

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lung cancer is the most common cause of cancer deaths in both men and women in Korea. In 2010, the number of incidence of lung cancer was 14,650 among men and 6,061 among women, and the age-adjusted standardized incidence rate per 100,000 persons was 47.2 and 14.8 in men and women, respectively (1). Smoking is the predominant cause of lung cancer, followed by occupational and environmental exposure. The global burden of occupational lung cancer was first estimated in 1981 at 15% of total lung cancer cases (2). Several studies (2,3,4) were subsequently conducted to determine the population attributable fraction (PAF) of occupational lung cancer, reporting a range of 8% (4) to 29.0% (3). The PAF study of occupational lung cancer in Korea was conducted two times in 2009 and 2010. Kim et al. (5) calculated the PAFs of occupational lung cancer caused by 9 lung carcinogens using the International agency for research on cancer (IARC) relative risks (RRs) and Korean RRs, which were 7.0% and 3.7%, respectively. The estimated number of occupational lung cancers ranged from 630 to 1,181 incidence cases in 2005 (6). Son et al. (7) estimated that the PAF of occupational lung cancers was 26.1% for incident lung cancer cases and 26.3% for lung cancer deaths.
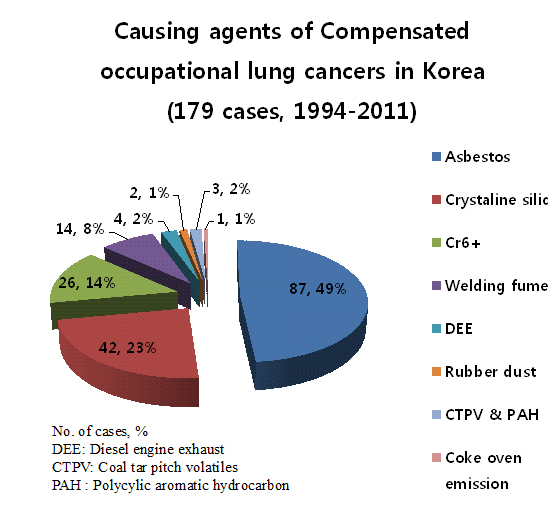
Despite being expected to the large number of occupational lung cancers in Korea, the number of compensated occupational lung cancers as approved by the Korea Workers' Compensation and Welfare Service (KCOMWEL) is approximately 10 to 20 cases per year. The first documented case of compensated occupational lung cancer in 1994 involved a worker who produced heat insulator contained asbestos (8). From 1994 to 2011, 179 lung cancers have been compensated by the KCOMWEL.
An understanding of the characteristics of occupational lung cancer is important to make policies that prevent carcinogen exposure and refer to compensation criteria for workers who develop lung cancer due to these occupational exposures. So, the authors analyzed the characteristics of occupational lung cancers that were compensated under the Industrial Accident Compensation Insurance Law (IACIL), which is operated by the KCOMWEL. Through this study, it is available for grasping such epidemiologic characteristics as the kinds of carcinogen, the disease latency, carcinogen exposure duration, and the type of industry and job of workers with compensated occupational lung cancers.
MATERIALS AND METHODS
Using KCOMWEL's electronic database, 179 cases of compensated occupational lung cancers were identified between 1 January 1994 and 31 December 2011. Each of these 179 cases was reviewed and the epidemiologic characteristics of these cases were analyzed.
Three additional sources of data were used to obtain more information about these 179 cases. The first data source was the Survey of Occupational Accidents and Diseases, which has collected data from workers who have been compensated with occupational diseases through direct interview, telephone, and mail surveys conducted by the Korea Occupational Safety and Health Agency (KOSHA) since 1999. The second data source was epidemiological investigation reports produced by the Occupational Safety and Health Research Institute (OSHRI) of KOSHA. Since 1992, OSHRI has been investigating the workers and workplaces of claimed cases to determine the work-relatedness of each case. The diseases which were related to the work environment by a probability of more than 50% were considered as occupational diseases. Although this probability was decided by a panel of occupational physicians and hygienists, there are no consistent objective criteria to determine the probability. The third data source was epidemiological investigation reports produced by the Occupational Lung Disease Institute (OLDI) of KCOMWEL. Like OSHRI, OLDI has also been investigating the relationship between the work environment and claimed cases of lung diseases, including lung cancer, since 2007. The investigation process and recognition criteria are similar to those of OSHRI.
