

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The purpose of prophylactic antibiotic use is to prevent local or systemic postprocedural infection. Two types of infection dominate urologic surgery: 1, urinary tract infection (UTI), which is either a space or organ infection associated with both endoscopic and endoluminal interventions and with both open or laparoscopic surgery, mostly coinciding with catheter and stent placement or an undetected harbored bacterial load; and 2, wound infection after open and laparoscopic surgery. A third form of infection is observed in the male genital system (prostatitis, epididymitis, and orchitis). A fourth form of infection, bloodstream-borne sepsis secondary to urologic instrumentation, accounts for 10% to 12% of healthcare-associated infections in urology wards (1). However, the use of antibiotics in urologic surgery has been controversial for decades (2, 3). During the previous decade, much progress in prostate surgery has been made (e.g., transurethral surgery, open and laparoscopic prostatectomy); however, controversy over antibiotic prophylaxis for prostatic surgery remains.
In the context of surgical field classification, transurethral resection of the prostate (TURP) can be categorized into a clean-contaminated or contaminated operation depending on the patient's history of UTI/urogenital infection, catheterization, and sterile/nonsterile urine (4). This classification may extend to total or laparoscopic radical prostatectomy because during surgery, opening of the urogenital tract is inevitable and Foley catheterization is mandatory after the procedure (5). In this regard, the administration of prophylactic antibiotics is suitable for prevention of postoperative infectious complications. Unfortunately, however, studies of the prophylactic effect of antimicrobial therapy and risk factors associated with TURP and other prostate interventions (e.g., adenoma enucleation, laser ablation) have been limited (6, 7, 8, 9). In addition, there are few retrospective or prospective cohort studies of the prophylactic antibiotic effectiveness in total or radical prostatectomy (10, 11, 12). These studies focused only on surgical site infection, not UTI, and did not include risk factor assessment. As mentioned previously, in cases of prostatectomy, the urinary tract is opened during the procedure; thus, postoperative bacteriuria is probably the main source of postoperative infectious complications (13). Therefore, it is reasonable to identify the risk factors for postoperative bacteriuria or infectious complications and the effectiveness of prophylactic antimicrobial therapy for prostate surgery.
There is currently a lack of information on the risk factors for infectious complications associated with prostate surgery in Korea. In addition, the Health Insurance Review & Assessment Service of Korea recently recommended the use of first- or second-generation instead of third-generation cephalosporins for prophylactic antibiotics in patients undergoing prostate surgery without any Korean evidence. Therefore, we evaluated the risk factors for infectious complications after transurethral surgery of the prostate and after open or laparoscopic prostate surgery as well as the efficacy of antibiotic prophylaxis.
MATERIALS AND METHODS
Study population
From January 2012 to June 2013, we evaluated a total of 424 patients with symptomatic benign prostatic hyperplasia or prostate cancer who underwent TURP, holmium laser enucleation of the prostate, photovaporization of the prostate (GreenLight laser; American Medical Systems, Minnetonka, MN, USA), or prostatectomy at multiple institutions in Korea. Inclusion criteria were as follows: patients who received initial intravenous antibiotics 30 to 60 min before prostate related surgery, patients who underwent urinalysis and urine culture by collection of a midstream urine sample on 3 to 5 days preoperatively, at 4 to 8 hr after postoperative removal of the catheter, and 1 to 2 weeks postoperatively. Patients were ineligible if they had no follow up urinalysis and urine culture.
All data were recorded prospectively. The clinical parameters subjected to analysis were age, preoperative maximal flow rate, residual urine volume, prostate volume, prostate-specific antigen level, resected prostate volume (fresh tissue weight in the operating room), operation time (minutes), duration of postoperative catheterization, presence of bladder stones, recent (within 2 weeks) or preoperative UTI, presence of preoperative Foley catheterization, duration of antibiotic therapy (intravenous and oral), presence of diabetes mellitus (DM), operation method, type of antibiotics, and infectious complication rate. Postoperative infectious complications were defined as febrile UTI and bacteriuria.
Defintion of postoperative infectious complications
Because "postoperative bacteriuria" is the best-assessed outcome parameter, we chose this as the primary outcome parameter for our purposes. Because we were aware of the possible lack of clinical significance of bacteriuria, our secondary outcome parameters were symptomatic UTI, fever, sepsis, and bacteremia. Therefore, postoperative infectious complications were defined as febrile UTI and bacteriuria. Febrile UTI and bacteriuria were described according to the clinical guideline for the diagnosis and treatment of urinary tract infections in Korea (14).
