

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Helicobacter pylori is a curved, microaerophilic, Gram-negative bacterium that was isolated in 1983 from the stomach biopsy specimens of patients with chronic gastritis (1). The bacterium colonizes the human gastric mucosa, and the infection can persist for decades. H. pylori infection is recognized as a causal factor of chronic gastritis, peptic ulcers, and gastric cancer (2). The World Health Organization has declared H. pylori as a class I carcinogen. H. pylori colonization should be eradicated in patients with peptic ulceration because eradication not only accelerates ulcer healing but also prevents long-term ulcer relapse. Treatment regimens consisting of a proton pump inhibitor (PPI) and a combination of 2 or more antibiotics, including amoxicillin and clarithromycin, are highly effective; however, recently, drug resistance has become a significant clinical problem for the management of H. pylori infections. Reports from Korean patients have shown a continuous increase in primary resistant strains for several antibiotics such as clarithromycin, amoxicillin, metronidazole, tetracycline, and fluoroquinolones (including ciprofloxacin and moxifloxacin) from 1987 to 2003 (3). Consistent with these findings, eradication rates for first-line therapy have decreased to less than 75% in Korea (4). Resistant strains of bacteria hinder successful eradication because treatment of H. pylori infection is usually initiated on an empirical basis. Information about the status and changes in H. pylori resistance to antibiotics is of the utmost importance for designing successful treatment strategies. Clarithromycin resistance reduced efficacy of clarithromycin-based triple therapy by over 50% (5). The rates of eradication were 97% for clarithromycin-susceptible strains and 0% for clarithromycin-resistant strains in Korean patients (3). Therefore, clarithromycin resistance is a prime concern for clinicians who treat patients infected with H. pylori. Matsuoka et al. (6) first reported that mutations in 23S rRNA are associated with clarithromycin resistance in H. pylori. Point mutations in 2 positions (A2143G or A2144G) are the most commonly reported mutations in clarithromycin-resistant H. pylori isolates (6). However, little information is available regarding the antibiotic minimum inhibitory concentrations (MICs) for H. pylori isolates and the mechanism of clarithromycin resistance in Korea. Therefore, we studied H. pylori isolates obtained from Korean patients with the following objectives: 1) to determine the antibiotic resistance rates of H. pylori and the distribution of MICs for amoxicillin, clarithromycin, metronidazole, tetracycline, ciprofloxacin, moxifloxacin, and levofloxacin, 2) to evaluate the efficacy of clarithromycin-based triple therapy in H. pylori eradication and 3) to detect mutations in 23S rRNA of clarithromycin-resistant H. pylori isolates from Seoul, Korea.
MATERIALS AND METHODS
Patients and H. pylori Strains
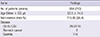
Two hundred and twelve strains of H. pylori were isolated from 204 patients attending Chung-Ang University Yongsan Hospital. None of the patients had been administered antibiotics, PPI, or non-steroidal anti-inflammatory drugs during the preceding 3 months. The patients had a mean age of 52.5±14.5 yr (115 men, 89 women) and were diagnosed with one of the following; gastritis (n=119), gastric ulcer (n=26), duodenal ulcer (n=41), combined gastric and duodenal ulcer (n=15), and stomach cancer (n=3) (Table 1). Different fingerprints of randomly amplified polymorphic DNA obtained by polymerase chain reaction (PCR) were observed in the paired strains obtained from the gastric antrum and body of 8 patients (Fig. 1).
The H. pylori strains were cultured for 4 days under microaerobic conditions (5% O2, 10% CO2, and 85% N2) as previously described (7). All stock cultures were stored in brucella broth supplemented with 15% glycerol and 10% fetal bovine serum at -196℃. These preparations were thawed and subcultured for the subsequent experiments.
Determination of Antibiotic MICs
The MIC values of amoxicillin (Sigma Chemical Co., St Louis, MO, USA), clarithromycin (Abbott Laboratories, Abbott Park, IL, USA), metronidazole (Sigma), tetracycline (Sigma), ciprofloxacin (Sigma), moxifloxacin (Sigma), and levofloxacin (Sigma) against H. pylori isolates were confirmed 3 times in triplicates using the serial 2-fold agar dilution method as described previously (3, 8). Briefly, bacteria were subcultured on Mueller-Hinton agar that was supplemented with 5% defibrinated sheep blood for 48 hr. The bacterial suspension, adjusted to McFarland no. 2 (6×108 colony-forming units/mL), was inoculated directly onto each antibiotic-containing agar dilution plate. After 72 hr of incubation, the MIC of each antibiotic was determined. Quality control was performed using H. pylori ATCC 43504 (8). Resistant breakpoints of MICs for amoxicillin, clarithromycin, metronidazole, tetracycline, and fluoroquinolones (ciprofloxacin, moxifloxacin, and levofloxacin) were defined as >0.5, >1.0, >8.0, >4.0, and >1.0 µg/mL, respectively (8, 9).
