

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gallbladder polyps (GBP) are defined as lesions protruding from the gallbladder mucosa that are usually found incidentally by ultrasonography (USG) (1). GBP are classified into two categories: true polypoid neoplasms, including benign adenomas and adenocarcinomas, and non-neoplastic polyps, including cholesterol polyps, inflammatory polyps, and adenomyomatous hyperplasia (2). The clinical implication of GBP lies in its malignant potential. Although the reported malignancy rate of GBP is only 3%-8% (3), late or missed diagnoses of gallbladder cancer may be fatal. The overall 5-yr survival rate of gallbladder cancer is historically < 5%; however, this has improved dramatically with early treatment (4). Thus, GBP should be detected as early as possible. Unfortunately, USG, which is commonly chosen as the initial imaging modality for evaluating gallbladder problems, has low sensitivity for the diagnosis of gallbladder cancer until advanced disease stages (5). Although several early gallbladder cancers present as GBP on USG, the biologic nature of GBP is difficult to discern prior to surgical resection (6). These facts highlight the clinical significance of GBP.
Because the pathogenesis of GBP has not yet been clearly defined, evaluating risk factors for GBP will increase its understanding, diagnosis, and prevention. The detection rate of GBP has been increasing due to improved USG quality and availability. Several studies have reported the prevalence of GBP as identified on USG (7, 8). However, the prevalence of GBP varies widely among populations and study designs and there are few data on the population-adjusted prevalence and changes in GBP risk factors for > 10 yr in a specific ethnic population. Therefore, the aim of this study was to evaluate the shifting prevalence and risk factors for GBP in Korea.
MATERIALS AND METHODS
Subjects
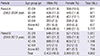
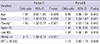
Between January 2002 and December 2012, 48,591 (≥ 20 yr of age) subjects underwent abdominal USG as part of a health check-up at Keimyung University Dongsan Medical Center in Daegu, Korea. We retrospectively reviewed the subjects' medical records. After excluding subjects who underwent cholecystectomy, age- and gender-matched random sampling was performed considering the population composition ratio. The sampling process was based on the data from the Korea National Statistical Office population census conducted in 2010 (9). This study included 14,250 consecutive subjects (6,898 men and 7,352 women). To evaluate the GBP trends over time, we divided the total 11-yr time frame into Period A (2002-2004) and Period B (2010-2012). Of the total 14,250 subjects, 3,772 were included in Period A and 4,962 were included in Period B. Table 1 shows the age and gender distribution of the studied population in Periods A and B. If a subject underwent more than one health screening at our center, the most recent data were analyzed.
Diagnosis of GBP
After fasting for at least 11 hr prior to the examination, radiology specialists performed USG examinations using an ACUSON 128XP 10 (Acuson, Charleston Road, CA, USA) and Philips-iU22 (Philips, Bothell, WA, USA) equipped with a 3.5/5.0 MHz ultrasound probe. According to the standard radiologic criteria, GBP were diagnosed if the lesions were immobile, hyperechoic masses without acoustic shadowing that were attached to the gallbladder (GB) wall (10).
Analysis of risk factors
Blood serum samples were collected early in the morning after the subject had fasted for at least 8 hr. Levels of fasting plasma glucose (FPG), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total cholesterol, triglyceride (TG), high density lipoprotein cholesterol (HDL-C), γ-glutamyl transferase (γ-GTP), and total bilirubin were measured using a Hitachi-747 autoanalyzer (Hitachi, Nakashi, Tokyo, Japan). Hepatitis B surface antigen (HBsAg) and hepatitis C virus antibody (anti-HCV) were detected using an enzyme-linked immunosorbent assay on AxSYM (Abbott Laboratories, Abbott Park, IL, USA) and Coda (Bio-rad, San Francisco, CA, USA).
Body mass index (BMI) was calculated by dividing weight by height squared (kg/m2). Obesity was defined according to World Health Organization BMI criteria for an Asian population as BMI≥25 kg/m2 (11). Blood pressure (BP) was measured at each patient's left arm in the seated position after 5-10 min of quiet rest using a mercury sphygmomanometer. A subject was considered to have hypertension (HTN) if they had a systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg or were taking anti-hypertensive agents (12). Diabetes mellitus (DM) was diagnosed when the FPG level was ≥126 mg/dL, the hemoglobin A1c level was ≥6.5%, or a patient was being treated with oral hypoglycemic agents or insulin. Impaired fasting glucose (IFG) was defined as a FPG level of 100-125 mg/dL (13). The categorized cut-off value of serum biochemistry was determined according to the reference standard of our laboratory.