Use of antibiotics
All patients received an initial intravenous antibiotics 30 to 60 min before surgery. The oral antibiotics were the same type as the intravenous antibiotics used previously. The selection of intravenous antibiotics was chosen according to physician preference.
Statistics
Statistical analysis was performed using the SPSS software, version 17.0 (SPSS Inc., Chicago, IL, USA). Descriptive analysis was performed to assess patient demographics. Univariate and multivariate logistic regression analyses (stepwise backward procedure) were performed to assess the associations of clinical parameters with infectious complications. Statistical significance was set at P<0.05 for all analyses.
RESULTS
Baseline demographics
The mean age of the enrolled patients was 69.1±7.0 yr. The mean prostate volume was 55.8±54.5 mL. Of all 424 patients, 215 underwent transurethral prostate surgery and 209 patients underwent open or laparoscopic prostate surgery. The mean durations of the operative, intravenous antibiotic administration, and postoperative Foley catheter placement were 165.1± 91.6 min, 3.4±2.3 days, and 9.0±6.4 days, respectively. The frequency of DM, recent UTI, preoperative UTI, and preoperative Foley catheter placement were 17.9%, 8.0%, 7.5%, and 11.8%, respectively. A first- or second-generation cephalosporin was given to 369 (87.0%) patients, and a third-generation cephalosporin to 51 (12.0%) patients (Table 1). Postoperative infectious complications developed in 149 (34.9%) paients, including postoperative bacteriuria (29.0%), fever (9.2%), and bacteremia (0.2%) (Table 1).
Clinical parameters associated with postoperative infectious complications
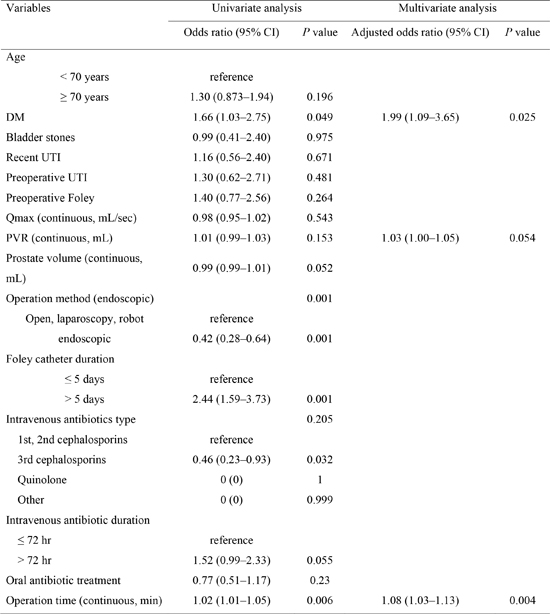
Univariate analysis indicated that long-term (>5 days) Foley catheterization (OR, 2.44; 95% CI, 1.59-3.73, P=0.001), operation time (OR, 1.02; 95% CI, 1.01-1.05, P=0.006), transurethral prostate surgery (OR, 0.42; 95% CI, 0.28-0.64, P=0.001), DM (OR, 1.66; 95% CI, 1.03-2.75, P=0.049), and third-generation cephalosporins (OR, 0.46; 95% CI, 0.23-0.93, P=0.032) were risk factors for postoperative infectious complications. However, the prostate volume (OR, 0.99; 95% CI, 0.99-1.01, P=0.052) and a duration of intravenous antibiotic administration>72 hr (OR, 1.52; 95% CI, 0.99-2.33, P=0.055) showed borderline significance (Table 2).
Multivariate analysis revealed that DM (adjusted OR, 1.99; 95% CI, 1.09-3.65, P=0.025) and operation time (adjusted OR, 1.08; 95% CI, 1.03-1.13, P=0.004) were independently associated with postoperative infectious complications (Table 3).
Culture results
Among the patients who had postoperative bacteriuria and bacteremia (n=124), 4 patients had 2 organisms in culture. The quinolone resistance microorganisms were identified as Escherichia coli (n=4), Klebsiella pneumoniae (n=2), Pseudomonas aeruginosa (n=1), Enterobacter spp. (n=1), Enterococcus spp. (n=14), Acinetobacter baumannii (n=1), and others (n= 2). Thus, overall quinolone resistance rate were 19.5% (25/128). In addition, the results of extended spectrum β-lactamase (ESBL) positivity were similar to those of quinolone resistance rate (21.1%, Table 4).
