

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lower urinary tract symptoms (LUTS) manifest multiple domain of clinical symptoms such as storage, voiding and post-micturition and are common among older men (1). Of the various etiologies and clinical symptoms associated with LUTS, benign prostatic hyperplasia (BPH) is considered a primary cause and also closely resembles its symptoms, although a clear relationship is not fully understood between LUTS and BPH (1,2,3).
The underlying pathophysiologies of LUTS/BPH are currently uncertain but it has been considered a subjective indicator of disease, not a confirmative formal diagnosis (4). According to a recent huge cross-sectional population-based study, the negative effects of LUTS/BPH were prominent across several domains of quality of Life (QoL) and on overall perceptions of general health status and mental health (5, 6). In addition, the clinical course of LUTS/BPH is chronic, recurrent and difficult-to-treat. According to the recent large catchment area study with 5-yr follow-up for natural history of LUTS (n = 5,502) (7), the prevalence of LUTS increased from 19% at baseline to 20% at follow-up. In particular, only less than half (43%) of those with moderate to severe LUTS at baseline remitted or become mild LUTS at follow-up; most men with severe LUTS at baseline continued to have severe LUTS (61.5%) at follow-up.
However, the treatment response with such medications is not satisfactory. A recent treatment guideline also suggests the weak efficacy of such medications, where approximately 20%-50% reduction in LUTS/BPH symptoms are common after treatment of monotherapy of α-receptor blockers and 5α-reductase inhibitors based on results from a number of short-term and long-term clinical trials (8, 9).
Meanwhile, it was found that the clinical manifestation of LUTS/BPH is strongly associated with psychiatric disturbances such as depression, anxiety, and stress vulnerability, and impairments of instrumental activities during daily living in some studies (5, 10, 11, 12, 13, 14, 15, 16, 17). For instance, the recent large cohort study (14) have also demonstrated the important relationship between LUTS/BPH and depression, in which depression was significantly associated with the severity of the diseases as well as it also involves in all stages of LUTS. According to a large observational, longitudinal, multicenter study (n=666), a substantial proportion (22.6%) of LUTS/BPH patients reported anxiety or depression and they also explained a 7% of variance for explaining the severity of LUTS/BPH. Likewise in a large population-based study (EpiLUTS, n=30,000) (5), approximately 36% and 30% of men were found to report anxiety and depression, respectively. Pre-existing study results consistently suggest that putative role of psychiatric parameters in the development of LUTS/BPH and also proposes that the current treatment for LUTS/BPH may not fully ameliorate urinary issues if the underlying psychiatric disturbances are not properly resolved (18).
Taken together, a high level of psychiatric morbidity has important implications for the appropriate management in patients with of LUTS/BPH and warrants further in-depth studies in terms of potential relationship between psychiatric symptoms and treatment reponse in patients with LUTS/BPH (5). However, there has been a paucity of clinical data regarding a potential influence of such psychiatric disturbances on the treatment outcomes in patients with LUTS/BPH till today.
Therefore, the aim of this study was to investigate the potential influences of depression, anxiety and somatisation on the treatment response in patients with LUTS/BPH with the use of brief, user-friendly and quick but validated rating scales since timely and proper measurement of such psychiatric parameters may help identify individuals more likely to benefit from treatment interventions in daily busy routine practice.
MATERIALS AND METHODS
Subjects
Male patients with LUTS/BPH were recruited at an outpatient clinic in the Department of Urology at Bucheon St. Mary's Hospital.
Principal inclusion criteria included men aged ≥40 yr, a clinical diagnosis of LUTS/BPH was evaluated by medical history, a careful physical examination and laboratory tests including prostate-specific antigen (PSA) levels. Few exclusion criteria were applied because the aims of the study were based on observational approach. However, patients who exhibited the following symptoms were excluded for diagnostic stability: 1) PSA level>10 ng/mL, 2) a history or evidence of prostate cancer by prostate biopsy, 3) previous prostatic surgery, 4) any causes of LUTS other than BPH (i.e., neurogenic bladder, bladder neck contracture, urethral stricture, bladder malignancy, acute or chronic prostatitis, or acute or chronic urinary tract infections), and 5) speech or language deficits and cognitive dysfunction.
