

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In 2000, more than a quarter of the world's adult population, totaling nearly 1 billion, had hypertension; and this proportion will increase to 29% (1.6 billion) by 2025 (1). High blood pressure (BP) is responsible 7.6 million premature deaths and 92 million disability-adjusted life years (DALYs) in 2001 (2). In addition, BP change is a common condition that elevates the risk of cardiovascular disease (CVD) and mortality in several studies (3, 4, 5, 6).
Serum γ-glutamyltransferase (GGT), a commonly used alcohol consumption or liver disease, was an established risk factor for CVD, such as stroke, myocardial infarction, congestive heart failure, metabolic syndrome, and coronary heart disease, suggesting that GGT may be a predictor of CVD (7, 8, 9). GGT is also a significant risk factor for increase BP (10, 11, 12, 13) and incident hypertension (14, 15, 16, 17, 18, 19). It is well reported that several cardiovascular risk factors influences differently according to gender (20). Some studies showed that considerable underlying differences in the distributions of GGT by gender (21, 22). However, the difference of the association between GGT and BP by gender is unclear. Some previous study has suggested no gender differences in risk of hypertension (18) while other has shown a different risk in women than in men (12). Moreover most previous studies have not been explored gender differences of these associations (10, 11, 13, 14, 15, 16, 17, 19).
Therefore, we investigated the association between GGT at baseline and BP and 4-yr change in BP in a large population and assessed whether gender-related difference in this association.
MATERIALS AND METHODS
Study subjects
As a part of the Korean Genome Epidemiology Study, the Ansung-Ansan cohort study is an ongoing community-based prospective cohort of 10,038 participants aged 40 to 69 yr. The initial enrollment was carried out in 2001-2002 and follow-up examinations are conducted biennially. The details of the study design and procedures have been previously described (23). The current study was based on an examination of baseline and second follow-up data. A total of 7,260 subjects was enrolled in the current study after the 4-yr follow-up examination; 2,492 subjects declined to participate in the follow-up surveys and 286 died before completing the 2 follow-up visits.
For accurate observation of association between GGT and BP change, 3,067 individuals with hypertension at baseline (BP ≥ 140/90 or use of antihypertensive medications) were excluded. In addition, 168 participations with missing information on GGT, systolic blood pressure (SBP), diastolic blood pressure (DBP), body mass index (BMI), alcohol intake and smoking status at baseline and SBP and DBP in the 2 follow-up visits were excluded. The remaining 4,025 participants (1,945 men and 2,080 women) are included in this analysis.
Data collection
Height and weight were measured using standardized techniques and equipment. The BMI was calculated as weight (kg) divided by height squared (m2). BP while the subject was sitting and had rested for at least five minutes was measured on 2 occasions 5 min apart using a standard mercury sphygmomanometer (Baumanometer; W. A. Baum, Copiague, NY, USA) by trained staff; and the mean of value was used for this study. At baseline examination, hypertension was defined as BP ≥ 140/90 or use of antihypertensive medications. Blood sample were obtained after a fasting at least 12 hr; serum GGT, triglycerides, high-density lipoprotein (HDL)-cholesterol and C-reactive protein (CRP) were quantified by biochemical assays, performed by a central laboratory (Seoul Clinical Laboratories, Seoul, Korea).
Demographic characteristic was collected at baseline by trained interviewers; age, gender, cigarette smoking status, alcohol consumption (grams/day), menopausal status (yes/no), and medication (yes/no). Non-smokers were defined as those who had reported "never smoking" in the questionnaire. Former smokers were defined as those who had reported "abstain from smoking" in the questionnaire. Current smokers were defined as those who had reported "currently smoking" in the questionnaire. Alcohol consumption determined based on self-report. Subjects were asked how often, on the average, they had consumed the specified amount of each item over the past year. Then, alcohol consumption in grams per day was calculated as the sum of the average alcohol content per type of alcoholic beverage intake multiplied by the daily number of drinks. Menopausal status was also assessed by the self-report. Subjects who answered "yes" to the following question: "Do you menstruate?" were allotted to premenopausal, and "no" to the question were allotted to postmenopausal.
Statistical analysis
Variables with skewed distribution were log-transformed before analysis. Descriptive statistics used to characterize the study subjects included means and SDs for continuous variables and proportions for categorical variables. Comparison between men and women were done with t-test or with the chi-square test. Correlations were evaluated with Pearson correlation coefficient.