Among 179 cases, 99 cases (55.3%) and 27 cases (15.1%) had been investigated by OSHRI and OLDI, respectively. The other 53 cases (29.6%) were recognized as occupational lung cancers by the physician advisory committee of KCOMWEL. This committee adopted the diagnostic criteria in the Enforcement Ordinance (an annexed list 3) of the Industrial Accident Compensation Insurance Act (IACIA). For example, this committee determined without an epidemiological investigation from OSHRI or OLDI that the lung cancer of a female worker with no smoking history who had worked more than 10 yr at an asbestos textile factory was an asbestos-related occupational lung cancer.
For each case, the general characteristics of the workers (e.g., gender, age at cancer diagnosis, smoking status), clinical findings (e.g., pathology and chest CT), occupational exposure history (e.g., type of occupation, type of carcinogen exposure, duration of exposure, and disease latency), and the type of industry were analyzed. The time of the first exposure was considered as the first exposure to a lung carcinogen regardless of the start of employment. In many cases, workers had been exposed to several types of lung carcinogens in addition to the major causative carcinogen. In these cases, the duration of exposure added the durations of individual lung carcinogen exposures and then subtracted periods in which individual exposures overlapped. The latency was defined as the duration between the first exposure and the date of diagnosis of the lung cancer.
Industries were classified by the 9th version of Korea Standard Industrial Classification (9th KSIC), which is based on the International Standard Industrial Classification (ISIC) adopted by the United Nations.
Ethics statement
This study protocol was approved by the institutional review board (IRB) of Dongguk University Ilsan Hospital (IRB No. 2013-91). This study used the secondary data and all information was collected for 18 yr via KCOMWEL. So there was no method to follow the study subjects or their families to obtain informed consents. Also, there is no adverse effect on esteem, right, and welfare of study subjects. Therefore the IRB of Dongguk University Ilsan Hospital waived the informed consents to this study subjects.
RESULTS
Recognition rate of compensated occupational lung cancers per 100,000 insured Korean workers
The KCOMWEL compensated 179 lung cancers including 87 asbestos-related lung cancers between 1994 and 2011. Recognition for overall- and asbestos-related occupational lung cancers per 100,000 insured workers were 0 to 0.15 (mean 0.09) and 0.00 to 0.09 (mean 0.05) (Table 1).
Worker demographics
Men accounted for 94.4% (169 cases) of recognized cases. The absolute number of compensated cases increased approximately 11-fold, from 15 cases between 1994 and 1999 to 164 cases between 2000 and 2011.
The mean age at the time of diagnosis was 53.5 (Standard deviation; SD 8.2) yr old. The most common age group was 50-59 yr old (86 cases), followed by 40-49 yr old (49 cases).
Among 160 cases in which smoking history had been assessed, 74 cases (46.3%) were current smokers and 65 cases (40.1%) were non-smokers. Mean smoking amounts of smokers and ex-smokers were 18.2 pack-years (Table 2).
Characteristics of the workers and work environments
The major causative carcinogen in the 179 recognized cases was asbestos (87 cases, 48.6%), followed by crystalline silica (42 cases, 23.5%) and hexavalent chromium (Cr6+) (26 cases, 14.5%). The mean duration of exposure to lung carcinogens was 19.8 (SD 9.9) yr. An exposure of 20-30 yr was the most common duration (n=78), followed by exposure durations of 10-20 yr (n= 73). The mean duration of the latency period was 23.2 yr. The most common latency period was 20-30 yr (n=80) (Table 3).