Efficacy of clarithromycin-based triple therapy for H. pylori eradication
The retrospective study was conducted for the evaluation of eradication rate of clarithromycin-based triple therapy at Yongsan Hospital in Seoul, Korea. We included all patients that were received H. pylori eradication and performed to determine if H. pylori had been successfully eradicated between 2005 and 2010. The definition of H. pylori eradication success was as follows: 1) negative result in urea breath test (UBT) or 2) negative result in both rapid urease test and histology after eradication therapy.
Restriction fragment length polymorphism (RFLP) and DNA sequencing analysis
H. pylori genomic DNA was extracted as previously described (10). Oligonucleotide primers (sense, 5'-CCACAGCG ATGTGGTCTCAG-3'; antisense, 5'-CTCCATAA GAGCCAAAGCCC-3') were used to detect mutations in the 23S rRNA gene that resulted in clarithromycin resistance. The PCR profile consisted of 35 cycles of denaturation for 1 min at 94℃, annealing for 1 min at 55℃, and extension for 1 min at 72℃. Amplicons (424 bp each) of the 23S rRNA gene were digested with either BsaI (New England BioLabs, Beverly, MA, USA) for 14 hr at 50℃ or BbsI (New England BioLabs) for 14 hr at 37℃ to detect the A2144G and A2143G mutations, respectively (10). Digested fragments were separated on a 1.5% agarose gel and viewed on a Gel Doc XR system (Bio-Rad Laboratories, Hercules, CA, USA).
Sequencing was performed with nonrestricted PCR products that were purified using Promega gel clean-up system (Promega Co, Madison, WI, USA). Purified PCR products were sequenced directly using the BigDye terminator sequencing kits and ABI PRISM 3730XL Analyzer (Applied Biosystems, Foster City, CA, USA).
RESULTS
Prevalence of antibiotic resistance and determination of MICs
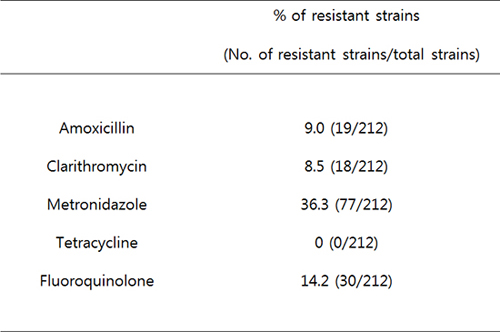
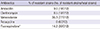
Amoxicillin, clarithromycin, metronidazole, tetracycline, and fluoroquinolone (ciprofloxacin, moxifloxacin, and levofloxacin) resistance rates were 9%, 8.5%, 36.3%, 0%, and 14.2%, respectively (Table 2). Additionally, the antibiotic MICs are shown in Fig. 2. These MIC values of amoxicillin, clarithromycin, metronidazole, tetracycline, and fluoroquinolones were ranged from 0.0625 to 4 µg/mL, from 0.0625 to 16 µg/mL, 0.5 to 128 µg/mL, from 0.125 to 4 µg/mL, and from 0.125 to 16 µg/mL, respectively.
Multidrug resistance (MDR) of H. pylori
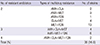
Thirty-five of 212 strains (16.5%) were resistant to at least 2 antimicrobial agents (exhibiting MDR) (Table 3). The most common MDR was to levofloxacin plus metronidazole. Resistance to 3 and 4 drugs were observed in 10 (4.7%) and 2 (0.9%) strains, respectively.
Eradication Rate of Clarithromycin-based Triple Therapy
A total of 833 patients were evaluated, who had received H. pylori eradication therapy from 2005 to 2010 in Chung-Ang University Yongsan Hospital. The patients had a mean age of 55.3 ±13.0 yr (539 men, 294 women) and were diagnosed with one of the following; gastritis (n=209), gastric ulcer (n=234), duodenal ulcer (n=315), combined gastric and duodenal ulcer (n=47), and stomach cancer (n=5) (Table 4). The eradication rates of H. pylori from 2005 to 2010 were 89.3%, 82.6%, 86.3%, 87.7%, 81.8%, 84.2%, respectively. Total eradication rate was 84.9%, and there was no statistical difference between eradication rates by year (Fig. 3).
