

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intraoperative hypothermia is common because anesthetics impair thermoregulatory control (1, 2). This effect is associated with adverse outcomes including impaired coagulation (3), increased incidence of surgical wound infections, prolonged hospitalization (4), and myocardial ischemia (5). Despite the absence of environmental exposure of a wound or abdominal viscera, hypothermia has been reported to occur during laparoscopic surgery (6, 7). Exposure of the abdominal cavity to large volumes of cold, dry carbon dioxide gas used for insufflation has been implicated as a potential source of heat loss during laparoscopy (6, 7, 8).
Theophylline is an active stimulant metabolite from caffeine. Therefore, the effects of aminophylline (85% theophylline, 15% ethylendiamine) are similar to those of caffeine. Aminophylline has been shown to elicit thermogenesis and improve cold tolerance in rats (9, 10) and increase the metabolic rate in lambs during cold stress (11).
Since there have been no reports on the thermogenic effects of aminophylline in humans, we tested the hypothesis that aminophylline reduces the decrease in core body temperature during laparoscopic vaginal hysterectomy (LVH) requiring pneumoperitoneum.
MATERIALS AND METHODS
This was a prospective, randomized, blinded clinical trial. After obtaining written informed consent from all patients, fifty patients scheduled for elective LVH were enrolled between 40 to 60 yr of aged with American Society of Anesthesiologists (ASA) physical status I or II. Patients with a history of cardiovascular, pulmonary, or thyroid disease; dysautonomia; fever; aminophylline intake within a day before surgery; or who were transfused were excluded from this study.
The patients were randomly divided into an aminophylline group (n=25) and a saline control group (n=25) using a computer-generated randomization list. The ambient operating room (OR) temperature was maintained around 21℃ (12). No premedication was given. Upon arrival in the operating room, standard anesthetic monitors were applied, including ECG, a non-invasive blood pressure monitor, and pulse oximetry. To evaluate the depth of anesthetization, BIS monitor (A-3000 BIS monitor, Aspect Medical System, Covidien, MA, USA) sensors (BISTM Quatro, Aspect Medical System, Norwood, MA, USA) were attached to the patient's forehead and temple. A skin temperature probe was attached to the index finger of the non-infused arm. After induction, a urinary catheter was inserted to measure hourly urine output.
To prepare the study drug, aminophylline (10 mg/kg) was mixed with saline in a syringe to a volume of 100 mL by an independent researcher. Saline alone (100 mL) was used as a control. Fifteen minutes before inducing anesthesia, 10 mL (1 mg/kg) of the study drug was administered intravenously over 1 min as an initial infusion. An esophageal temperature probe was inserted into the lower esophagus immediately after intubation in order to measure the core temperature. The remaining 90 mL of the study drug was administered intravenously at a rate of 50 mL/hr for next 108 min using a syringe pump.
Induction was accomplished with fully preoxygenation, 1% lidocaine 40 mg and 1% propofol 2 mg/kg, followed by rocuronium 0.6 mg/kg. Anesthesia was maintained with 1-3 vol% of sevoflurane and 2 L/min each of nitrous oxide and oxygen to obtain BIS values between 45 and 55. The lungs were ventilated with a tidal volume of 7-10 mL/kg and a respiratory rate of 8-12 breaths/min to maintain an end-tidal carbon dioxide (ETCO2) value between 30 and 35 mmHg. The pneumoperitoneal pressure was maintained at 12 mmHg to decrease the risk of venous carbon dioxide embolism. The average temperature of inflow gas was 21℃, and the temperature of the outflow was 32℃. The tidal volume and respiratory rate were set to maintain an ETCO2 between 35-40 mmHg after pneumoperitoneum. None of the fluids were warmed but were maintained at room temperature. When the systolic blood pressure fell below 80 mmHg, 5 mg i.v. ephedrine was given slowly, and additional doses were given at 10 min intervals, as needed. Lactated Ringer's solution and 6% hydroxyethyl starch in normal saline (NS) solution (Voluven™, Fresenius Kabi, Bad Homberg, Germany) were administered at a maximum dose of 50 mL/kg. Lactated Ringer's solution was infused at a constant rate of 6 mL/kg/hr. Body temperature was measured in the post-anesthesia care unit (PACU) using a tympanic thermometer (ThermoScan IRT 1020, Braun, Germany). In the PACU, a Bair Hugger forced-air warmer (Augustine Medical Inc., Eden Prairie, MN, USA) was applied to patients who had a tympanic temperature below 36℃.