The most common type of industry from which cases originated, as classified by the KSIC-9, was manufacturing (112 cases, 62.6%), followed by construction (30 cases, 16.8%), transportation (18 cases, 10.1%), and mining and quarrying (7 cases, 3.9%). Among the 112 manufacturing industries from which cases originated, the most common manufactured product was basic metal products (29 cases, 25.9%), followed by transport equipment (24 cases, 21.4%), non-metallic mineral products (14 cases, 12.5%), fabricated metal products excluding machinery and furniture (13 cases, 11.6%), textiles excluding apparel (8 cases, 7.1%), and motor vehicles, trailers, and semi-trailers (8 cases, 7.1%). Among the 30 construction industries from which cases originated, 14 (46.7%) cases originated from general construction and 16 (53.3%) cases originated from special trade construction (Table 4). The most common types of occupations from which the 179 cases originated were maintenance and repair (29 cases, 16.2%), followed by foundry work (23 cases, 12.8%), welding (22 cases, 12.3%), painting (13 cases, 7.3%), and spinning or weaving (7 cases, 3.9%) (Table 4).
Exposure and pathology characteristics by types of major causative carcinogen
Among all 179 cases, the pathological findings were investigated in 132 cases (73.7%). We classified the 132 lung cancers by IASLC/ATS/ERS (IASLC, International association for the study of lung cancer; ATS, American thoracic society; ERS, European respiratory society) classification in small biopsies/cytology (9, 10). A total of 115 Cases were non-small cell lung carcinoma (NSCLC). Among NSCLC, 64 cases (48.5%) were adenocarcinomas, 38 cases were squamous cell carcinomas, and 1 case was a NSCLC, not otherwise unspecified (NOS). The other 17 cases were small cell carcinomas (Table 2).
The mean exposure duration and latency as categorized by the type of major causative carcinogen were 18.1-20.2 yr and 18.6-24.0 yr, respectively. There was no statistically significant difference in the mean exposure duration or latency by the type of major causative carcinogen. For cases of occupational lung cancer with a co-exposure to two or more lung carcinogens, the mean exposure duration and latency (20.1 and 23.6 yr, respectively) were not statistically different from those cases of occupation lung cancers with an exposure to a single carcinogen (19.6 and 22.8 yr, respectively) (Table 5).
Among 59 asbestos-related occupational lung cancers with a known pathology, adenocarcinoma and squamous cell carcinoma represented 34 (57.6%) and 15 (25.4%) cases, respectively. Among 25 silica-related occupational lung cancers with a known pathology, adenocarcinoma and squamous cell carcinoma represented 12 (48.0%) and 10 (40.0%) cases, respectively. There was no statistically significant difference in the pathology by the types of major causative carcinogen (Table 5).
DISCUSSION
The Industrial Accident Compensation Insurance (IACI), which is operated by KCOMWEL in Korea, covered 14,198,748 workers in 2010, which accounted for approximately 57.4% of the economically-active population (24,748,000 persons) (11). The IACI does not cover self-employed workers or some atypical workers. Also, government employees, private school teachers, and military officers (including soldiers and other military staff) are covered by their own insurance systems. This study included only cases that were compensated by the IACI. In addition, lung cancers in miners with pneumoconiosis (greater than grade 1) were excluded from this study. Since 1999, KCOMWEL has listed lung cancer as a complication of pneumoconiosis and has approved as work-related lung cancer without individual review. However, formal statistics for lung cancers in miners with pneumoconiosis was not available from KCOMWEL. The KCOMWEL just has reported the number of pneumoconiosis not to separate lung cancers with pneumoconiosis. Therefore we excluded lung cancers in miners with pneumoconiosis because we could not grasp it.