Statistical analysis
Statistical analyses were performed using SPSS version 18.0 (SPSS, Inc., Chicago, IL, USA). Student's t-test was used to compare continuous variables. Categorical variables were analyzed using Pearson's chi-square and and Fisher's exact test. Logistic regression analysis was used to analyze potential risk factors for GBP. Two-tailed P values<0.05 were considered statistically significant.
RESULTS
General characteristics of GBP
Table 2 shows the baseline characteristics of the Korean population estimated from Period A to Period B. The presence of HBsAg (P<0.001) was more frequently observed in Period A than in Period B. Subjects in the two periods did not differ in age, gender distribution, mean BMI, presence of HTN, DM, IFG, or GB stone and other laboratory parameter. The mean GBP sizes were 4.10±1.94 mm in Period A and 3.67±1.61 mm in Period B. A total of 68.1% (92/3,772) of GBP in Period A and 73.8% (256/4,962) of GBP in Period B were >5 mm.
Prevalence of GBP
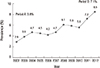
Among a total of 14,250 subjects, 765 had GBP, and the overall prevalence through the 11-yr time period was approximately 6.3%. The annual prevalence of GBP is shown in Fig. 1. The prevalence curve increased linearly from 2.9% in 2002 to 8.5% in 2012. From Period A to B, mean annual prevalence increased from 3.8% to 7.1%. During the total study period, the average ages of the GBP and control groups were 42.55±12.75 and 43.29±13.77 yr, respectively. GBP were more frequently found in men (434/6,898; 6.3%) than in women (331/7,352; 4.5%). The prevalence of GBP was further stratified by gender in the different age groups in Periods A and B. Men showed a higher prevalence than women in all age groups and in both periods. The peak prevalence was in men 30-39 yr of age (7.0% in Period A and 9.3% in Period B; Fig. 2).
Factors related to GBP
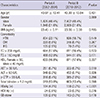
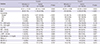
Univariate analysis showed that age (P=0.042), male gender (P=0.002), obesity (P<0.001), and the presence of HBsAg (P<0.001) were significantly associated with GBP in Period A, whereas age (P=0.010), male gender (P<0.001), obesity (P<0.001), high TG levels (P<0.001), low HDL levels (P<0.001), and high AST levels (P=0.030) were significantly associated with a high probability of GBP in Period B (Table 3). On multivariate analysis, male gender (odds ratio [OR], 1.55; 95% confidence interval [CI], 1.08-2.23; P=0.018), and obesity (OR 1.90; 95% CI 1.32-2.72; P<0.001) were significantly associated with GBP in both periods. However, HBsAg lost its significance in Period B. Instead, hyper-TG (OR, 1.48; 95% CI, 1.09-2.01; P=0.013), and low HDL (OR, 1.38; 95% CI, 1.06-1.81; P=0.018) were correlated with GBP in Period B (Table 4).
DISCUSSION
The prevalence rates of GBP vary among countries and regions. Results from Western studies have shown a GBP prevalence of 1.4%-6.9% (10, 14, 15), whereas Asian studies have shown a GBP prevalence of 2.2%-9.5% (1, 16, 17). Such geographic differences may be associated with different genetic and environmental factors. The prevalence of GBP in Korea is not high; the reported prevalence rate was 2.2% in 1998-2003 (17). However, with social and environmental changes, increasing life expectancies, greater levels of health consciousness, and the increased popularity of USG, the prevalence of GBP in Korea has increased; from Period A to B, the population-adjusted prevalence rate of GBP increased from 3.8% to 7.1%. The increase in prevalence observed between the two periods of our study corresponded with those observed in other studies (18, 19).
Many studies have reported on the risk factors that predispose patients to developing GBP. It is known that male gender is a risk factor for GBP (8). Consistent with previous studies, we found that men had a higher prevalence of GBP than did women in all age groups in periods A and B. The prevalence of GBP peaked in men 30-39 yr of age in both of these periods. In most studies, the highest prevalence of GBP has been observed in the third to fifth decades of life (1, 16). The reasons for peak incidence of GBP in middle aged people are still unclear. In our study, the fact that most of subjects who had undergone cholecystectomy were in their 50s and 60s or older may partly affect the high prevalence rate of GBP in middle aged subjects. In logistic regression analysis, no association was observed between age and GBP in this study; however, male gender seems to be a significant risk factor for GBP.
The impact of obesity on the development of GBP has been documented in several studies (1, 17). Obesity is a global public health problem. According to the national survey, the overall prevalence of obesity in Korea increased during the period of 1998-2010 (20). In the current study, obesity was a common risk factor for GBP in Periods A and B. Hence, GBP appears to be predominant in obese subjects, and the increase in the prevalence of GBP can be partly attributed to the increasing rates of obesity.