The skin temperature, mean blood pressure, and heart rate were recorded 15 min before inducing anesthesia (T-15), immediately after intubation (Tintu), and at 15 min intervals (T15-T105) after intubation. Esophageal temperature was recorded immediately after intubation (Tintu) and at 15 min intervals (T15-T105) afterward. The room temperature, fluid intake, urine output, and estimated blood loss were recorded at T105.
To estimate the sample size needed, a pilot study was conducted measuring core body temperature of ten control patients. The standard deviation of core body temperature at T15 was 0.34. For the power calculation, we assumed an equal standard deviation for the aminophylline infusion group. A sample size of 22 patients per group provided 80% power with a two-tailed α=0.05 to show a difference of 0.3℃ between groups. To compensate for an estimated dropout rate of 10%, 25 patients per group were recruited.
Data are expressed as mean and SD. Continuous data within the groups, such as temperature and hemodynamic variables, were compared with repeated measures of ANOVA followed by paired t-tests with Bonferroni correction for multiple comparisons. Student's t-test or Chi-square test was used to compare variables between the groups, where appropriate.
In all tests, P<0.05 was considered significant.
Ethics statement
The study protocol was approved by the institutional review board for human research at the Catholic University of Korea St. Vincent Hospital, Suwon, Republic of Korea (VC12OISI0078). The nature of the study was explained to all patients, each of whom provided written informed consent before the beginning of the study, in accordance with the principles of the Declaration of Helsinki (revision of Edinburgh, 2000).
RESULTS
The patient characteristics and perioperative data are listed in Table 1. Patient characteristics and perioperative data, including room temperature, fluid intake, urine output, and blood loss, did not differ significantly between the groups.
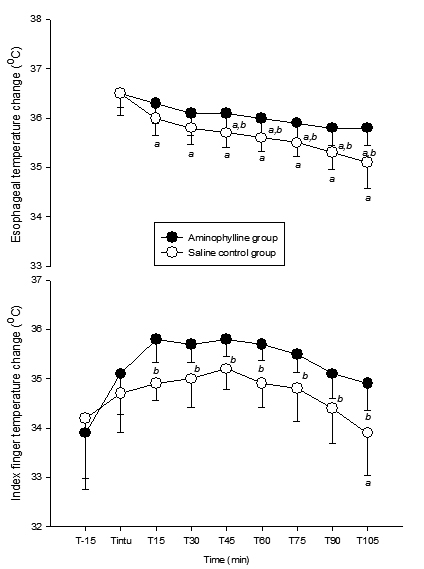
In the aminophylline group, esophageal temperatures at T45, T60, T75, T90, T105 (P values are in the order of 0.024, 0.053, 0.025, 0.011, 0.017) and index finger temperatures at T15, T30, T45, T60, T75, T90, T105 (P values are in the order of 0.001, 0.029, 0.020, 0.010, 0.028, 0.042, 0.024) were significantly higher than in the saline control group (Table 1) (Fig. 1). The esophageal temperatures decreased significantly from Tintu at T15-T105 in the saline control group (P values were in the order of 0.040, 0.006, <0.001, <0.001, <0.001, <0.001, <0.001) and at T45-T105 in the aminophylline group (P values were in the order of 0.039, 0.011, 0.002, <0.001, <0.001) (Fig. 1). The index finger temperature at T105 in the saline control group decreased significantly from Tintu (P=0.045) (Fig. 1).
Heart rates in both groups were significantly higher at Tintu than at T-15 (P=0.025 in the saline control group, P=0.014 in aminophylline group). Mean blood pressures in the aminophylline group were significantly lower at T45-T105 than at T-15 (P<0.001) (Fig. 2).