This study used all of the electronic data that were available from KCOMWEL on compensated workers, and added variables about the underlying causes of the occupational lung cancers from the epidemiological investigation reports of two institutes above mentioned. However, there was insufficient clinical information, such as radiological findings and pathology, for all of the cases. Therefore, the information available for this study was limited.
In this study, asbestos was the predominant carcinogen (48%) implicated in occupational lung cancers, followed by silica and hexavalent chromium. In 2006, the fraction of recognized asbestos-related occupational lung cancers in Germany, France, and Belgium was 73.2% (721 among 958 cases), 93.6% (1,024 among 1,094 cases), and 88.1% (59 among 67 cases), respectively (12). The fraction of asbestos-related occupational lung cancers was therefore relatively low in Korea compared with these European countries. In addition, the fraction of asbestos-related occupational lung cancers is even lower compared with European countries because the present study excluded cases of lung cancer in miners with pneumoconiosis. Korean researchers have assumed that lung cancers in miners with pneumoconiosis are mainly related to silica exposure. Therefore, silica will be the predominant causal agent of recognized lung cancers if we include the lung cancers in miners with pneumoconiosis. Based on the calculation of the attributable fraction of occupational lung cancers by the type of lung carcinogen in Korea, silica-related lung cancers represent the highest attributable fraction (13.0%) among lung carcinogens, followed by asbestos-related lung cancers (12.4%) (7).
Several studies have examined the association between asbestos-related lung cancer and the pathology. Some studies have shown an increase in adenocarcinoma (13,14,15,16) among asbestos-related lung cancer, whereas other studies have shown an increase in both adenocarcinoma and squamous cell carcinoma (17, 18). In this study, the proportion of adenocarcinoma and squamous cell carcinoma among asbestos-related lung can cers was 57.6% and 25.4%, respectively. Also, the most frequent pathology among silica- and Cr6+-related (including welding) lung cancer was adenocarcinoma. These pathologic distributions of lung cancers are different from that of Korean men reported by the Korea Central Cancer Registry in 2002 (median year of this study), which involved 20.7% adenocarcinomas and 39.8% squamous cell carcinomas (19). Several studies have reported that smoking-related lung cancers are associated with squamous cell carcinoma (19, 20). Therefore, these pathological differences in lung cancers between the general population of Korean men and compensated workers in Korea may not be due to the fact that adenocarcinoma is the predominant pathology type among occupational lung cancers, but rather that adenocarcinoma is more easily recognized as an occupational cancer compared with squamous cell carcinoma. Because the physician advisory committee of KCOMWEL for work-relatedness decision made a judgment that adenocarcinoma might be occurred by exposure to occupational carcinogens including asbestos than to smoking and other risk factors (13,14,15,16).
In this study, the mean latency was not statistically different among the different types of carcinogens. The median latency was 24.0 yr in asbestos-related, 21.5 yr in silica-related, and 21.0 yr in chromium-related (including welding) lung cancers. A prior study has reported that the latency period of asbestos-related lung cancer is approximately 25 yr from the first exposure (21). Another study that analyzed 152 compensated asbestos-related lung cancers in Japan found that the median latency was 47 yr (22). The latency of asbestos-related lung cancer found in this study was therefore shorter than the latency found in the Japanese study. This difference may be due to a different history of asbestos use among Korean and Japanese workers. One German study showed that the median latency of silica-related lung cancers was 40 yr (range 7-69 yr) (23). The present study found a latency of 21.5 yr among silica-related lung cancers, but the range of the latency duration (7-61 yr) was similar to the range reported in the German study. Prior studies have reported that the latency period of chromium-related lung cancers is approximately 20-35 yr (24,25,26,27), which is similar to the latency period, found in this study.