PCR Amplification and Sequence Analysis of the 23S rRNA Gene for Mutations that Result in Clarithromycin Resistance
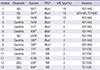
Only 14 of the 18 clarithromycin-resistant strains were evaluated due to technical difficulties associated with the H. pylori culture. The A2144G mutation in the 23S rRNA gene was detected in 8 of the 14 clarithromycin-resistant strains (57.1%) by BsaI digestion of the PCR products (Fig. 4); the PCR products of these strains were not digested with BbsI, revealed a A-to-G mutation at position 2144 (A2144G) (Fig. 4). Sequencing of 5 clarithromycin-resistant strains (35.7%), whose PCR products were not digested by BsaI and BbsI, revealed a T-to-C mutation at position 2183 (T2183C). Sequencing of 1 strain whose PCR product was digested by BsaI revealed A2144G and T2183C mutations (7.1%) (Fig. 4). The MICs for the A2144G mutant strains ranged from 2 to 16 µg/mL (Table 5). The MICs for the T2183C mutants were relatively low (MICs=2 µg/mL).
DISCUSSION
The National Committee for Clinical Laboratory Standards (NCCLS) has not established an official breakpoint for amoxicillin resistance in H. pylori isolates. Nevertheless, many reports have provisionally defined the cut-off value as an MIC higher than 0.5 µg/mL (11, 12). In the present study, the prevalence of amoxicillin resistance was 9%. This rate was found to be similar to that (9.1%) found in H. pylori isolated from 99 Koreans who lived in Gyeonggi, Kangwon province and Busan in 2008 (12).
The prevalence of clarithromycin MICs>1 µg/mL was 8.5% in our study. This rate was higher than that (5.1%) reported from our hospital in 2001 (10). The prevalence of clarithromycin resistance in H. pylori strains isolated from Korean patients in Seoul National University Hospital increased from 2.8% (MICs≥1 µg/mL) in 1994 to 13.8% (MICs≥1 µg/mL) in 2003 to 32.5% (MICs>1 µg/ml) in 2008 (3, 12). Moreover, there were differences in the rates of resistance to clarithromycin in 3 institutes located in Gyeonggi (32.5%), Kangwon province (12.5%), and Busan (42.1%), even though, by post-hoc analysis, there was no statistically significant difference between the rates in the 3 regions (12). These results may suggest both a tendency towards increasing resistance and regional differences in resistance to clarithromycin. The clarithromycin resistance rate found at Hallym University Chuncheon Hospital in Kangwon province was closer to our result. Our institute is a localized secondary referral hospital, but Seoul National University Hospital is a national referral institute. Therefore, the antibiotic resistance rates observed in our institute may be lower than those observed in the Seoul National University Hospital. The threshold of resistance at which clarithromycin should not be used, or a clarithromycin susceptibility test should be performed, is 15%-20% (13). The Maastricht IV/Florence Consensus Report recommends that PPI-clarithromycin-amoxicillin or metronidazole regimens be used as first-line therapy in populations with less than 15-20% clarithromycin resistance (13). Therefore, clarithromycin based triple therapy could be used as the first-line therapy in our hospital.
The NCCLS has not designated an official breakpoint for metronidazole resistance in H. pylori isolates. The prevalence of metronidazole MICs >8 µg/mL in H. pylori isolated from our institute was 54.4% in 2001 (10). Metronidazole is widely prescribed for infections (e.g., parasitic or those of the female genitourinary tract) in Korea, and the growing use or abuse of this inexpensive drug may have contributed to the elevated MICs. In the present study, the prevalence of metronidazole resistance was 36.3%. A recent multicenter study has shown a decreased resistance rate (19.2%) (12). Although sample size, technical problems with the agar dilution test, regional differences, and socioeconomic status may account for these differences, the recent H. pylori resistance to metronidazole in Korea is reduced as compared to that reported by previous studies (10, 12). The Maastricht III Consensus Report recommends treatment with PPI-clarithromycin-metronidazole in populations with less than 40% metronidazole resistance (14); however, metronidazole may still be less effective in Korea due to the relatively high resistance rate.
