

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is characterized by a persistent airflow limitation, which is caused by a mixture of small airways disease (obstructive bronchiolitis) and parenchymal destruction (emphysema) (1). The current therapeutic options for COPD are smoking cessation and pharmacologic and non-pharmacologic therapies. Pharmacologic therapies include bronchodilators and corticosteroids, which aim to decrease airway resistance and airway inflammation. However, these treatments show limited effectiveness against the decreased elastic recoil and hyperinflation associated with emphysema (2).
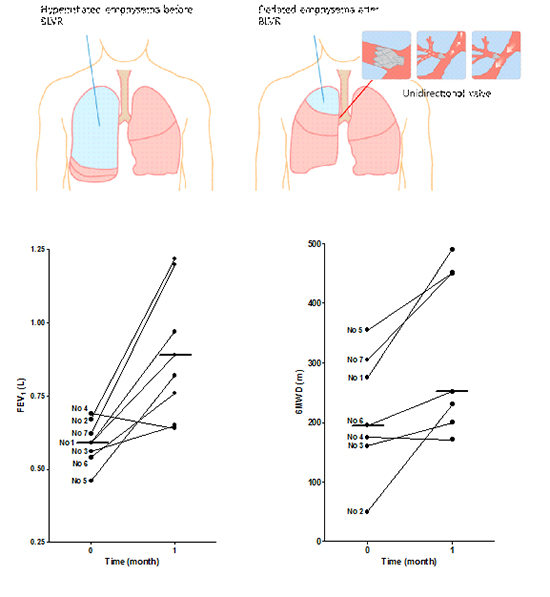
Lung volume reduction surgery (LVRS) is a surgical procedure in which selected areas of the hyperinflated lungs are resected, making respiratory muscles more effective pressure generators and increasing the elastic recoil pressure of the lungs (3, 4). LVRS has been proposed as a palliative treatment for patients with severe emphysema and was shown to improve lung function, exercise tolerance and quality of life in a subgroup of patients with upper lobe-dominant emphysema when compared to medical therapy alone (5). However, the substantial perioperative morbidity and mortality associated with LVRS has led to the development of lower risk and less invasive bronchoscopic techniques that have similar physiologic mechanisms to LVRS. Among them, endobronchial valves (EBVs) are the most widely used devices for bronchoscopic lung volume reduction (BLVR) and have shown promising results. EBVs are bronchial devices that incorporate a one-way valve that blocks the bronchial lumen leading to a targeted region of the emphysematous lung. EBVs have shown acceptable safety and efficacy when used as a unilateral treatment to improve lung function, exercise tolerance, and quality of life in patients with advanced emphysema (6, 7, 8). EBVs have been granted European Community (Communauté Européenne [CE]) mark approval for use in BLVR and many patients worldwide have benefited from the procedure. However, the use of EBVs in BLVR in Asian emphysema patients has been minimal.
In Korea, EBVs were first introduced and approved for BLVR by the Korean FDA in November 2011, with the first case performed in July 2012. The aim of this paper was to report the experience of the first Asian cases of EBV deployment in advanced emphysema patients treated with BLVR.
MATERIALS AND METHODS
Patients
Patients with advanced emphysema who did not respond to standard treatment for COPD were eligible to undergo BLVR. The inclusion and exclusion criteria are listed in Table 1. We recruited subjects which corresponded with such criteria at outpatient or inpatient pulmonary clinic. Between July 2012 and March 2013, consecutive seven patients underwent BLVR at Asan Medical Center, Seoul, Korea. They each had a smoking history of more than 10 pack-years. Dyspnea was persistent despite pharmacologic treatment and pulmonary rehabilitation for more than 3 months. Written informed consent was obtained from each patient before the procedure. All patients received optimal medical treatment at the time of inclusion and no changes were made to their medication regimen after the procedure.
The preoperative evaluation included a physical examination, spirometry, chest radiography, lung perfusion computed tomography (CT) scan, and transthoracic echocardiography, as well as measurements of lung volumes by body plethysmography, diffusing capacity for carbon monoxide (DLCO), and exercise capacity using the 6-min walk distance (6MWD) test. The degree of dyspnea was measured using the modified British Medical Research Council (mMRC) questionnaire. Quality of life was assessed by the St. George Respiratory Questionnaire (SGRQ) and COPD Assessment Test (CAT) (9, 10).