DISCUSSION
This study demonstrated that an aminophylline infusion reduced the changes in core and skin temperature compared to a saline control during LVH requiring pneumoperitoneum. Aminophylline, like caffeine, is a methylxanthine that has been shown to elicit thermogenesis and improve cold tolerance in rats (9, 10). It has also significantly improved cold tolerance in lean Sprague-Dawley rats, regardless of age or thermogenic capacity. Aminophylline (18.7 mg/kg intraperitoneal) significantly improved thermogenesis and cold tolerance in both lean and corpulent rats without any age-related difference (13). Zimmermann et al. (11) reported that aminophylline has potential as a treatment for hypothermia or to improve recovery from hypothermia in lambs by increasing metabolic rate during cold stress at 16 and 32 mg/kg doses.
Vestal et al. (14) reported that methylxanthine derivatives, such as caffeine and theophylline, stimulated epinephrine and norepinephrine release from the sympathoadrenal system. In six healthy males, a 262% increase in plasma epinephrine and a 64% increase in plasma norepinephrine during a high-dose infusion of theophylline (plasma theophylline level of 20 µg/mL) resulted in dose-dependent cardiovascular and metabolic effects. Plasma concentrations of glucose and free fatty acids (FFAs) also increased, but insulin secretion was inhibited (14). Caffeine (15) and aminophylline also block adenosine receptors (16), which is an effect that may have a greater impact on metabolism than the inhibition of phosphodiesterase (17). The combined effects are expected to enhance lipolysis, glycogenolysis and gluconeogenesis and hence contribute to enhanced maximal thermogenesis (10).
After anesthesia is induced, core hypothermia is largely caused by a redistribution of body heat from the core to the periphery (1). Most anesthetics cause arterial and venous dilation as well as thermoregulatory vasodilation in the arteriovenous shunt (18, 19). Ikeda et al. (20) stated that hypothermia during general anesthesia develops in three distinct phases: 1) an initial, rapid decrease in core temperature, resulting largely from an internal core-to-peripheral redistribution of body heat; 2) a slower, linear decrease in core temperature that results from heat loss exceeding metabolic heat production (21); and 3) a core-temperature plateau resulting from decreased cutaneous heat loss (22) and metabolic heat constrained to the core thermal compartment in patients becoming sufficiently hypothermic to trigger thermoregulatory vasoconstriction (23).
In this study, the core temperature gradients in the aminophylline group during sevoflurane anesthesia decreased significantly less than in the saline control group. Skin temperature gradients followed a similar trend. These data suggest that aminophylline effectively maintained the core temperature through a thermogenic effect despite reduced peripheral thermoregulatory vasoconstriction.
Since there are no data on the thermogenic effect in humans, we cannot determine the therapeutic range of aminophylline infusion doses. Zimmermann et al. (11) reported that, in lambs, a dose of more than 16 mg/kg of aminophylline can improve recovery from hypothermia by increasing metabolic rate during cold stress, whereas 8 mg/kg of aminophylline did not affect metabolic rate. Although this was the first study to report the thermogenic effect of aminophylline in humans, we hoped positive results. Therefore, we chose an aminophylline dose high in the therapeutic range (10 mg/kg). The optimal dose should be determined in further investigation. For safety, 1 mg/kg of aminophylline was administered as an initial infusion at 15 min before inducing anesthesia, and the remaining 9 mg/kg was administered intravenously after intubation at a rate of 50 mL/hr for 108 min using a syringe pump.
This study had some limitations. One limitation is the lack of a preoperative esophageal temperature. An esophageal temperature probe was not inserted before inducing anesthesia to ensure patient comfort. Another limitation is that the study was performed only in women that underwent laparoscopic gynecologic surgery requiring pneumoperitoneum. Other types of surgeries in both sexes should be investigated further.
In summary, this is the first study to report the thermogenic effect of aminophylline in humans. We found that an intraoperative infusion of aminophylline reduced the decreases in core and skin temperature during LVH requiring pneumoperitoneum. These data suggest that aminophylline maintains core temperature through a thermogenic effect despite reduced peripheral thermoregulatory vasoconstriction. Aminophylline, therefore, may be a useful and supplemental thermogenic agent to prevent hypothermic conditions when limited facilities are available to provide supplemental heat.



 XML Download
XML Download