

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Kawasaki disease (KD) is an acute febrile disease with coronary and other systemic vasculitis that occurs predominantly in infancy and early childhood. Although the pathogenesis of KD has not been clearly identified, serum levels of proinflammatory cytokines, such as interleukin (IL)-6 and tumor necrosis factor (TNF)-α, are elevated during the acute phase of KD, suggesting that they may be involved in the development of KD (1).
White adipose tissue which used to be simply known as a storage of surplus energy is now perceived as an independent and active endocrine organ. It produces various kinds of adipokines such as leptin, adiponectin and resistin, which have major effects on obesity related metabolic disease by controlling fat metabolism, energy homeostasis and insulin sensitivity. Moreover, adipokines participate in the systemic inflammatory response with strong reciprocal influences on other cytokines such as TNF-α, IL-6 and IL-10, and in regulating the systemic inflammatory response, angiogenesis, and subclinical atherosclerosis (2).
Recent studies have reported that circulating adiponectin levels in patients with acute KD were significantly lower than that in convalescent KD patients and controls (3). The role of hypoadiponectinemia or hyperadiponectinemia on the degree of severity of KD remains controversial. Also, previous reports have shown that the serum resistin levels were elevated in KD children than healthy children, but its concentrations were unlikely to help predict the prognosis of disease in acute KD patients (4). There have been contrasting reports on the potential role of leptin in the pathogenesis of KD. Some published studies have suggested that leptin participates in the systemic inflammatory response (5), and increased leptin concentration is an independent risk factor for coronary heart disease (6). In contrast, Liu et al. (7) reported that serum leptin levels in patients with KD were lower than those in healthy controls, which suggests that leptin is not involved in the generalized inflammation seen in KD patients. Taking this evidence into consideration, we hypothesized that adipokines might exert direct or indirect effects on the progression of KD, and that they may be predictive factors for development of coronary artery lesions (CAL). Therefore, we compared the sereial levels of adipokines, IL-6, and TNF-α in KD patients and control groups to assess whether an association is present between circulating adipokine levels and CAL in KD patients.
MATERIALS AND METHODS
Patients and data collection
The study included 40 Korean children with KD and 47 age-matched children recruited between May and November 2013. The 40 KD patients were enrolled within 8 days of the onset of illness, with day 1 defined as the first day of fever symptoms. The control groups consisted of 47 subjects (32 febrile patients and 15 afebrile patients) with a mean body mass index (BMI) of 16.15±1.82 kg/m2. The febrile control patients had either pneumonia, acute tonsillitis, or acute cervical lymphadenitis. The afebrile control patients had acute gastroenteritis, acute urticaria, or Henoch-Schonlein purpura.
Echocardiography
Echocardiography was performed within 8 days of the onset of fever or before intravenous immunoglobulin (IVIG) administration. CALs were diagnosed on the basis of the Z scores of the left main coronary artery, proximal left anterior descending coronary artery, and proximal right coronary artery, and were defined as the Z scores of 2.0 or more. The value of Z scores from a standardized coronary artery dimension was calculated from the body surface area (8) based on formula of Haycock's et al. (9).
Laboratory analysis
Levels of leptin, adiponectin and resistin were measured in 87 cases, including groups: KD patients with normal coronary arteries (n=28), KD patients with dilated coronary arteries (n=12), the acute febrile control group (n=32), and the afebrile control group (n=15). The serum levels of leptin, adiponectin, resistin, IL-6, and TNF-α were assayed with an enzyme-linked immunosorbent assay (ELISA) kit (abcamR, R&D Systems, Cambridge, United Kingdom). White blood cells counts (WBC), hemoglobin, hematocrit, platelet count, alanine aminotransferase (ALT), aspartate aminotransferase (AST), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and lipid panels were obtained in all study subjects; blood samples were drawn before IVIG therapy in KD patients.
Serial blood samples were obtained from all KD patients in the acute stage, 2-4 days after IVIG infusion, and in the convalescent phase, when ESR was normal (on days 30-35). Samples were prepared at the appropriate dilutions and paired samples were assayed together according to the instructions of the manufacturers.
Statistical analysis
Normally distributed continuous data were expressed as mean±standard deviation. Comparisons of the frequencies between groups were analyzed using chi-square tests. Differences among groups were assessed using the unpaired 2-tailed t-tests and analysis of variance (ANOVA). The significance of difference was calculated by Scheffe's test, and a P value less than 0.05 was considered as statistically significant.
RESULTS
Baseline patient characteristics and laboratory findings
The KD group included 25 boys and 15 girls with a mean age at diagnosis of 35.18±22.09 months with a range from 5 months to 8 yr. Of the 40 KD patients, 33 patients (82.5%) were diagnosed with typical KD and 7 patients (17.5%) with incomplete KD. The mean time until start of IVIG treatment was 5.43±1.19 days. The mean age of the control groups was 34.41±21.09 months and 41.07±22.80 months in febrile and afebrile control groups, respectively.