Computed tomography
CT scanning with intravenous contrast medium was performed using a dual-source CT system (SOMATOM Definition; Siemens Healthcare, Forchiheim, Germany) in the dual-energy mode (80 and 140 kV). The perfusion to volume ratio of each lobe was calculated by measuring the iodine to voxel ratio with in-house software. The detailed CT protocol was described in other paper (11). The most hyperinflated and least perfused lobe of the emphysematous lung was selected as the target lobe for BLVR. Additionally, fissure integrity of the target lobe was assessed by a thoracic radiologist. Only patients having complete fissure of the target lobe were selected as subjects (Table 1).
Procedure
Using flexible bronchoscopy, BLVR was performed by placing one-way EBVs in the bronchi supplying the most hyperinflated parts of the emphysematous lungs. Patients were administered inhaled salbutamol and intravenous anesthesia with midazolam before BLVR. The Zephyr® EBV (Pulmonx Inc., Redwood City, CA, USA) was used in all patients in this study. It is a self-expanding nitinol (nickel-titanium) stent with a silicone one-way duckbill valve that allows release of gas and mucus during exhalation but blocks entry of air during inhalation. It is available in two sizes (4.0-7.0 mm and 5.5-8.5 mm) to fit the subsegmental, segmental, and lobar bronchi. These EBVs can be removed or repositioned with bronchoscopy. Before the procedure, the Chartis® System (Pulmonx Inc.) was used to confirm that the target lobe had no collateral ventilation with the non-target lobe. The Chartis® system is an endobronchial catheter-based device for estimating collateral resistance, which assists in the selection of suitable patients for lung volume reduction (12, 13). When the Chartis® system did not give reliable results in target lobe, adjacent lobe was tested instead. If adjacent lobe had no collateral ventilation on the Chartis® system, target lobe was considered to have no collateral ventilation.
The EBV was delivered to the target bronchi using a flexible delivery catheter (with the valve in situ), which was inserted through the working channel of a standard bronchoscope. Valves were places unilaterally in either the lobar, segmental, or subsegmental bronchi in the targeted lobe. The physician determined the number of valves that were required to occlude the target lobe completely. Chest radiographs were taken within 1 hr of the procedure and on the following day to assess atelectasis of the target lobe, diaphragm shift, and pneumothorax.
Follow-up and outcome measures
Follow-up evaluations were performed at 1 month post-procedure. Patients were re-evaluated with chest radiograph, pulmonary function test, exercise tolerance as measured with the 6-MWD test, a quality of life assessment, and any adverse events were noted. Clinical efficacy measures included forced expiratory volume in 1 second (FEV1), the 6MWD test, and the mMRC dyspnea scale.
Statistical analysis
Descriptive statistics were expressed as median and range because of the limited number of patients. The Wilcoxon signed rank test was used to assess the significance of differences between variables at baseline and at follow-up. A value of P<0.05 was considered to indicate statistical significance. Statistical analyses were performed using SPSS, version 19.0 for Windows (SPSS, Chicago, IL, USA).
RESULTS
The demographic and baseline characteristics of all patients are summarized in Table 2. They were aged between 53 and 69 yr and had severe dyspnea, poor lung function and low exercise capacity (mMRC dyspnea scale 3-4; median FEV1, 0.59 L, 19.0% predicted; median 6MWD, 195 m). All patients had severe hyperinflated emphysema with a median residual volume (RV) of 193% predicted. Patient No. 1 underwent BLVR because of persistent air leakage through a chest tube after spontaneous pneumothorax. Surgical bleb resection was considered too dangerous because he had poor lung function.
Endobronchial valve treatment
Most patients had upper lobe predominant emphysema and the right upper lobe was used as the target lobe in all patients except for patient No. 6. The treating physician inserted two to four small or large valves into the bronchi of the target lobe depending on the anatomical variation of the bronchi. The target lobe of each patient, as well as the procedural details, is shown in Table 3.