DISCUSSION
The incidence of postoperative infectious complications after prostate-related surgery in this study was 34.9%. DM and a long operation time were independently predictive of postoperative infectious complications after prostate-related surgery. In urologic surgical practice, the prevention of postoperative infectious complications is important; however, few studies have evaluated the risk factors for postoperative infectious complications in such settings.
The current classes of surgery/surgical field contamination were developed and updated for open surgery and to determine the relative risk of surgical wound infection (15). Urological interventions have not been classified, and the current definitions do not include endoscopic surgery. In addition, the current guidelines for surgical site infection focus on gastrointestinal surgery (5). The criteria for assessment of contamination categories in open surgery are the type of incision, level of spillage, and evidence of infection or inflammation; UTI is not included. These guidelines cannot be adapted to urologic prostatic surgery because many urological procedures are associated with urine exposure and endourological procedures. Whether opening of the urinary tract should be classified as clean or clean-contaminated surgery in cases of negative urine culture remains controversial. The same applies to endoscopic and transurethral surgery. For practical and strategic reasons, clean-contaminated urologic operations should be extended. In an extension, this classification could theoretically be widened to also cover endoscopic urological procedures, the surgical site being the urinary tract and the surgical site infection being UTI.
Several studies have shown that these procedures should be considered clean-contaminated because urine culture is not always a predictor of bacterial presence, and the lower genitourinary tract is colonized by microflora, even in the presence of sterile urine (3, 16). According to recent criteria for the assessment of level of surgical class/surgical field contamination in prostatic urological procedures, these procedures are considered contaminated in the presence of a previous history of UTI/urogenital infection (prostatitis), presurgical catheterization, or controlled bacteriuria (4).
In addition, there is a paucity of evidence for prophylactic antibiotics and risk factors in laparoscopic radical prostatectomy. Therefore, it is valuable to evaluate the risk factors for postoperative infectious complications related to prostate surgery and the efficacy of prophylactic antibiotics in the era of antibiotic resistance.
Postoperative UTI and bacteremia are the principal complications after TURP; therefore, antibiotic prophylaxis is essential (17). However, the most optimal antibiotic regimen and duration of prophylaxis remain to be determined. According to the systematic reviews by Berry and Barratt (18) and Qiang et al. (19), the incidences of postoperative bacteriuria and bacteremia more severe than UTI are approximately 26.0% and 4.4%, respectively. In this regard, the authors concluded that antibiotic prophylaxis significantly decreases the development of post-TURP bacteriuria, post-TURP fever, sepsis, and the need for additional antibiotics post-TURP. In addition, there was a trend suggesting higher efficacy with a short course (<72 hr) of antibiotic prophylaxis than with a single-dose regimen (18).
No randomized controlled trials on antibiotic prophylaxis versus placebo/no antibiotics in total prostatectomy have been performed. Thus, there is a lack of baseline data on the infectious profile of this frequently performed operation. A few retrospective and prospective cohort studies have evaluated surgical site infections and catheter-associated bacteriuria following different antibiotic regimens. They concluded that the frequency of wound infection is low and that a single oral antibiotic dose is sufficient (10, 11, 12, 13).
The recommended antibiotic phrophylactic regimen for laparoscopic surgery is similar to that for open surgery. Because laparoscopic surgery is thought to be less invasive, the incidence of surgical site infection in laparoscopic procedures could be lower than that in open procedures. Rassweiler et al. (20) reported that surgical site infection occurred in 5 of 219 (2.3%) patients undergoing open radical prostatectomy while in just 1 of 438 (0.3%) undergoing laparoscopic radical prostatectomy.
Studies on antimicrobial prophylaxis in radical prostatectomy are rare, and most focused on surgical site infection and not UTI, as in TURP. No consideration has been given to postoperative UTI in prostatectomy, which carries a higher risk of bacteriuria than does TURP because of the long-term postoperative catheterization in prostatectomy.
In the present study, the postoperative infectious complications rate was 34.9%, and included postoperative bacteriuria (29.0%), fever (9.2%), and bacteremia (0.2%). The mean duration of antibiotic administration was 3.4 days, but neither the duration of antibiotic administration nor the type of surgery affected the postoperative infectious complications.
