

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Warfarin is the most widely used anticoagulant agent for the prevention of stroke or systemic thromboembolism in patients with atrial fibrillation. However, warfarin has a narrow therapeutic range of international normalized ratio (INR) and is known to have multiple interactions with drugs, food, and herb.
There is some difficulty in deciding a starting dosage of warfarin, because of the large interindividual variation in the dose needed to reach adequate level of INR. The warfarin dose can be affected by several factors including dietary, demographic factors, drugs and, several pathophysiological conditions (1). Genetic factors also play a relevant role in the individual variability of the warfarin dose. In particular, several single nucleotide polymorphisms of the cytochrome P450 (CYP), subfamily IIC, polypeptide 9 (CYP2C9) and vitamin K epoxide reductase (VKORC1) genes can significantly influence the warfarin dose requirement (2).
Clinical factors, such as thyrotoxicosis, can either strengthen or reduce warfarin action. Several coagulation and fibrinolytic parameters appear to be affected by thyroid hormone excess (3).
We report a patient with atrial fibrillation in whom the concomitant presence of rare genetic abnormality and thyrotoxicosis caused a marked increase in the INR level at the beginning of warfarin therapy.
CASE DESCRIPTION
A 73-yr-old Korean male with permanent atrial fibrillation visited outpatient clinic for the management of atrial fibrillation on Feb. 21, 2012. He had a history of hypertension and colon cancer with liver metastasis. At the age of 68, he had undergone extended right hemicolectomy with liver tumorectomy due to colon cancer with liver metastasis and received adjuvant chemotherapy for two years. After chemotherapy, he had no evidence of tumor recurrence.
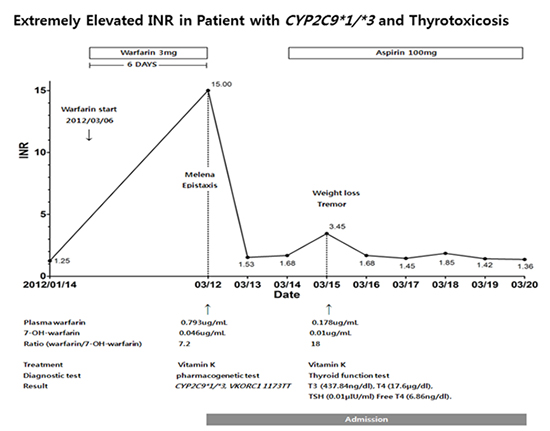
His current medication included diltiazem (90 mg/day) and aspirin (100 mg/day), spironolactone (25 mg/day), hydrochlorothiazide (12.5 mg/day). Considering his risk for stroke and systemic thromboembolism (CHA2DS2-VASc score 2), oral anticoagulation was recommended for him. He began to take warfarin 3 mg daily since March 6, 2012. When he revisited the outpatient clinic after six days, his INR was significantly increased to 15 (Fig. 1). He had recently experienced epistaxis and melena. He was admitted for correction of high INR and bleeding tendency on March 12, 2012. His liver function test at the time of admission was normal and he had no short bowel syndrome which would affect drug absorption. He denied any drug, alcohol, or herbal intake, which may affect INR level.
We also performed a pharmacogenetic test on him to identify genetic susceptibility to warfarin effect. Genomic DNA was extracted from peripheral blood leukocytes using DNA extract all lysis reagents (Applied Biosystems, CA, USA). Genotyping for polymorphisms of CYP2C9 (rs1057910, CYP2C9*3) and VKORC1 (rs9934438, 1173C>T) variants was performed using TaqMan® Drug Metabolism Genotyping Assays and 7500 Fast Real-time PCR system (Applied Biosystems, CA, USA). Later, he was found to be an intermediate metabolizer with genotype of CYP2C9*1/*3 and had VKORC1+1173TT genotype indicating high warfarin sensitivity (Fig. 1).