The mean intervals of blood sampling day from the onset of illness before and after IVIG therapy in the KD patients were 5.43±1.19 and 8.00±1.60 days, respectively.
Two patients resisted the initial IVIG treatment, but responded to the second IVIG treatment.
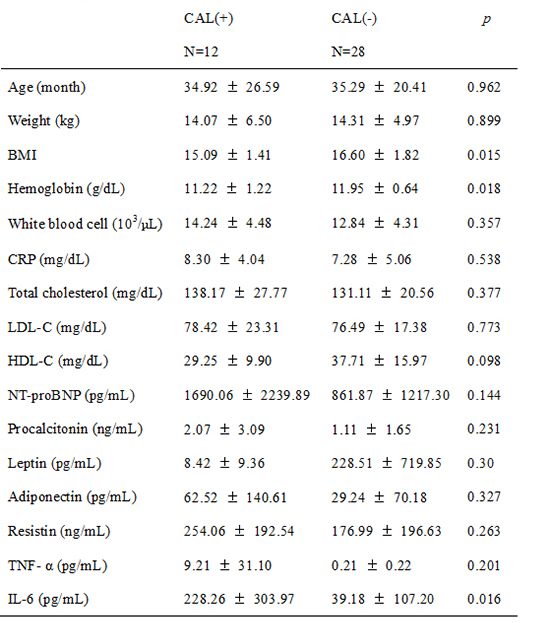
At admission, the levels of WBC, neutrophil count, ALT, ESR, CRP, and N-terminal fragment of B-type natriuretic peptide (NT-proBNP) were significantly higher in KD patients compared with the control groups. The level of HDL-C was lower in KD patients compared with the control groups (P=0.008 in febrile controls, P=0.004 in afebrile controls) (Table 1).
Levels of TNF-α, IL-6, adipokines and other parameters in KD patients
The serum resistin levels at baseline in KD children were significantly higher than those in the febrile controls (177.56 ng/mL [3.12-546.83] vs. 76.48 ng/mL [0.17-257.6], P=0.024). There were no significant differences between groups of KD with and without CALs in age, gender, ALT, AST, CRP, and NT-proBNP levels. However, serum IL-6 levels were significantly higher and hemoglobin levels were significantly lower in the KD group with CALs than those without CALs (P=0.016 and P=0.018, respectively). There were no significant differences in serum leptin, resistin, adiponectin, and TNF-α levels between groups of KD with and without CALs (Table 2).
Echocardiographic findings
Twelve of the 40 patients (30.0%) showed dilation of coronary arteries in the acute stage of KD. All of the KD patients with CALs at admission showed normal coronary arteries at 1 month after discharge. None of the KD patients developed coronary artery aneurysms as evaluated by echocardiography before and after IVIG therapy. There was no difference between the KD patients and the febrile control patients in the degree of left ventricular fractional shortening. The ratio of mitral peak velocity of early filling to early diastolic mitral annular velocity measured by tissue Doppler imaging (TDI) was increased in the acute KD group compared with the febrile control group, which did not reach a statistical significance (Table 3).
Correlations between adipokines and other parameters
Hemoglobin and IL-6 levels were significantly correlated with resistin levels in patients with KD (r=-0.318, P=0.027; r=0.431, P=0.014, respectively). Age in KD patients was negatively associated with adiponectin levels (r=-0.354, P=0.027). In addition, BMI was positively associated with leptin levels in KD (r=0.502, P=0.001). A positive correlation was found between leptin and adiponectin levels before IVIG treatment in acute stage of KD (r=0.501, P=0.001) (Table 4). In febrile controls, resistin concentrations were significantly associated with elevated WBC counts (P=0.002) and CRP levels (P=0.021).
Serial changes in serum levels of adipokines, IL-6 and TNF-α in KD patients
Fig. 1 and Fig. 2 show the changes in serum adipokines, IL-6, and TNF-α levels between the acute stage (before IVIG therapy), 2-4 days after IVIG treatment, and the convalescent phase. The serum adiponectin levels were increased immediately after IVIG therapy but were decreased to baseline levels in the convalescent phase. IL-6 and TNF-α levels peaked at 5.43±1.19 days and 8.0±1.60 days from onset of illness, respectively.
After IVIG therapy, serum resistin levels significantly decreased (177.56 ng/mL before IVIG therapy vs. 63.37 ng/mL at 48 hr after IVIG infusion, P<0.01) (Fig. 1). Serum IL-6 levels significantly decreased from 141.65 pg/mL to 1.91 pg/mL after IVIG treatment (P<0.01) (Fig. 2). The levels of TNF-α continued to increase after IVIG treatment during hospitalization (4.86±22.0 pg/mL at baseline vs. 19.13±61.82 pg/mL at 48 hr after IVIG therapy, P=0.281), but did not reach a statistical significance.
DISCUSSION
This study was conducted to determine the role of adipokines in the pathogenesis of Kawasaki disease (KD) and to investigate the association between adipokines and coronary artery complication. Only resistin was significantly elevated in KD patients among three adipokines (leptin, adiponectin and resistin), although its concentration could not predict coronary artery dilatation in the acute stage.
