

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary artery disease (CAD) is one of the major predictors of future cardiovascular events (CVEs). Flow-mediated dilation (FMD), which represents endothelial function, reflects not only the presence of CAD but also predicts the risk of CVEs in patients with CAD (1, 2). Brachial-ankle pulse wave velocity (baPWV) is also a predictor of future CVEs for the general population and for patients with CAD (3, 4). In addition, biomarkers such as high-sensitivity C-reactive protein (hsCRP), fibrinogen, homocysteine, and free fatty acid (FFA) correlate well with a future CVE (5, 6, 7, 8, 9). The Framingham risk scoring system has been used to help identify future cardiovascular risk based on a large cohort study (10). However, there are few data on whether the Framingham risk score is still valid for secondary prevention after a diagnosis of stable angina. von Birgelen et al. (11) reported that a positive relationship exists between initial Framingham risk score and future plaque progression in patients with stable coronary artery disease. In addition, the Framingham risk score was a strong predictor of CVEs, including stroke (12). Although the Framingham risk score, FMD, baPWV, and biomarkers (such as hsCRP, fibrinogen, homocysteine, and FFA) could predict future CVEs, a comparison of these risk assessments for future CVEs in patients with stable coronary artery disease has not been reported.
The aim of this study was to assess the inter-relationship between the Framingham risk score, FMD, baPWV, and biomarkers for future CVEs in patients with stable angina.
MATERIALS AND METHODS
Study population, study endpoint, and follow-up
Patients were eligible for enrollment in the study if they were aged between 30 and 75 yr, had stable angina and were scheduled to undergo coronary angiography (CAG). Patients were excluded if they had acute coronary syndrome, significant valvular heart disease (more than a moderate degree), left ventricular dysfunction (left ventricular ejection fraction<55%), an ankle-brachial index<0.9, or an inability to follow the protocol.
The end point of this study was a composite of CVE, including myocardial infarction, de-novo coronary revascularization, in-stent restenosis, stroke, and cardiovascular death. All events were based on clinical diagnoses made by the patient's physician. Clinical follow-up was performed in the office or via telephone at one month, six months, and one year and then annually thereafter.
Before evaluation of the baPWV and FMD, which were evaluated on the morning of the planned CAG, the patients were instructed not to exercise and to discontinue substances that might affect the baPWV and FMD, such as caffeine, food, tobacco, or vasoactive medication, for at least 12 hr before the study. The studies were done in a quiet temperature-controlled room (22℃-24℃). All of the patients had been given clopidogrel (loading dose, if needed) before CAG, because there was a chance that they would need to be undergo percutaneous coronary intervention (PCI).
In this study, significant coronary artery disease (sCAD) was defined as lumen diameter stenosis >50% in one or more major coronary arteries as determined by CAG. The CAG was interpreted by one cardiologist who was blinded to the patients' clinical data. If a patient had sCAD, a decision regarding the treatment option (medical treatment, PCI, or a coronary artery bypass graft operation) was made by the attending physician.
Measurement of FMD
An experienced vascular sonographer who was blinded to the patients' information obtained ultrasound images using a Vivid 7 system (GE Vingmed Ultrasound, Horten, Norway) with a 12-MHz linear array transducer. FMD was measured according to the recommendations of Corretti and colleagues (13). In brief, a landmark 10 cm above the proximal wrist crease of the left radial artery (RA) was used for the vascular ultrasound measurement. After the baseline diameter of the RA was measured, a blood pressure cuff was inflated on the forearm up to 220 mmHg for five minutes and then deflated; after one, two, and three minutes, the RA diameter was measured to obtain the post-occlusion value. All images were recorded digitally by capturing the RA in the longitudinal plane with an electrocardiogram. One cardiologist, who was blinded to the participants' clinical data interpreted the ultrasound results using an off-line method. The maximal RA diameter image for analysis was evaluated during the end diastole in the cardiac cycle (the onset of the R wave on electrocardiography). Measurements were taken at seven points, and the maximal and minimal values were discarded. The mean value from the remaining five measurements was used for further analysis. Thirty randomly selected images were reanalyzed to assess intra-observer variation plotting by two independent measurements; the standard error of the estimate of the intra-observer variability was 5.6%.
