korea and in other Asian countries. Women with a high BMI also frequently develop endometrial cancer. Obesity is one of the most important risk factors for the development of type I endometrial carcinoma, particularly in postmenopausal women (26).
Many previous studies have shown that the use of total laparoscopic hysterectomy and laparoscopic-assisted vaginal hysterectomy are associated with a significant decrease in blood loss, the need for transfusions, postoperative pain, and the duration of hospitalization compared with the use of open surgery for the treatment of endometrial cancer (27, 28, 29, 30, 31).
In order to minimize the risk of intra- and post-operative complications, a less invasive laparoscopic surgical approach would be helpful in this setting. The role of vaginal surgery is restricted by the need to harvest lymph nodes for complete nodal staging, although it also demonstrates many advantages by reducing morbidity and the operative time (32).
Since the first report describing the use of laparoscopic surgical staging to assess two patients with clinical stage I endometrial cancer (33), the use of laparoscopic surgery for the management of gynecologic cancer, including endometrial cancer, has increased (34). Many studies have since supported the theory that laparoscopic surgery is feasible for the management of patients with early-stage disease (3, 4, 5, 27, 28, 30).
In our study, there were no significant differences between the non-obese, overweight, and obese groups in terms of the operative time, volume of transfused blood, and the EBL. The mean hospital stay of our patients was longer than that reported in other studies, most likely because most Korean patients only want to be discharged after a complete recovery, including the removal of any drainage tubes and stitches and improvement in their general health condition, and the Korean medical insurance system covers this (3).
The no drainage method has been shown to be as effective as the conventional drainage method (35). Patients could probably be discharged sooner by safely removing drainage tubes earlier than several days following their procedure or by completely avoiding the need for drainage tubes. We did not close the retro-peritoneum following laparoscopic lymphadenectomy in order to allow the free flow of lymphatic fluid into the peritoneal space, and thus resulting in a lower incidence of lymphocyst formation.
In our study, there was no difference in terms of the operative time and the rate of transfusion compared to those in previous studies, and our study showed a lower rate of intra- and post-operative complications, a larger number of retrieved lymph nodes, and a better survival outcome after the longest follow-up period (Table 5). Farthing et al. (19) reported a short operative time and low EBL compared to previous studies, including our study. This is probably due to the relatively low rate of lymphadenectomy of 3.1%.
The complication rates observed in the three patient groups in our study were low, which highlights the safety of the surgical approach. Intra-operative complications included injuries to the great vessels, bladder, and bowel serosa. No vascular injuries developed while using the closed method to insert the trocar. One patient developed a vascular injury during a lymphadenectomy. This was repaired by clip ligation, and the patient did not undergo a laparotomy. Other complications were also resolved during surgery, and no conversions to laparotomy were required as a result of the intra-operative complications.
A recent study from an ancillary data analysis of the Gynecologic Oncology Group (GOG) LAP2 also revealed that there was no difference in intra-operative complications in obese patients (14). This indicates that obesity is not an obstacle for performing both open and laparoscopic surgery for endometrial cancer. A higher post-operative complication rate was observed in the higher BMI groups as the frequency of these complications increased significantly at a BMI higher than 30 for the duration of the use of antibiotics, and at 35 for venous thrombophlebitis and wound infection (14). The etiology of the difference in post-operative complications between Western studies and our study might be due to the fact that Korean patients are less obese compared to those patients in Western studies. However, the mean BMI of the obese group in our study was 30.9 with a range of 28 to 42.2, and which was also sufficiently 'obese' for the Western criteria. In addition, the aim of the study based on ancillary data of GOG LAP2 was to investigate the association of obesity on complications, recurrence, and survival outcome in endometrial cancer patients regardless of the type of surgery rather than investigating the surgical feasibility and survival outcome of laparoscopic surgery, as in our study (14). Increasing BMI did not impact the rate of post-operative complications of laparoscopy in another Western study (21). This indicates that not only the severity of obesity, itself, but also the difference in patient characteristics in terms of diet, socio-behavior patterns, ethnic group, and differences in study design should be considered and investigated for determining the differences in surgical and survival outcomes.
There are few reports regarding the feasibility of laparoscopic surgery in obese Korean women. To our knowledge, ours is the first study regarding the surgical feasibility and safety of laparoscopic surgery for treating endometrial cancer in obese Korean women. In our study, laparoscopic surgery was feasible in terms of the intra- and post-operative complications, such as one of the previous reports of GOG LAP2 study data which compared laparoscopy with laparotomy for comprehensive surgical staging of endometrial cancer (36).