The study was a 12-week prospective observational design in a naturalistic treatment setting. Alpha-blockers, 5-alpha-reductase inhibitors or combination of both were the primary treatment utilised for the patients during the study. Throughout the study period, patients remained on the same medication and the same dosage as was given at the time of enrolment.
Rating scales
All the rating scales were examined at baseline and week 12. The Korean versions of the International Prostate Symptom Score (IPSS) for severity of LUTS/BPH (19), the Patient Health Questionnaire-9 (PHQ-9) for depression (20, 21), the Patient Health Questionnaire-15 (PHQ-15) for somatization (22, 23) and the 7-item Generalized Anxiety Disorder Scale (GAD-7) (24) for anxiety, were utilized in the study. The criteria for depression (≥5 on PHQ-9) (20), anxiety (≥5 on GAD-7) (24) and somatisation (≥5 on PHQ-15) (22) were defined by previous studies suggested.
Treatment outcomes
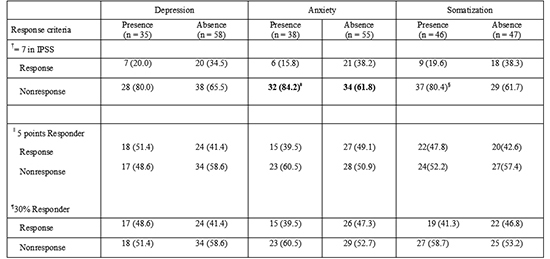
The primary endpoint of the study was a responder rate defined by the total score of IPSS (≤7) at the end of treatment (week 12). The 7 point response criterion was chosen since the IPSS total score of 7 indicates no or mild symptoms of LUTS/BPH.
Secondary endpoints included the changes in total scores and three sub-scores on the storage, obstruction, and QoL domains of the IPSS from baseline to week 12. Other responder analyses by different criteria included as follows: 1) ≥5 points and 2) ≥30% decrease from baseline to week 12 in IPSS total score from baseline to week 12 (25, 26). In LUTS/BPH clinical trials, regarding point decrease with IPPS total score, the 4 to 6 points decline was common and 3 points decrease was proposed to be the minimum for clinical benefit (26). Regarding % improvement of IPSS total score from baseline, 25% and 30% reductions in IPSS total score were mostly utilized. However, none of point decrease or % reduction in IPSS total score has been validated as established response criteria, they were usually empirically used by individual research group. Hence, we have also empirically chosen the 5 point decrease and 30% improvement of IPSS total score as another potential response criteria.
Statistical analyses
Demographic variables were compared by the presence of depression, anxiety and somatization using Student's t-test, a chi-square test with Yate's correction, or Fisher's test, as appropriate. To investigate the influence of each clinical parameter on various treatment outcomes, changes of individual rating scales from baseline to week 12 were analyzed using an analysis of covariance (ANCOVA) controlling for age, duration of disease and type of medication. To analyze responders as defined a priori, Fisher's exact tests were conducted. Odds ratio (OR) with 95% confidence intervals (CIs) was also utilized for the responder analysis as well.
Statistical significance was two-tailed and set at P<0.05 and there was no adjustment for multiple comparisons because the sample size was relatively small. With these statistical parameters and after adjusting with covariates, the power of the sample to detect a medium effect size (d=0.5) was 0.6108, which corresponds to a difference of 2.6 in the mean changes of IPSS total scores between patients with depression and those without. All statistical analyses were conducted using the NCSS 2007® and PASS 2008® software (Kaysville, Utah, USA).