Upon admission, warfarin was discontinued and 10 mg of Vitamin K was injected 2 times. Then on hospital day (HD) 3, aspirin 100 mg a day was started to replace warfarin. But his INR was increased to 3.45 again on the same day (Fig. 1).
We measured his plasma warfarin and 7-hydroxy-warfarin concentrations by high-performance liquid chromatography tandem mass spectrometry on HD 0 as a baseline and HD 3. On HD 0, total plasma warfarin, 7-hydroxy-warfarin concentration (7-OH-warfarin), and the ratio of warfarin/7-OH-warfarin were 0.793 µg/mL (therapeutic range 0.5 to 3.0 µg/mL), 0.046 µg/mL, and 7.2, respectively. On HD 3, total plasma warfarin and 7-OH-warfarin levels were decreased to 0.178 µg/mL and 0.01 µg/mL, respectively, and the ratio of warfarin/7-OH-warfarin was increased to 18 (Fig. 1).
On thorough history taking, he complained of hand tremor with proximal muscle weakness. He also experienced unexplained body weight loss before admission. From this information, we suspected hyperthyroidism and thyroid function test was performed on HD 3 to confirm the diagnosis. Total T3, total T4, TSH, and free T4 were 437.84 ng/dL (normal range 60 to 181 ng/dL), 17.6 µg/dL (normal range 3.2 to 12.6 µg/dL), 0.01 µIU/mL (normal range 0.64 to 6.27 µIU/mL), and 6.86 ng/dL (normal range 0.89 to 1.8 ng/dL), respectively. The results were consistent with hyperthyroidism, so carbimazole (20 mg twice daily) and betaxolol (20 mg twice daily) were started. The patient was discharged from the hospital on HD 8. His INR was 1.36 at the time of discharge (Fig. 1). After discharge, warfarin was discontinued due to the risk of bleeding and instead aspirin was maintained for atrial fibrillation.
DISCUSSION
We have observed a rare case with genotype of CYP2C9*1/*3 and concomitant hyperthyroidism in which the usual initiation of warfarin therapy caused a dangerous and unexpected elevation of the INR value and led to bleeding complication. CYP2C9 is a liver enzyme required for the oxidative metabolism of a large number of clinically important drugs, including warfarin. Three alleles, CYP2C9*1, *2, and *3 are present in most ethnic populations. Both CYP2C9*2 and *3, and only in carriers of at least 1 copy of CYP2C9*3 confer significantly higher risk for warfarin over-anticoagulation and hemorrhagic complications compared to wild type allele (4).
The frequency of CYP2C9 and VKORC1 1173 C/T polymorphism is largely dependent on ethnicity. In a Korean population study, the allele frequencies of CYP2C9*3 and CYP2C9*1 are reported to be 6% and 93.4%, respectively. But CYP2C9*2 allele has not been detected. The frequencies of CYP2C9*1/*3* and 1/*1 genotypes are 12% and 86.9%, respectively (5). VKORC1+1173TT genotype associated with high warfarin sensitivity predominates in Asian population than in non-Asian population (6).
It has been reported that overt hyperthyroidism exerts a procoagulant effect and increases the risk of thromboembolic events (5). In contrast, thyrotoxicosis has been associated with an increased sensitivity to warfarin, irrespective of the nature of the underlying thyroid disease (6). Several studies reported warfarin-induced hypoprothrombinemia in hyperthyroidism with an increased risk of bleeding (7, 8, 9, 10). In thyrotoxic patients, warfarin produced a greater fall in factors (II and VII) and a greater increase in prothrombin time than in the euthyroid state (11). Furthermore in thyrotoxicosis, the degradation rate of coagulation factors is increased, resulting in their higher plasma clearance and shorter plasma half-life (6).
We are presenting a very rare case about a patient with an uncommon genetic susceptibility to warfarin effect and co-existing hyperthyroidism at the beginning of warfarin treatment. From this case, we learned the clinical usefulness of pharmacogenetic and thyroid function tests in patients with atrial fibrillation, in whom warfarin is considered to prevent stroke or systemic thromboembolism.

 XML Download
XML Download