Several authors found that the prevalence of GBP was higher in patients with HBV infection than in those without HBV infection (8, 16). Meanwhile, others did not find a relationship between HBV infection and GBP (21, 22). The underlying mechanism of this association remains elusive (8). In the present study, the presence of HBsAg had statistical meaning in Period A; however, it was not continuously meaningful in Period B. This result is probably related to the nationwide HBV vaccination program. Korea was an endemic area for HBV infection in the past. The Korean government's universal HBV vaccination program, which started in 1991, was administered to all infants in 1995 (23). As a result, the prevalence of HBsAg in the Korean population has steadily decreased from 4.60% in 2001 to 2.98% in 2010 (24). Although Korea is still endemic for HBV infection (25), this dramatic decline in the general population may influence the changing risk factors for GBP.
In the current study, elevated TG and low HDL levels were significantly associated with GBP. Most GBP are cholesterol polyps. Although the pathogenesis of GBP remains poorly understood, several investigators have hypothesized that direct deposition of bile or blood cholesterol may contribute to the formation of cholesterol polyps (26). In support of this mechanism, a similar association has been suggested between GBP and lipid profile abnormalities (27, 28). However, this shift in association in the current study was distinctly different from that reported in previous studies. Our results suggested that lipid profile abnormalities are emerging risk factors. The reason for this shift in temporal trends is unclear. However, we hypothesized that it is probably associated with the lifestyle and diet changes in Koreans. With the rapid socioeconomic development of the past few decades, Koreans have experienced remarkable transitions in lifestyle as well as food choices (29). According to the data from the Korean nationwide survey, the prevalence of dyslipidemia has increased substantially in recent years (30). The most remarkable finding of this study is that this emerging trend of lipid profile abnormality is contrary to the trends of loss in the significance of HBV infection in recent years. Considering these results, we assumed that the transition of GBP risk factors may be attributable to the changes in social economy and health policies in Korea.
The increasing prevalence of GBP observed in our study can be explained by the changing trends in risk factors. Especially, metabolic status such as obesity and dyslipidemia may had an important role in increasing prevalence of GBP. However, it is rather premature to conclude that the increased prevalence is only a consequence of shifting trends in risk factors. Indeed, the prevalence of GBP may yet be attributed to unrevealed risk factors. Furthermore, increased detectability probably accounts for the increased prevalence. Compared with Period A, polyps smaller than 5 mm were more frequently observed in Period B. Numerous recent studies support our results that this finding is likely due to the increased availability and improved technology of USG (16, 22).
Several recent studies have advocated the role of metabolic syndrome in GBP (8, 22). Unfortunately, we could not evaluate the same because waist circumference was not included among the routine check-up items of the examinations performed at our health screening center. Furthermore, HTN and IFG, which are contributors to metabolic syndrome, were not identified as risk factors for GBP in this study.
Our study had several limitations. First, because of age- and gender-matched selection, relatively few cases were ultimately included. However, this is a common difficulty in evaluating the prevalence rate because subjects who visit a single health screening center are not representative of an entire community. Second, FPG was measured at one time only during a single visit. According to the current definition (31), DM is diagnosed only once a FPG level of >126 mg/dL is documented twice. Similarly, BP was measured once during a single visit. HTN is diagnosed on the basis of the average of at least two BP readings at more than two visits after the initial screening (12). Although these methods were inevitable due to the retrospective design of this study, the fact that HTN and DM can be over- or underestimated may have affected the results. Third, it is often difficult to discriminate between small polyps (<5 mm) and GB stones. In the present study, most of the polyps were <5 mm and the diagnosis of GBP was based on the USG criteria.
Despite these limitations, the strength of this study is its design, which documented the changes over a long period of time based on population-adjusted selection. Most epidemiologic studies on GBP were not based on population-adjusted results, so it is possible that an inappropriate distribution of age and sex was analyzed. To our knowledge, this is the first report of the temporal changes in the prevalence and risk factors of GBP for >10 yr in Korea. Thus, the results of this study are reliable and could be representative of the general Korean population.
In conclusion, GBP are not rare and the prevalence of GBP increased dramatically from 2002 to 2012. The risk factors for GBP have also changed over time. The risk factors for GBP are shifting from HBsAg positivity to increased TG levels and decreased HDL levels. Male gender, obesity, and lipid profile abnormalities are the current risk factors for GBP in Korea. These results may be a valuable resource for health education, health care policy, and future studies.

 XML Download
XML Download