The rate of conversion to laparotomy in laparoscopic surgery was 1.04% to 10.6% in previous studies (18, 19, 27, 37). In contrast, Walker et al. (36) and Scribner et al. (38) reported the conversion rate in their studies as 25.8% and 36.4%, respectively. In our study, there was only one case of conversion in the overweight group and thus with a rate of 1.3%. Walker et al. (36) revealed that conversion to laparotomy is associated with obesity, metastatic disease, and increasing age. In our study, the rate of extra-uterine spread was lower and the mean age was younger than that of the GOG LAP2 data. However, the mean BMI of the obese group in our study was higher than the GOG LAP2 data, indicating that the reason for the difference in conversion rate between the two studies should be considered with other factors including the rate of metastatic disease and patient age rather than only obesity itself. The surgeon's preference and clinical experience as well the conventions of medical institutions should be considered, although these are difficult to quantify.
We assume that the most important factor is the difference in the rate of pelvic and/or para-aortic lymphadenectomy. Walker et al. reported that 98.3% of their patients underwent lymphadenectomy and 91.9% underwent para-aortic lymphadenectomy, and Scribner et al. reported the utility of laparoscopy in lymphadenectomy and all patients in this study underwent pelvic and para-aortic lymphadenectomy (36, 38). In contrast, Farthing et al. (19) performed lymphadenectomy in 3.1% of all of their patients. Eltabbakh et al. performed pelvic lymphadenectomy in 77.5% of their patients and para-aortic lymphadenectomy in 17.5% of the patients in his earlier study, and with 75.7% for pelvic and 21.1% for para-aortic lymphadenectomy in his later study, while Obermair et al. performed lymphadenectomy in 67.8% of their patients (18, 27, 37). In our study, 98.8% and 95.7%, respectively, underwent lymphadenectomy, and 26.8% and 31.4% underwent para-aortic lymphadenectomy in the overweight group and the obese group.
Giugale et al. reported that an increasing BMI in laparoscopic surgery patients decreases the frequency of lymphadenectomy and the number of harvested para-aortic lymph nodes with 4.6 in the obese group with a BMI of 30-39 and 2.2 in the morbidly obese group with a BMI of 40-49 (39). Helm et al. (21) also reported that the performance of para-aortic and pelvic lymphadenectomy had an inverse relationship with an increasing BMI, although an increasing BMI did not impact the number of para-aortic and pelvic lymph nodes removed. Scribner et al. and Eltabbakh et al. harvested 6.6 and 2.5 para-aortic lymph nodes in their studies (27, 38). In our study, 5.3 and 3.7 para-aortic lymph nodes were harvested in the overweight group and the obese group, respectively, and which seems to have no significant difference compared to previous studies.
Although not statistically significant, the obese group showed less recurrence and death in our study. The association between obesity and the prognosis of endometrial cancer remains controversial. Previous studies have suggested that obesity is associated with a worse prognosis, while there no relationship seen in other studies (10, 11, 12, 13). Gunderson et al. (14) recently reported that a high BMI was not associated with the patient survival outcome, but showed a lower recurrence although not of statistical significance. This is probably because an increasing BMI shows a lower FIGO stage, a higher proportion of well-differentiated endometrioid type tumors, and a lower risk factor for recurrence such as lymph node/ovarian metastasis, as well as positive cytology as defined by Keys et al. in GOG 99 (14, 40). Also in a previous Korean population study, overweight and obese women had an earlier FIGO stage with less cervical extension and positive peritoneal cytology (13).
As seen in previous studies, there were no significant differences from our study in terms of the disease-free and overall survival rates in our three patient groups. It indicates, therefore, that the use of laparoscopic surgery to manage obese patients has no appreciable impact on their prognosis (22).
The limitation of our study is its retrospective design and the possibility of a selection bias as most of the laparoscopic surgeries were chosen by the patient and/or surgeon based on their preference and decision, although there was no difference in the patient characteristics in the three groups. At the same time, this is the largest Korean study to date to directly investigate the surgical and survival outcomes of obese Korean patients with endometrial cancer who underwent laparoscopic surgery during such a long study period. In conclusion, our findings indicate that laparoscopic surgery is a safe and feasible procedure for managing obese, Korean, early-stage endometrial carcinoma patients and does not appear to affect the prognosis in these cases. Large, randomized, prospective, multi-center studies regarding the safety and feasibility of laparoscopic surgery for the management of obese Korean women with early endometrial carcinoma are still needed.



 XML Download
XML Download