Primary resistance to tetracycline is rare. We used a recent provisional breakpoint of >4 µg/mL and found no tetracycline resistant strain (0%). These results contrast sharply with the resistance rates of 12.3% (MICs≥4 µg/mL) in 2003 and 15.2% (MICs>4 µg/mL) in 2008 (12). Thus, further study is necessary to clarify tetracycline resistance in Korean patients.
Fluoroquinolones have been proposed as components of triple PPI-based regimens (4, 5). In particular, fluoroquinolones have been used in second-line therapy for H. pylori eradication in Korea (5). The NCCLS has not designated an official breakpoint for fluoroquinolone resistance in H. pylori isolates; however, a provisional breakpoint of >1 µg/mL has been proposed (9, 12). We found resistance rates to be 14.2% for ciprofloxacin, moxifloxacin, and levofloxacin on the basis of this breakpoint. This rate is lower than 21.5% (MICs≥1 µg/mL) found in 2003 and 23.2% (MICs>1 µg/mL) found in 2008 (9, 12).
In the present study, 35 of 212 H. pylori strains (16.5%) exhibited MDR to 2 or more antimicrobial agents. This rate was lower than that (47.7%) for H. pylori isolated from Korean patients in 2003 (15). The resistance rate (0.9%) to both amoxicillin and clarithromycin was much lower than that (6.2%) of H. pylori isolated from Korean patients in 2003 (15). The eradication rate of H. pylori was about 85% according to data from our institute that was collected from 2005 to 2010 (Fig. 3). And P for trend of eradication rate by year did not show statistical difference (P=0.516). On the basis of these results, the clarithromycin-based triple therapy that includes amoxicillin and clarithromycin may still be an effective regimen against H. pylori in some parts of Korea. These results may be appear to contrast to that of other studies that show high H. pylori resistance rate to clarithromycin and low eradication rate. However, there are several reports that the prevalence rates of antibiotic resistance in H. pylori have varied widely according to geographical regions (16, 17). There is Korean report concerning institutional difference of antibiotic resistance of H. pylori strains (18). Hallym University Chuncheon Hospital in Kangwon province reported the similar H. pylori resistance rate to clarithromycin. However, several institutes reported higher H. pylori resistance rate. The variety of eradication rate according to region was reported in Korea (20, 21, 22). A Korean study recently performed by Kim et al. (24) in 2011 showed high eradication rate (89.2%). Therefore, regional differences in antibiotics resistance and eradication rate may be present in Korea. In future, large well conducted nationwide study should be designed to investigate regional differences in antibiotics resistance.
Clarithromycin is one of the most useful antibiotics for treating H. pylori infections. Therefore, early detection of clarithromycin resistance before treatment is very important. Evaluation of 23S rRNA mutations in clarithromycin-resistant H. pylori was suggested to detect of clarithromycin resistance before treatment. After 23S rRNA mutations in clarithromycin-resistant H. pylori were first reported (23), point mutations (A to G at 2,143 and 2,144) were subsequently confirmed by other investigators (6, 24). Moreover, the A2142G mutation has been reported (25) along with several other rare mutations such as A2143C (24), T2183C (10), T2717C (26), and T2182C (27). Additionally, both A2116G and A2142G have been reported (28). These mutations reduced the affinity of clarithromycin for the 23S ribosomal component, resulting in impaired activity against H. pylori (3).
In the present study, the A2144G mutation in the 23S rRNA gene was detected in 8 of 14 clarithromycin-resistant strains (57.1%). Sequencing of 5 clarithromycin-resistant strains (35.7%), of which PCR products were not digested with BsaI or BbsI, revealed a T-to-C mutation at position 2183 (T2183C). Sequencing of a strain whose PCR products were digested with BsaI revealed both A2144G and T2183C mutations (7.1%). Mutations such as T2183C and T2245C are generally do not contribute to drug resistance (6). However, our study showed T2183C mutations in clarithromycin-resistant H. pylori strains.
In summary, antibiotic resistance rates in the present study were appropriate for the use of a clarithromycin based triple therapy for the eradication of H. pylori. An A2144G mutation was present in the 23S RNA gene of clarithromycin-resistant bacteria. Moreover, a T2183C mutation was shown in clarithromycin-resistant H. pylori, and the observation of 1 double mutation can be of interest for further studies. Therefore, we conclude that a clarithromycin based triple therapy that includes clarithromycin is a still effective eradication therapy against H. pylori infections in some parts of Korea. Nationwide surveillance of antibiotic resistance is important for evaluating the growing problem of antibiotic resistance.




 XML Download
XML Download