The question of whether asbestos (or silica) or asbestosis (or silicosis) itself is the true risk factor for lung cancer is important issue for surveillance and compensation. Generally the stronger correlation has been shown in lung cancers with asbestosis than in that without asbestosis (28,29,30,31,32). However, some studies have shown an increase in lung cancer mortality in asbestos-exposed workers without clinical, radiological, or pathological evidence of asbestosis (33,34,35,36). In this study, simple chest radiograph or CT scan was available in only 23 cases through the KOSHA epidemiological survey. Two cases reported pleural plaques and another two cases showed evidence of pleural thickening. From these cases, only 6 cases of pulmonary fibrosis appeared to be related to asbestosis. This means that the physician advisory committee of KCOMWEL assumed that asbestos itself might cause lung cancers regardless of asbestosis in this study subjects. Because the committee considered that synergistic interaction between smoking and asbestos itself, which means relatively low dose asbestos exposure comparing to asbestosis, might cause lung cancers. However we would conclude the role of asbestosis through radiological review on other un-reviewed cases among asbestos-related lung cancers in this study. Among 42 silica-related lung cancers in this study, 8 cases (19.0%) had pneumoconiosis. A recent IARC review noted that the rate ratios were similar across studies regardless of silicosis (1.74-2.76 for workers with silicosis and 1.25-1.32 for workers exposed to crystalline silica), which suggests that silica itself causes lung cancer with or without silicosis (37). Based on this review, lung cancers exposed to silica without silicosis can be compensated as occupational lung cancers in Korea.
In Korea, most raw materials that contain asbestos are imported, and most of these raw materials are used to produce construction materials, such as roofing slate, insulating material, and rags. The remains of these raw materials are used to produce friction materials and textile materials (38). However, in this study, only 5 cases of asbestos-related lung cancers were associated with the manufacture of construction materials and only 6 cases were associated with the production of friction and textile materials. In comparison, 15 asbestos-related lung cancers were associated with construction, including demolition. Among Japanese asbestos-related compensated cases in 2005-2006, construction workers accounted for 40.0% (515 workers) of the 1,287 lung cancer cases (39). Based on the results of the Japanese study as well as the amount of in-place asbestos materials that are used in construction, including shipbuilding, in Korea, construction workers have the potential for continued exposure to asbestos during the maintenance, renovation, and demolition of buildings.
Among 42 silica-related lung cancers, 23 cases (54.8%) occurred in foundry workers, followed by stonemasons (8 cases, 19.0%) and tunnel workers (4 cases, 9.5%). These results can be explained by the poor working environment and mixed carcinogen exposure (i.e., polycyclic aromatic hydrocarbons [PAH] and heavy metals such as hexavalent chromium, nickel, and cadmium) in Korean foundries. An analysis of lung cancer morbidity among a Korean foundry cohort that included 17,000 workers found that the standardized incidence ratio (SIR) of lung cancer in production workers was significantly higher (SIR 1.45; 95% confidence interval [CI], 1.11-1.87) than the general Korean population (40). Because granite, which contains silica, is the main rock in Korea, lung cancers among stonemasons and tunnel workers are recognized as occupational diseases.
In 26 chromium-related lung cancers, 12 cases (46.2%) occurred in painters and 8 cases (8 cases, 19.0%) occurred in platers. Paints that contain Cr6+ are mainly used in shipbuilding and manufacturing special-purpose machinery in Korea. Although Cr6+ exposure was not confirmed at the time of the epidemiological investigation, lung cancer in welders is recognized as an occupational disease because these workers are known to be exposed to Cr6+ as well as asbestos, silica, and other carcinogens.
This study has the limitation of using secondary data. So, details about the exposure, such as the cumulative exposure dose, the burden of asbestos fibers or asbestos bodies in the lung, and other clinical information, could not be assessed. However, this study has the strength for including overall occupational lung cancers compensated by the KCOMWEL. Therefore the information extracted from this study will be helpful to make policies that protect workers who are exposed to occupational lung carcinogens and to determine the impact of the work environment on lung cancer for compensation.




 XML Download
XML Download