

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anti-Müllerian hormone (AMH), also called Müllerian-inhibiting substance, has become known as an important regulator of follicle development (1, 2). It is exclusively produced by granulosa cells of preantral and small antral follicles, presumably independently of follicle-stimulating hormone (FSH) (3, 4, 5). AMH is involved in the inhibition of the growth from primordial to primary follicle as well as in follicle recruitment and selection (3, 4). Moreover, it attenuates the FSH-dependent increase in aromatase activity during early follicle development and reduces the number of LH receptors in FSH-stimulated granulosa cells (5).
Serum AMH has been well studied as an excellent marker of ovarian reserve. Serum AMH levels have shown great sensitivity to ovarian aging and significant correlation with antral follicle count, and this relationship was stronger than that for other hormonal markers (6, 7). In addition, it has been a useful predictor of the ovarian response to controlled ovarian stimulation (COS) (8, 9, 10). All of these evidences show that serum AMH quantitatively reflects the size of the ovarian follicle pool; in other words, AMH is a quantitative marker of ovarian reserve and response.
Several studies on the serum AMH level showed that AMH levels during COS may reflect the oocyte and embryo quality (1, 11, 12, 13). Studies on the follicular fluid (FF) AMH levels have shown a more direct role of AMH as a regulator of human folliculogenesis (14, 15, 16). Fanchin et al. (14) demonstrated that FF AMH levels of the preovulatory follicle are positively associated with embryo implantation. Takahashi et al. (16) showed that oocytes are more likely to be fertilized when follicles have high concentrations of AMH. However, there have been very few studies on the direct relationship between FF AMH levels and quality of oocyte and embryo and this issue require further study.
The objectives of this prospective study were to investigate the relationship between FF AMH levels and the ensuing oocyte and embryo quality and to clarify the role of AMH as a qualitative indicator of ovarian follicular status.
MATERIALS AND METHODS
Subjects
A total of 65 FF samples from 54 women were collected. The inclusion criteria were as follows: 1) age<42 yr; 2) normal ovulatory cycle with cycle lengths between 25 and 35 days; 3) body mass index<32 kg/m2; and 4) no evidence of endocrine abnormalities such as hyperprolactinemia, thyroid dysfunction, or polycystic ovarian syndrome as defined by the Rotterdam criteria (17). Patients with stage III-IV endometriosis were excluded. FF was obtained from the largest follicle sized≥20 mm of mean diameter from each ovary. FF containing no oocyte or contaminated with blood was excluded.
COS protocol
All women received ovarian stimulation using gonadotropin releasing hormone (GnRH) antagonist multiple-dose flexible protocols. Recombinant FSH (Gonal-F; Serono, Geneva, Switzerland) was started on the third menstrual cycle day without oral contraceptive pretreatment. The GnRH antagonist, cetrorelix (0.25 mg Cetrotide; Serono), was added daily, starting when the diameter of the leading follicle reached 14 mm and ending when the mean diameter of the leading follicle reached 18 mm or when 2 or more follicles had a diameter of 17 mm. Recombinant human chorionic gonadotropin (hCG) (250 µg Ovidrel; Serono) was administered subcutaneously 36 hr before transvaginal oocyte retrieval. Up to 3 embryos were transferred 3 days after oocyte retrieval. The luteal phase was supported with 50 mg of progesterone in oil (Progest; Samil, Seoul, Korea) or 8% progesterone gel (Crinone; Serono) daily, initially for 14 days starting on the day of oocyte retrieval and continuing for another 6 to 8 weeks in cases where a pregnancy was achieved. Pregnancy was first assessed using serum β-hCG levels 14 days after oocyte retrieval, and clinical pregnancy was defined by the presence of an intrauterine gestational sac with pulsating fetal heart beats.
FF collection
FF was obtained from the largest follicle sized≥20 mm of mean diameter from each ovary during oocyte retrieval. We punctured the largest follicle and aspirated the fluid into an empty bottle without any media. After the needle was withdrawn, it was flushed to obtain the possible trapped oocyte in the dead space of the collection needle. Samples were collected from only 1 follicle for each ovary, and only 1 needle was used for each follicle. Collected samples were centrifuged at 500×g for 15 min; FF supernatant was stored at -20℃ until assayed.
FF AMH measurements
FF AMH levels were measured using enzyme-linked immunosorbent assay (Immunotech Beckman Coulter, Marseille, France). The measurement range was 0.14-21 ng/mL. Intra- and inter-assay coefficients of variation were 12.3% and 14.2%, respectively, with a sensitivity of 0.14 ng/mL.
Definitions of AMH groups
Samples were divided into 3 groups according to the FF AMH levels: below the 33th percentile (low group, FF AMH<2.1 ng/mL, n=21), between the 33th and the 67th percentile (intermediate group, FF AMH=2.1-3.6 ng/mL, n=22), or above the 67th percentile (high group, FF AMH>3.6 ng/mL, n=22).
Fertilization and culture
Oocytes were placed in the insemination medium (Sydney IVF fertilization medium; Cook Women's Health, Spencer, IN, USA) 1 to 4 hr before insemination with 50,000 to 500,000 motile spermatozoa per milliliter of medium. Intracytoplasmic sperm injection was performed in our institution according to the following criteria: 1) total motile sperm count<50,000, 2) retrieval of fewer than 3 oocytes, or 3) a history of total failed fertilization. Fertilization was assessed 16 to 18 hr after insemination by the presence of 2 pronuclei and a second polar body. The fertilized oocytes were maintained in the culture medium (Sydney IVF cleavage medium; Cook Women's Health).