These data show that prostatectomy is associated with a high incidence of postoperative UTI and bactremia, as is TURP. From this perspective, it is logical to apply the antibiotic prophylaxis regimen of TURP to prostatectomy. In TURP, the prophylactic effect of multiple doses of cephalosporins for 24 to 72 hr is more effective than that of a single dose (18, 19). In the Japanese guidelines, radical prostatectomy is considered to be a clean-contaminated operation; therefore, antibiotic prophylaxis is recommended within 3 days (21).
In Asia, the incidence of antibiotic resistance is higher than that in Western or European countries, which recommend single-dose or <24-hr antibiotic prophylaxis. Thus, antibiotic prophylaxis within 3 days might be appropriate for Asian countries.
In terms of antibiotic type, there is a lack of evidence to suggest the routine use of one class of antibiotics versus another, with aminoglycosides, fluorquinolones, cephalosporins, and TMP-SMX all demonstrating efficacy in large meta-analyses (18). In our study, third-generation cephalosporins reduced the incidence of postoperative infectious complications on the univariate analysis, but did not result in a significant change in the multivariate analysis. Therefore, the prophylactic efficacy did not differ according to the antibiotic type, and a first- or second-generation cephalosporin is a reasonable option to reduce antibiotic resistance.
Several studies have investigated risk factors for postoperative infectious complications after TURP (6, 9, 16, 22, 23). Well-documented risk factors are preoperative bacteriuria, duration of the operation, rupture of closed drainage systems, and duration of postoperative catheterization. In the present study, as in previous studies, the operation time (adjusted OR, 1.08; 95% CI, 1.03-1.13, P=0.004) was a risk factor for postoperative infectious complications. The operation time was dependent upon surgeon experience and resected volume in TURP. In accordance, Wagenlehner et al. (16) added surgeon experience as a risk factor; and our previous study revealed resected volume as a risk factor (24). However, the current study was a multicenter study, and enrolled patients underwent radical prostatectomy or open prostatectomy; this is why we did not include surgeon experience or resected volume as risk factors for analysis. A history of preoperative or recent UTI and the duration of postoperative catheterization were not risk factors for postoperative complications in our study. This result may explained by the effective preoperative eradication of UTI and well-managed closed drainage systems after the procedure.
In our study, another risk factor for postoperative complications was DM (adjusted OR, 1.99; 95% CI, 1.09-3.65, P=0.025). The independent role of DM in infectious complications is still controversial (25). However, in a recent prospective study from Japan, poor postoperative blood glucose control was directly correlated to an increased rate of infectious complications (26). A stable and normal blood sugar level is considered to be important before, during, and after surgery (27). It is also recognized that bacteriuria is more often present in individuals with DM, and it is more severe and lasts longer (28). Because bacteriuria is a well-defined risk factor for postoperative infectious complications, patients with DM must have a controlled blood glucose level and no bacteriuria prior to surgery. In addition, because the incidence of DM is increasing in most societies, we can assume that there will be an increasing number of infectious complications.
The current study was not without drawbacks. First, the antimicrobial regimens and durations were not standardized. Thus, our findings should be interpreted cautiously, because each center has different clinical practice guidelines for antimicrobial prophylaxis in surgery. There is possible bias related to the quality control between different centers. However, in line with the recent evaluation of prophylactic antibiotic use for prostate surgery, a variety of antibiotics are being used prophylactically with varying duration depending on the hospital. Therefore, we sought to assess the practice of antibiotic prophylaxis for prostate surgery in Korea. Second, we did not consider locoregional antimicrobial resistance in our selection of antibiotics. Finally, heterogeneous population and operative methods can lead to the possibility of an unknown cofounder associated with infectious complications. However, to our knowledge, this is the first study in Korea to evaluate postoperative infectious complications after prostate surgery. No previous studies have investigated the risk factors for postoperative UTI after prostatectomy (29, 30). With a paucity of Korean data addressing this issue, the present study will serve as a basis for future prospective research.
Evidence concerning perioperative infections in the urological field is limited. The importance of postoperative bacteriuria, which is observed in the majority of the patients, is unknown. Further studies on long-term complications in patients with postoperative UTI, such as patients with chronic prostatitis and urethral stricture, will be required. Further studies to gather additional evidence are necessary to establish Korean guidelines.
In conclusion, based on our results, a prolonged operation time and the presence of DM affect postoperative infectious complications associated with prostate surgery. Neither the type/duration of prophylactic antibiotics nor the type of surgery resulted in a difference in infectious complications. Additional research with multicentric prospective well-designed randomized controlled trials is needed to further evaluate infectious complications after prostate surgery.


 XML Download
XML Download