Linear regression models were used to examine the associations of GGT and BP and 4-yr change in BP. We used 3 models. First, we performed unadjusted analysis. Second, we adjusted for baseline levels of age, BMI, HDL-cholesterol, triglyceride, CRP and SBP. Finally, we further adjusted for baseline levels of smoking status and alcohol intake.
Finally we evaluated the association of GGT and BP and 4-yr change in BP for subgroups defined by gender, age, menopausal status. All reported P values are two-sided, and P<0.05 was considered statistically significant. Analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC, USA).
RESULTS
Participant characteristics in men and women
Table 1 presents study population characteristics at baseline for men and women. The mean age of study population was 49.9 yr in men and 50.1 yr in women at baseline. The BP, triglyceride, CRP, GGT levels, and alcohol intake were significantly higher in men than in women. Proportions of current smokers were 48.1% in men and 3.1% in women.
Associations between baseline GGT and baseline BP
Unadjusted analyses showed that GGT was positively associated with SBP both in men and in women (P<0.001, respectively), and regression coefficient is higher in women than in men. Also, this relationship remained significant after adjusting for age, BMI, HDL-cholesterol, triglyceride, CRP, smoking status, and alcohol intake in all subjects (β=1.28, P<0.001). There was no significant gender difference in the association between baseline GGT and baseline SBP (P for interaction with gender=0.829). DBP also showed significant association with GGT even after adjusting covariates mentioned above (P<0.05). GGT was not associated with SBP in any age group in men or in women. However, DBP showed significant association with GGT even after adjusting covariates in men younger age group (β=0.77, P=0.037). In the menopausal status-stratified association between GGT and BP after adjusted covariates, GGT was not associated with BP in pre- and post-menopause, either.
Association between baseline GGT and change in BP
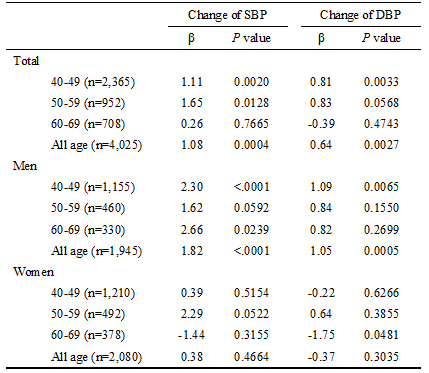
Table 2 showed relationship between GGT at baseline and 4-yr change in SBP. Remarkably, after adjusting for age, BMI, HDL-cholesterol, triglyceride, CRP, smoking status, alcohol intake, and SBP at baseline, GGT was still positively associated with change in SBP in men with statistical significance (P<0.001), but not in women. DBP change also showed significant association with GGT even after adjusting covariates mentioned above (P=0.003) (Table 3). There was significant gender difference in this association (P for interaction with gender=0.007). Furthermore, the gender difference still remained significant after adjusting body weight change during 4 yr (Supplemental Table 1). Also, these results still remained constant even when heavy drinkers or documented hepatitis patients were excluded (Table 4).
The age-stratified association between GGT and change in SBP is presented Table 2. In unadjusted model, men showed significantly positive association in the age groups 40-49 yr and 50-59 yr, and also positive associating tendency in the age groups 60-69 yr with marginal significance (P=0.097). After adjusting covariates, men still showed significantly positive association in the age groups 40-49 yr and 60-69 yr and also positive associating tendency in the age groups 50-59 yr with marginal significance (P=0.060). DBP change also showed significant association with GGT in age group of 40-49 yr. However, GGT in women was not associated with change in BP in any age group. Women showed significantly inverse association in the age group 60-69 yr (β=-1.75, P=0.048).
There was significant age difference in this association in women (P for interaction with age=0.021), but not in men (P for interaction with age=0.476). In the menopausal status-stratified association between GGT and change in BP after adjusted covariates, GGT was not associated with BP in premenopause, postmenopause or change from premenopause to postmenopause, either.