KD is an acute febrile vasculitis of unknown origin. Activated monocytes and macrophages have a pivotal role in KD and are indeed found in the vessel walls of KD patients (1). During the acute phase of KD, certain unidentified agents activate monocyte, T cell and B cell, and up-regulate proinflammatory cytokines such as IL-1, IL-2, IL-6, and TNF-α.
Adipokines are an important group of inflammation-related molecules that play roles in the immune system and inflammation. Adipokines can be subdivided into those inducing mainly pro-inflammatory (leptin, resistin, IL-6, TNF-α) and anti-inflammatory effects such as adiponectin and IL-10 (10). Our study showed that serum leptin levels in patients with KD were higher than that of febrile and afebrile controls but the difference was not statistically significant. Leptin is produced by inflammatory cells, and leptin mRNA expression and circulatory leptin levels are increased by a number of inflammatory stimuli, including IL-1, IL-6 and lipopolysaccharide (11). A previous study reported that high leptin levels are predictive of poor vascular compliance in adolescents. In these healthy adolescents, leptin was a better predictor of vascular compliance than the traditional risk factors, such as fasting insulin and CRP (12). In our study, no significant difference in leptin level was observed between the KD patients with and without CALs.
Adiponectin has been suggested to be involved in glucose metabolism and insulin sensitization. It promotes the phagocytosis of apoptotic cells, since the accumulation of apoptotic debris can cause inflammation and immune system dysfunction (13). Moreover, the secretion of adiponectin is inhibited by proinflammatory cytokines such as IL-6 and TNF-α (14). In our study, the adiponectin levels were negatively correlated with IL-6 and TNF-α, which did not reach statistical significance. In addition, adiponectin in KD patients was negatively associated with age, which means that younger patients with KD have higher level of adiponectin.
Ouchi et al. (15) reported that physiological concentrations of adiponectin (5-25 µg/mL) had significant inhibitory effects on TNF-α-induced monocyte adhesion and adhesion molecule expression in a dose-dependent manner in vitro. In our study, adiponectin levels were higher in the acute stage of KD patients with CAL than those without CAL, but the difference did not reach a statistical significance. In contrast, low adiponectin levels have been observed in patients with coronary artery disease (16, 17). It might be because of relatively different age groups in the subjects of the study. The pathophysiology of coronary artery disease in adults is different from that of CALs of KD in children. Moreover, only low molecular weight adiponectin displays anti-inflammatory properties and high molecular weight adiponectin has proinflammatory effects (18). Therefore, analysis of specific adiponectin isoforms may be necessary to prove these diverse effects.
In humans, resistin is mainly expressed in monocytes, macrophages, spleen and bone marrow-derived cells and also at very low levels in adipose cells (19). In our study, serum resistin levels were significantly higher in the acute stage KD patients than the control groups. However, its concentrations were not significantly different between KD patients with and without CALs. Elevated serum resistin has been reported in patients with chronic inflammatory disease such as rheumatoid arthritis (20), inflammatory bowel disease (21), and asthma (22). In our study, hemoglobin levels were negatively correlated with resistin levels in patients with KD. Moreover, serum hemoglobin levels in the KD patients with CALs were significantly lower compared with the KD patients without CALs. This result is in line with previous observation that anemia in KD occurs in patients exhibiting more severe inflammation. Further studies will be necessary to confirm the pathogenic mechanisms causing the elevation of resistin levels in anemic KD patients.
The present study showed that the serum IL-6 levels were significantly higher in group of KD with CALs than those without CALs, which may be useful to predict CAL and IVIG resistance in KD. IL-6 is a multifunctional cytokine, which promotes inflammation in damaged organ tissue by giving rise to the secretion of other inflammatory cytokines (23). Lin et al. (24) showed that serum IL-6 and IL-8 were highest during the first week of KD and decreased progressively thereafter, and that serum TNF-α increased in the first week and continued to increase in the second week. These serial changes correlated with the results of our study. Interestingly, BMI was significantly lower in the KD group with CALs than those without CALs in our study. Although there has been no report of the association between the severity of KD and BMI, it may be due to the relatively younger age in KD group with CALs than in those without CALs.
This study has some limitations. First, the number of subjects was relatively small. Second, there were no coronary aneurysms as a sequela in KD group. Lastly, the synthesis of leptin is mainly regulated by food intake and the production of adiponectin is down regulated when the uptake of free fatty acid is reduced, such as in the fasting state (25). Therefore, the control of fasting time before blood sampling will be necessary in the future study.
In conclusion, the serum levels of resistin were elevated significantly in the acute stage of KD patients. However, there were no significant differences in serum leptin, resistin, adiponectin, and TNF-α levels between KD patients with and without CALs. Multicenter, randomized clinical trials should be conducted to determine the role of adipocytokines in the pathogenesis of KD vasculitis.



 XML Download
XML Download