Measurement of brachial-ankle pulse wave velocity
The baPWV was measured using a volume-plethysmographic apparatus (VP-2000, Colin Co., Komaki, Japan). Cuffs were connected to both plethysmographic and oscillometric sensors and were placed around both the arms and ankles while the subject remained in the supine position. Electrocardiogram electrodes were placed on both wrists and a microphone to detect heart sounds was placed on the left edge of the sternum to detect the second heart sound. The time interval between the wave front of the brachial waveform and that of the ankle waveform was defined as the time interval between the brachium and ankle (DTba). The distance between sampling points of the baPWV was calculated automatically according to the height of the patient. The path length from the suprasternal notch to the brachium (Lb) was obtained from superficial measurements and was expressed using the following equation: Lb=(0.2195×height of the subject [cm]-2.0734). The path length from the suprasternal notch to the ankle (La) was obtained from superficial measurements and was expressed using the following equation: La=(0.8129×height of the subject [cm]+12.328). Finally, the following equation was used to obtain baPWV: baPWV=([La-Lb]/DTba). In this study, the left side baPWV was used for the analyses.
Age-adjusted Framingham risk score
Although the Framingham risk score has been computed in many different ways since it was first introduced, we used the version described by Wilson et al. (14) that reports the age-adjusted Framingham risk score (AFRS) using categorical variables such as age, sex, blood pressure, total cholesterol, high-density lipoprotein cholesterol, cigarette smoking, and diabetes. This version divides the subject's Framingham risk score by the estimated average risk of the same age and sex group, thus providing the relative risk in the next 10 yr.
Statistical analysis
The continuous variables were summarized as mean±SD. Categorical variables were presented as numbers or percentages. To compare the predictive power of the CVE, a receiver operating characteristic (ROC) analysis was performed, and the area under curve (AUC) was calculated for each variable; the AUCs of the two equations were compared according to the procedure described by DeLong et al. (15). In addition, the Cox proportional hazard analysis was performed to assess independent risk predictors for a CVE. Because the beneficial effects of aspirin and statin have been well proven for patients with coronary artery disease (16, 17), we added these variables on the analysis. As a subgroup analysis, we also performed ROC analysis and Cox proportional hazard analysis for the coronary events of the patients with sCAD. Data were analyzed using standard statistical software (SPSS version 17.0; SPSS Inc., Chicago, IL, USA and MedCalc version 13.0; MedCalc Software, Mariakerke, Belgium). A probability value of <0.05 was considered statistically significant.
RESULTS
Between March 2008 and June 2009, 224 patients with stable angina were assessed for the study. Of these, 21 patients were excluded because of significant valvular heart disease (n=3), LV dysfunction (n=13), and an ankle-brachial index<0.9 (n=5), leaving 203 subjects enrolled in the study. The baseline clinical characteristics and the values of the AFRS, FMD, baPWV, hsCRP, fibrinogen, homocysteine, FFA, and prescribed medications are shown in Table 1. Of the 203 patients, 134 (66%) had sCAD while 69 patients showed mild or intermediate stenosis (non-sCAD; lumen diameter stenosis≤50%) on CAG. Among the 134 patients with sCAD, 82 patients underwent percutaneous coronary intervention. Three patients were treated with coronary artery bypass graft surgery and 49 patients decided to get medical treatment because of relatively less-tight lesions or small vessel disease (<2.5 mm lumen diameter), based on the decision of the attending physician. The duration of mean follow-up was 50±13 months, and 18 patients were lost at follow-up. During the study period, two patients presented with myocardial infarction and were treated with PCI, 19 patients underwent coronary revascularization due to the progression of CAD, eight patients showed in-stent restenosis, and seven patients suffered from stroke; in total, 36 CVEs occurred.