RESULTS
Baseline demographic characteristics
Ninety three patients participated in the study. The mean age of the whole population was approximately 62 (61.7±8.0) yr, and the majority of patients were married. More than half of patients exhibited comorbid medical diseases. The mean total score on the IPSS among all groups was approximately 17, indicating a moderate severity of LUTS/BPH symptoms. The mean volume of prostate (PV) and peak flow rate (Qmax) were 36.8±15.5 mL and 13.3±1.9 mL/sec, respectively; however, PV and Qmax were not significantly different by presence of depression, anxiety and somatization (Table 1). In addition, the PV and Qmax were not significantly different as criteria of responders and non-responders: 1) 33.2±16.2 mL vs. 38.3±15.0 mL and 13.5±1.3 mL/sec vs. 13.3±2.1 mL/sec, respectively, by IPSS at endpoint (≤7); 2) 38.2±15.3 mL vs. 35.6±15.8 mL and 13.1±1.7 mL/sec vs. 13.5±2.1 mL/sec, respectively, by IPSS decrease from baseline (≥5) and 3) 36.6±14.2 mL vs. 36.9±16.5 mL and 13.4 ±1.3 mL/sec vs. 13.3±2.3 mL/sec, respectively, by IPSS decrease from baseline (≥30%).
Depression subgroup
There were no group differences in demographic variables such as education level, family history of LUTS/BPH, economic status, comorbidity, alcohol history, smoking history, or marriage status between the two groups (data available on request). The LUTS/BPH total score was significantly higher in patients with depression than those without (18.5 vs. 15.3, P=0.046). In the sub-symptom analysis, the storage sub-symptom was also significantly higher in patients with depression than in those without (7.6 vs. 5.8, P=0.021). However, all the treatment outcomes were not different between the two groups (Tables 2, 3).
Anxiety subgroup
There were no group differences in demographic variables such as education level, family history of LUTS/BPH, economic status, comorbidity, alcohol history, smoking history, or marriage status between the two groups (data available on request). The LUTS/BPH total score was not different between the two groups. QoL sub-score was significantly higher in patients with anxiety (3.8 vs. 3.2, P=0.038) than in those without. Anxious patients showed significantly higher proportion of non-response (OR, 3.294, P=0.022) than those without in primary endpoint analysis (Tables 2, 3).
Somatization subgroup
There were no group differences in demographic variables such as education level, family history of LUTS/BPH, economic status, comorbidity, alcohol history, smoking history, or marriage status between the two groups (data available on request). The LUTS/BPH total score was significantly higher in patients with somatization than in those without (18.3 vs. 14.7, P=0.024). In addition, obstruction and storage sub-scores were in a trend toward a significant difference between the two groups (11.2 vs. 8.9 and 7.3 vs. 5.8, respectively, P=0.050 and P=0.050, respectively). There were no differences in all the treatment outcomes, although a trend toward a significant difference was found in primary endpoint analysis (P=0.067) (Tables 2, 3).
DISCUSSION
Our preliminary results suggest that depression, anxiety and somatization may have partly influences on the clinical manifestation of LUTS/BPH. Further, anxious patients had a lower response to treatment in patients with LUTS/BPH. The most strength of our study is to assess the relationship of depression, somatisation and anxiety with treatment response in patients with LUTS/BPH for the first time, especially with the use of simple, quick, reliable, well-validated, and self-administered rating scales which are easy to administer and interpret even in busy routine practice. However, the PV and Qmax were not significantly different by presence or absence of depression, anxiety, and somatization.