Treatment efficacy
Subsegmental linear atelectasis of the target lobe and expansion of other lobes were observed shortly after BLVR in most patients. The clinical efficacy of the procedure at 1 month post-procedure is shown in Table 4 and Fig. 1. Among seven patients, six patients showed clinical improvement with no clinical improvement seen in patient No 4.
The median FEV1 significantly increased from 0.59 L to 0.89 L (51%; P=0.028). Other pulmonary functional variables such as forced vital capacity (FVC), RV, and total lung capacity (TLC) also showed improvement although the changes were not statistically significant. Decreases in RV and TLC were noted to parallel increases in FEV1 and FVC. Overall, dyspnea was markedly improved after the procedure (P=0.026): two patients improved to dyspnea scale 1, four patients to 2, and the other patient remained at 4. Other health-related questionnaires (SGRQ and CAT) showed that patients experienced clinical improvement, although data were not present in some patients. The median 6MWD increased from 195 m to 252 m (29.2%; P=0.028).
The post-procedure median FEV1 and 6MWD increased by 60% (0.58 L to 0.93 L) and 49.4% (235 m to 351 m) respectively in the subgroup of patients with clinical improvement (i.e., excluding patient No. 4).
Adverse events
Patients No. 2 and No. 3 had pneumothorax at 5 days and 2 days after the procedure, respectively. The pneumothorax in patient No. 2 was mild and improved with oxygen supply. However, patient No. 3 required chest tube insertion and drainage. Air leakage was persistent although follow-up bronchoscopy showed an intact EBV. The chest tube was removed when the pneumothorax and air leakage resolved approximately 1 month after the procedure. Patient No. 2 experienced slight hemoptysis, but follow-up bronchoscopy showed no endobronchial lesion. He improved after administration of tranexamic acid and antibiotics. There were no other notable adverse events (i.e., acute exacerbation of COPD, pneumonia, readmission, etc.) in the all patients.
DISCUSSION
BLVR with EBV showed efficacy in Asian emphysema patients with noted improvements in pulmonary function, quality of life, and exercise capacity. The clinical efficacy rate was 85.7% (six of seven patients). Safety was also demonstrated with an absence of serious adverse events, although long-term follow-up is needed to confirm safety over the long term. To our knowledge, this is the first report on the use of Zephyr® EBV in BLVR in Asia.
Asian patients with COPD may have characteristics that predispose them to different BLVR outcomes than Western patients. Although tobacco smoking is the major cause of COPD, previous exposure to biomass fuels or dusty jobs, and treated pulmonary tuberculosis are other notable causes of COPD in Asia (14, 15). Especially, the prevalence of pulmonary tuberculosis is as high as 70 in 100,000 in Korea, and previous pulmonary tuberculosis is an important risk factor for Korean patients with COPD (16). Indeed, two of seven patients (Patients No. 5 and No. 7) had past history of pulmonary tuberculosis in our study. Patient No. 5 had focal area of parenchymal distortion in right upper lobe and patient No. 7 had focal fibrosis with linear atelectasis in both upper lobes. However, they did not have any cavitary lesions. Prior pulmonary tuberculosis history did not affect efficacy or adverse events such as pneumothorax. In addition, genetic diseases such as alpha-1 antitrypsin deficiency, which can generate panlobular emphysema, are extremely scarce in Korea. Nonetheless, our results were consistent with those of Western countries.
COPD is thought to be a heterogeneous disease, which has various distinct clinical outcomes despite similarities in airflow limitations (FEV1) (17, 18, 19). A particular COPD phenotype may be related to a distinct natural history and may respond differently to treatment than another phenotype. Identification and targeted treatment of specific phenotypes within the broad spectrum of COPD is important to improve overall treatment outcomes for the disease (20). Emphysema is one representative phenotype of COPD with a distinct pathophysiologic mechanism. However, therapeutic approaches have had limited effectiveness due to a decrease in lung elastic recoil, air entrapment, and hyperinflation associated with emphysema. Although lung volume reduction surgery is a proven palliative procedure for emphysema, the very high operative mortality has limited its use (5).