Definitions of the outcome measures
Normal fertilization was defined as the presence of 2 pronuclei and a second polar body. Top-quality embryos were designated as grade A or B embryos with at least 6 blastomeres on day 3 after fertilization. The embryo grades were classified according to the our laboratory criteria: A - no blastomeres fragmentation; B - fragmentation less than 20%; C - fragmentation between 20% -50% anucleate fragments, irregularity of blastomeres, and no apparent morphologic abnormalities; D - fragmentation above 50%. Embryo score was calculated as the points of embryo grade multiplied by the number of blastomeres. Four points were given for embryo grade A, 3 for grade B, 2 for grade C, and 1 for grade D.
Statistical analysis
Data were analyzed with SPSS software version 21.0 (SPSS, Chicago, IL, USA). Data were compared by Student's t-test, analysis of variance (ANOVA), or chi-square test, as indicated. Correlation between the FF AMH level and day 3 embryo score was determined by bivariate correlation analysis with Pearson's correlation coefficients. The result was considered as significant when the P value was <0.05.
RESULTS
Clinical characteristics of the study subjects and outcomes of COS
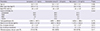
Clinical characteristics of the study subjects and COS outcomes are presented in Table 1. Comparing the characteristics and COS outcomes among the low, intermediate, and high groups, no significant differences were observed except for basal FSH and numbers of oocytes retrieved.
Correlation of the FF AMH level with embryo quality
FF AMH levels correlated positively with the matched embryo score on day 3 after fertilization (r=0.331; P=0.015) (Fig. 1).
Fertilization and top quality embryo rate in low, intermediate, and high AMH groups
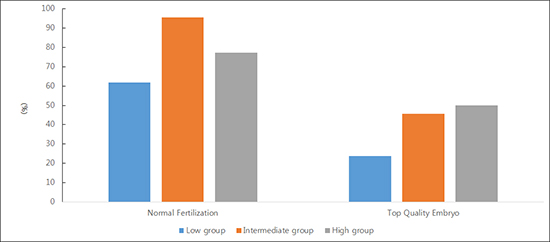
The normal fertilization rate was significantly lower in the low group than in the intermediate group (61.9% vs. 95.5% vs. 77.3%, in the low, intermediate, and high groups, respectively, P=0.028). The top-quality embryos rate showed the slight increases in the groups but differences did not reach statistical significance (23.8% vs. 45.5% vs. 50.0%, respectively, P=0.175) (Fig. 2).
DISCUSSION
The present study demonstrated AMH production by a single preovulatory follicle is positively related to the quality of the ensuing oocyte and embryo. Our work has for the first time conducted prospective study in individual lead follicle in conventional COS cycles. It may show the most direct relationship between FF AMH level and ensuing oocyte.
Our results, associating FF AMH levels on the day of oocyte retrieval and oocyte quality are consistent with the results from a previous studies (16). Takahashi et al. (16) demonstrated that FF AMH could be a predictive marker for success in oocyte fertilization in their retrospective study. Fanchin et al. (14) studied the relationship between serum and FF AMH levels and the fate of oocytes in IVF-ET conducted in monodominant follicle cycles. They showed that the FF AMH levels constitute a useful follicular marker of embryo implantation, but they failed to find any significant difference in the quality of oocytes and embryos originating from high- or low- AMH -producing follicles. This issue deserved further confirmative studies, and our study reveals an answer. On the other hand, Cupisti et al. (18) and Mehta et al. (19) showed that FF AMH levels were inversely correlated with oocyte maturation and development potential such as, fertilization, embryo quality and clinical pregnancy rate. In these studies, AMH levels were measured in the pooled FF rather than in any specific follicle. Assays from pooled FF may not reflect the microenvironment surrounding a specific oocyte.
The fate of the oocyte strongly depends on the health of the corresponding follicles, especially the surrounding cumulus cells. Mutual interdependence of AMH-producing granulosa cells and oocytes can be conceivable, and much evidence has been presented. Previous studies have shown that apoptosis of granulosa cells negatively affects the developmental competence of the oocyte (20, 21). Granulosa cells in the follicles from oocytes that were fertilized and developed into high-quality embryos showed a significantly lower incidence of apoptotic rates than those from oocytes that did not (22). Furthermore, growing evidence indicates that the oocyte regulates granulosa cell AMH expression. Higher AMH mRNA expression was seen in cumulus cells than in mural granulosa cells in mouse antral follicles (23). Salmon et al. (24) demonstrated that the oocytes in the preovulatory follicle directly induce the granulosa cell AMH expression in close contact with each other.
Limitation of this study is that it was focused exclusively on preimplantation development. We transferred multiple embryos, 2 or 3 embryos depending on the patient's age and embryo quality to increase the probability of pregnancy. Thus, it was impossible to follow up the subsequent implantation rate and clinical pregnancy rate according to the each oocyte. It needs to be further studied using single ET cycles.
In conclusion, the present study indicates that the FF AMH level predicts oocyte and embryo quality. FF AMH levels could be used as a reliable marker of oocyte competence. Additional prospective studies are needed for the clinical application of FF AMH to improve IVF-ET outcomes.


 XML Download
XML Download