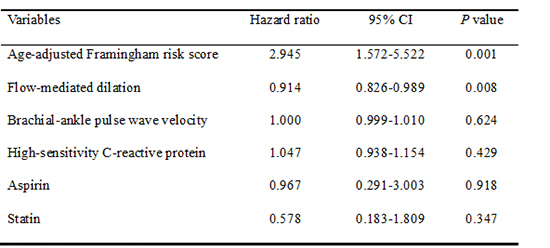
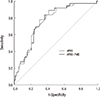
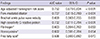
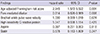
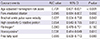
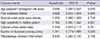
The results of the ROC analysis for CVEs with the AFRS, FMD, baPWV, hsCRP, fibrinogen, homocysteine, and FFA are shown in Table 2. The predictive power of the AFRS was shown to be best and was significantly better than the fibrinogen (z=2.463, P=0.014), homocysteine (z=2.206, P=0.027), and FFA (z=2.288, P=0.022). However, the predictive power of the AFRS was not statistically different from the FMD (z=0.759, P=0.448), baPWV (z=1.794, P=0.073), and hsCRP (z=0.865, P=0.387). Including aspirin and statin, the Cox proportional hazard analysis was performed with the AFRS, FMD, baPWV, and hsCRP which significantly predicted CVEs on the ROC analysis. The AFRS and FMD were independent predictors for CVEs (HR, 2.945; 95% CI, 1.572-5.522, P=0.001 and HR, 0.914; 95% CI, 0.826-0.989, P=0.008, respectively; Table 3). The area under the ROC curves of combined parameters of AFRS plus FMD indicating a future CVE was 0.763 (95% CI, 0.698-0.820; P<0.001). However, there was no difference in the power between combining the AFRS plus FMD and AFRS alone for predicting a CVE (z=1.358, P=0.175; Fig. 1). In the 134 patients with sCAD, we also evaluated for a coronary event, which removed stroke from CVEs. In patients with sCAD, the clinical results may be affected by the lesion characteristics and number of diseased vessels on CAG or by treatment strategy (medical treatment or PCI) (18). According to the ACC/AHA coronary artery lesion classification, 12 patients had type A, 37 patients had type B1, 37 patients had type B2, and 48 patients had type C lesions (19). In terms of the number of diseased vessels, 79 patients had one vessel disease, 33 patients had two and 22 patients had three. During the study period, 19 patients underwent PCI due to progression of CAD, and eight patients showed in-stent restenosis; in total, 27 coronary events occurred. In the 134 patients with sCAD, the ROC analysis for coronary events with the AFRS, FMD, baPWV, hsCRP, fibrinogen, homocysteine, and FFA are shown in Table 4. The predictive power of the AFRS was significantly better than the fibrinogen (z=2.006, P=0.045) and homocysteine (z=2.353, P=0.019). However, the predictive power of the AFRS was not statistically different from the FMD (z=0.505, P=0.613), baPWV (z=1.541, P=0.123), hsCRP (z=1.026, P=0.305), and FFA (z=1.577, P=0.115). In addition to the class of the coronary artery lesion, number of coronary artery disease, and PCI, the Cox proportional hazard analysis was performed with the AFRS, FMD, baPWV, and hsCRP, which significantly predicted coronary events on the ROC analysis. The AFRS was an independent predictor for coronary events and the FMD showed marginal significance (Table 5). The area under the ROC curves of combined parameters of AFRS plus FMD indicating coronary events was 0.736 (95% CI, 0.653-0.808; P<0.001). However, there was no difference in the power between combining the AFRS plus FMD and the AFRS alone for predicting coronary events (0.736 vs. 0.731; z=0.474, P=0.635).
DISCUSSION
The principal finding of this study was that in patients with stable angina, the AFRS and FMD were independent predictors of a CVE. However, FMD could not improve the prediction of a future CVE beyond that offered by the AFRS.
The Framingham risk score is a conventional means of predicting the risk of a CVE in the general population (10). Although the major risk factors are important in primary prevention, there has been limited data about whether the Framingham risk score is still valid for secondary prevention after a diagnosis of stable angina. In this study, the AFRS was the most effective measurement in predicting a future CVE in patients with stable angina. Our results might be supported by a report that a positive linear relationship exists between initial Framingham risk score and future clinical events, with plaque progression measured by serial intravascular ultrasound in patients with stable coronary artery disease (11). In addition, reports indicate that the major risk factors in primary prevention still have crucial value in secondary prevention (20, 21, 22).
It is well known that FMD could offer a noninvasive assessment of preclinical CVE in subjects with and without cardiovascular risk factors (23, 24). In addition, FMD is strongly associated with the presence and extent of CAD, and impaired FMD could independently predict the occurrence of in-stent restenosis after percutaneous coronary intervention (1, 25). In this study, the FMD had good predictive power for a CVE in the ROC analysis, but there was no additional benefit of predicting future CVEs when combining FMD with the AFRS compared to the AFRS alone. Likewise, when the Cox proportional hazard analysis was performed for the 134 patients with sCAD for future coronary events, the AFRS was still an independent predictor and FMD showed marginal significance. However there was no additional benefit of predicting coronary events when comparing FMD plus AFRS to the AFRS alone. A possible explanation was that FMD was closely related to the principal cardiovascular risk factors and the estimated 10-yr risk of CAD in patients with low cardiovascular risk (26). It means that the merit of FMD could be attenuated for future CVE risk assessment as a measurement of secondary prevention, not only in patients with stable angina but also in patients with sCAD.