A common neurochemical underpinning may be speculated to be attributable to depression/anxiety/somatization and bladder function. A compelling association between central and peripheral serotonin (5-HT)/norepinephrine (NE) systems and lower urinary tract function has been consistently proposed (27). In fact, duloxetine (serotonin/norepinephrine reuptake inhibitor, SNRI) has been approved for the treatment of urinary incontinence in Europe in 2004. It has been found to increases bladder capacity and urethral sphincter electromyographic activity in an animal model, which is mediated by increases in extracellular 5-HT or NE (28). In addition, the reduction of 5-HT developed urinary frequency and caused detrusor over-activity, which was successfully reversed by fluoxetine the selective serotonin reuptake inhibitor (SSRI) (29). Other studies (30) also suggest that the role of 5-HT in urinary function; 5-HT reuptake transporter knockout mice (-/-) demonstrated a bladder dysfunction, characterized by significant increases in the frequency of spontaneous non-voiding bladder contractions and decreases in voiding volume. It was also found that the predominant effect of NE release from sympathetic nerve terminals is on urethral contraction mediated through α1- and α2-adrenergic receptors (31, 32, 33). Therefore antidepressants such as SNRIs as well as SSRIs could be considered to enhance urine storage by decreasing bladder contractility and increasing outlet resistance. In addition, the crucial role of serotonin and norepinephrine has been very-well known in the development and management of depression, anxiety and somatization, which are effectively controlled by SNRIs (34). In fact, depression, anxiety and somatisation have been found to impact on self-perception, treatment compliance, coping strategies and clinical status in a various mental health and physical diseases. Taken together, we may deliberately speculate that depression/anxiety/somatization and LUTS are all linked with major neurotransmitters, 5-HT and NE, and that thereby these psychiatric symptoms may play a role in the development of clinical symptoms and treatment outcomes in patients with LUTS/BPH.
Differential associations between psychiatric symptoms and LUTS were found in male patients in a previous study (5), where depression was more associated with storage and post-micturition in male patients (5). Likewise the present study also found the association of storage symptoms and depression, supporting the previous finding that depressed patients may have more bother in urinary frequency.
Many previous studies have replicated lower QoL in patients with LUTS/BPH were prominent across several domains of quality of Life (QoL) and on overall perceptions of general health status and mental health, especially accompanied by depression/anxiety. Likewise, we also found a significant association of anxiety with QoL in the present study, although depression did not show such relationship. This slight discrepancy may be caused by different sample characteristic, sample size, different measurement of depression and so on. Our findings partly support the pre-existing study results.
The presence of anxiety and improvement of anxiety was significantly associated with the non-response in the present study, indicating that clinicians may benefit in expectation of future response in clinical practice if they know the level or improvement of anxiety. Our results are in line with the previous findings that anxiety may be involved as a risk factor in the severity and progression of LUTS/BPH (5, 16, 35).
An increasing evidence suggests the possibility that for some patients with LUTS/BPH (18, 35), CP/CPPS (36, 37) and urinary incontinence (38), urinary symptoms could be part of a somatizing process and requires further consideration (35). In fact, previous studies have consistently reported that the worse physical health ratings are significantly associated with more bother in patients with LUTS/BPH, indicating that measures of urinary bother capture somatic distress should be necessary and that treating LUTS/BPH alone may not completely ameliorate urinary bother if underlying such somatic concerns are not addressed (35).
Our preliminary study has a number of limitations and also implicates future study direction. First, the small sample size may be insufficient to detect such relationship between personality and symptom severity of LUTS/BPH. Currently, there are no large and unselected population-based studies that have utilised the PHQ-9, PHQ-15, and GAD-7 on patients with LUTS/BPH, and thus, the current results are entirely exploratory. The use of brief self-rating scales may be one of strength to be utilized in busy clinical practice but also could be a critical limitation; we propose to use of both subjective and objective rating scale to verify depression, anxiety and somatization as well as including some assessment of current burden of stress. The study period was only 3 months and thus we do not know the long-term effects of such psychiatric parameters on the clinical course and treatment response. An additional dilemma for clinical researchers is whether to correct for multiple comparisons. We did not perform multiple comparison correction in the present study due to the nature and small sample size of the study. The Bonferroni correction is the most popular way to correct for the multiple testing issue, but its utility may depend on the nature of the study. According to Streiner and Norman (39), correction of multiple testing can be waived if a small number of hypotheses have been stated a priori or if the purpose of the study is exploratory (preliminary), and this is also in agreement with the assertions of other researchers (40). Finally, the sample was only recruited in one teaching hospital and may not represent the general LUTS/BPH population.
In conclusion, the present study preliminarily demonstrates that clinicians may need careful evaluation of depression, anxiety and somatization issues for the proper management of patients with LUTS/BPH, despite study limitations. Subsequent studies with adequately-powered and better design may be crucial to validate and support the present exploratory study findings.


 XML Download
XML Download