Several non-surgical lung volume reduction techniques have been developed, including unidirectional valves (EBV and intrabronchial valve) deployment, lung volume reduction coils, biologic lung volume reduction, thermal vapor ablation, and airway tract bypass (21, 22). Among them, EBV deployment has the most abundant clinical data showing its feasibility and safety. EBV clinical trials demonstrated improvement in lung function (FEV1), exercise tolerance (6MWD), and symptoms in patients with advanced heterogeneous emphysema (7, 8). Our study showed better clinical efficacy rate with other clinical trials (7). This is likely due to the appropriate selection of patients and the target lobe in the present study. The right upper lobe was selected preferentially as the target lobe, which may be associated with larger lung volume reductions. Furthermore, we confirmed that the target lobe had no collateral ventilation. Successful BLVR with EBV is dependent on the emphysema distribution and degree of collateral ventilation (6, 23). Complete lobar occlusion by valve insertion provides an effective therapy for patients with severe heterogeneous upper lobe or lower lobe predominant emphysema and little collateral ventilation of emphysema. The use of CT scan is important in selecting patients with heterogeneous emphysema and for identifying fissure integrity. Unlike other studies, we performed pre-procedure dual-energy perfusion CT instead of ventilation-perfusion scintigraphy in all patients to identify the target lobe (11, 24), which was defined as the most hyperinflated and least perfused lobe in our study. In addition to dual-energy perfusion CT, we performed a balloon occlusion test (Chartis® Pulmonary Assessment System) to confirm that the target lobe had no collateral ventilation prior to insertion of the valve. Judicious patient selection using perfusion CT scan and a balloon occlusion test may have led to the excellent outcomes seen in our study.
The exact mechanism by which EBV deployment improves lung function and symptoms is not well understood, but a mismatch between ventilation and perfusion may play an important role. Studies on improvement in ventilation and perfusion, elasticity of the diaphragm, and bronchodilation after EBV deployment have not been performed and may clarify this issue. Furthermore, quantitative assessment with ventilation-perfusion CT scan using xenon before and after procedure may shed further light on the mechanism by which BLVR leads to clinical improvement in emphysema symptoms (25).
Although we noted a high clinical efficacy rate in our study, one patient (No. 4) showed no benefit. We verified that his target lobe had no collateral ventilation on the Chartis® system. However, there was no volume reduction noted on the post-procedure chest radiography. We then removed his pre-existing valves, which had been inserted in his right upper lobe, and placed further valves into his left upper lobe after confirming that the new target lobe was completely fissured and that there was no collateral ventilation using a balloon occlusion test. However, this re-insertion also did not lead to lung volume reduction. These findings suggest there may be very small channel between the lobes, such as the channel of Lambert (26), which cannot be detected by a balloon occlusion test.
BLVR is associated with several complications including pneumothorax, hemoptysis, pneumonia, and acute exacerbation of COPD (7), of which pneumothorax is the most common. In our study, the rate of pneumothorax (28.6%) was too high compared to VENT trial (4.2%) (7). This difference was due to exclusion of patients with collateral ventilation of the target lobe using CT scan and the Chartis® system. Inducing complete atelectasis of target lobe using such pre-tests to increase clinical efficacy would generate more pneumothorax. In our study, one patient (patient No. 3) experienced pneumothorax requiring tube thoracotomy. His clinical outcomes were relatively poorer than those observed in the other patients (ΔFEV1% change, 16.1%; ΔmMRC dyspnea scale, -1; Δ6MWD% change, 25.0%). It is thought that pneumothorax develops when the target lobe collapses and the adjacent lobe inflates abruptly after complete occlusion of the target lobe. There have been no studies on factors that may be predictive of pneumothorax, or measures that may be taken to prevent it. Such studies are warranted to avoid or minimize this complication.
There are some limitations in this study. First, small numbers of subjects were monitored in a short period of time. Some data of patient No. 1 were not available. Additionally, follow up of CT scan was not performed. Long-term follow-up data including changes in quantitative CT measures for more patients would be helpful in determining of clinical efficacy.
BLVR is effective in Asian patients with advanced heterogeneous emphysema, showing noted clinical improvements in lung function and exercise capacity. Judicious patient selection may be important to increase the efficacy and safety of BLVR, regardless of patient ethnicity. We recommend that BLVR with EBV to be considered in other Asian countries.


 XML Download
XML Download