The baPWV, which is known to be an indicator of arterial stiffness and vascular damage, is a well-known predictor of future CVEs in the general population (3). In addition, the value of baPWV increased in patients with CAD and could be an indepenent predictor of the prognosis of patients with acute coronary syndrome (4, 27). In this study, ROC analysis showed that baPWV could predict a CVE, but there was no difference in power between the AFRS alone and the AFRS plus baPWV (with AUC values of 0.752 and 0.748, respectively; z=0.267, P=0.789). This could be supported by our pervious report that in patients with stable angina the baPWV could predict the presence of sCAD, but there was no additional benefit in predictive power when the baPWV was combined with the Framingham risk score (28).
In many large prospective studies, biomarkers such as CRP, fibrinogen, homocysteine, and FFA have been proposed to enhance current risk score algorithms and be associated with an increased risk of CVE (7, 8, 9, 29, 30). CRP correlates with the risk of cardiovascular disease not only in patients with stable angina but also in those who have never been diagnosed with CAD (5, 6). However, among the biomarkers of the study, the ROC analysis showed that only hsCRP had a significant predictive power for a CVE, but there was no additional value in the power between the AFRS plus hsCRP and the AFRS alone for predicting a CVE (with AUC 0.744 vs. 0.752, z=0.204, P=0.839). In addition, the Cox hazard analysis showed that hsCRP was not an independent predictor of a CVE. In terms of fibrinogen, homocysteine, and FFA, these biomarkers showed marginal significance or non-significance in predicting a CVE in the ROC analysis of the study. The post hoc analysis showed that there was no additional value in adding the above biomarkers to the AFRS compared with the AFRS alone for a CVE. Our results suggest that although these novel surrogate markers are associated with a future CVE, they contribute little to the prediction of a CVE when the conventional risk factors (age, sex, total and high-density lipoprotein cholesterol levels, blood pressure, anti-hypertensive medication use, smoking status, and diabetes) are well considered in patients with stable angina. In addition, this could be explained by several studies that have not shown reclassification in predicting a CVE with the addition of conventional biomarkers compared to conventional risk factors (14, 31, 32). Therefore, it cannot be emphasized enough that precise evaluation and control of the conventional risk factors are most important in the management of patients with stable angina.
There are several potential limitations in our study. First, this study only included patients with stable angina and excluded patients with acute coronary syndrome. Therefore, our results may not be generalized to all patients with coronary heart disease. Second, many of the patients were taking statin or anti-hypertensive medications that may affect the results of FMD. Although the patients were instructed to discontinue vasoactive medications 12 hr before the study, we could not completely exclude the interaction of these drugs. Third, the measurement method for the FMD was rather old and the fixed time interval of measurement was somewhat long (one, two, and three minutes). In addition, we did not use the automated edge detection system that is frequently found in the literature at present (33). However, according to Corretti et al. (13), nearly 70% of the NO is released in the first 60 sec after cuff release, and most maximal dilation occurs around one minute after cuff release. In addition, previous and recent studies have given reliable results using the FMD data measured at 60 sec (34, 35). Fourth, many clinical reports have shown that anti-hypertensive medication and lipid-lowering medication have the beneficial effects of improving endothelial function and change of endothelial function could predict future CVEs (36, 37, 38, 39). However, we did not perform follow-up FMD and cannot describe the relationships between used medications and changes of the endothelial function. Fifth, we selected hsCRP, fibrinogen, homocysteine, and FFA to predict a CVE on the basis of previous clinical studies. However, we acknowledge that other biomarkers that were not included in this study might have resulted in additional information. Finally, the number of patients was relatively small and the duration of follow-up was somewhat short. In addition, a large proportion of events related to coronary revascularization. Therefore, further studies with larger numbers of patients and longer-term follow-up will be needed.
In patients with stable angina, AFRS and FMD are independent predictors of CVEs but the baPWV and biomarkers, such as hsCRP, fibrinogen, homocysteine, and FFA show no significance. However, there is no additive value of FMD on the AFRS in predicting future CVEs.

 XML Download
XML Download