DISCUSSION
This study showed gender differences in the relation of baseline serum GGT levels to BP change in 4 yr. GGT levels were associated with BP at baseline after adjusting for age, BMI, HDL-cholesterol, triglyceride, CRP, current smoking status and alcohol intake. However, baseline GGT levels were significantly associated with BP change only in men not in women. This suggests that the effect of GGT on BP changes may be somewhat different between men and women.
Previous studies have shown that GGT has been used as a simple marker of alcohol consumption (24) or liver dysfunction (25). Recent studies have demonstrated that baseline GGT is known as the major risk factor for development of CVD, diabetes, after adjusting for alcohol consumption (7, 16).
Several previous cross-sectional and longitudinal studies have also reported a positive association of GGT with BP and hypertension (10, 11, 12, 13, 14, 15, 16, 17, 18, 19). However, results of these studies on the difference in the association between men and women did not entirely consistent. Nilssen and Forde reported a positive association between GGT and BP only in women, but not in men (12), but Shankar and Li found no significant gender difference in the association between GGT and BP (18). Others had not studied separately in men and women but in only men (11, 13, 17) or pooled together (10, 14, 15, 16, 19). In this study, GGT levels were associated with BP at baseline after adjusting for age, BMI, HDL-cholesterol, triglyceride, CRP, current smoking status and alcohol intake in overall population, whereas the statistical significance was lost after dividing overall population into men and women. That might be result from the reduced sample size and overcorrection.
Our study also showed that there was significant age difference in the association of GGT with BP changes in men and women. Namely, in men, there were positive associations between GGT and change in SBP among those with age groups 40-49, 50-59 (borderline significant) and 60-69 yr, but, in women, only age group 50-59 yr (borderline significant). Generally, aging process is associated with a progressive stiffening arterial structure, and this process induces a rise in BP (26). In men, our study showed that the association of GGT with SBP change was stronger in old age groups. Lee et al. showed that clarified the complex interaction between GGT, BP and age in men. The study demonstrated that the relations of GGT with BP altered by age. There were positive associations between GGT and change in BP in at or greater than 35 yr old, but in less than 35 yr old (27). However, the study was made up in men aged 25 to 50 yr, so it seems unreasonable to compare our study. In women, considering that on average, natural menopause occurs between the ages of 42 and 50 yr in Asian populations (28), the association of GGT and BP change in women aged 50 to 59 yr may be explained change in menopausal status. So, when subdivide by menopausal status, we showed the strong positive association in change from premenopause to postmenopause, but it was not statistically significant.
In this report, we could not offer the clear mechanism of gender difference in the association between GGT and the BP. However, we evaluated the association between GGT and other risk factors in men and women (Table 5). The association between GGT and BP in men still remained significant after adjusting BMI and HDL-cholesterol, whereas is no more significant in women after adjusting BMI. That finding suggests GGT in men might be influenced thus reflects other stress condition such as oxidative stress.
Although the mechanism of the association between GGT and BP remains not fully understood, substantial evidence supports the biological plausibility of this finding, including an indirect role of GGT in initiating extracellular catabolism of antioxidant glutathione in response to oxidative stress (29). So, GGT might be a sensitive marker for oxidative stress (30). An experimental study found that oxidative stress have been found with higher levels in men (31), the result has been described that testosterone increases whereas estrogen inhibits total body oxidative stress (32, 33). In particular, the antioxidant activity of an estrogen depends on scavenging free radicals decrease reactive oxygen species (32, 34). Longitudinal cohort study and cross-sectional study also showed an association between menopause and BP and change of BP (35, 36). Therefore, a positive association of GGT with change in BP may be explained in considering the decreasing estrogen by transition from the pre- to the postmenopausal. Also previous report suggested the association of GGT and prehypertension incidence (37).
Major strengths of this study are the large prospective design, the length of follow-up, and the standardized protocol. Additionally, information on all major risk factors was collected. However, it has also potential limitations. First, GGT was only measured at baseline. Therefore, we were unable to examine for the effect change in GGT on BP. Second, the age-related increase in BP becomes steeper after the 40 yr old (26), however our study was conducted subjects aged 40-69 yr. And four years' follow up duration might still be too short in confirming gender difference in GGT levels and BP change. Finally, we did not consider the differences in natural and surgical menopause.
In conclusion, the most important findings of this study are the gender differences in the association between GGT and the change of BP. The definitive reasons for this gender difference remain unclear, and require further investigation.


 XML Download
XML Download