

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of diabetes mellitus in patients with liver cirrhosis is higher compared to that in the general population. The prevalence of diabetes has been reported to be between 30% and 70% depending on the etiology, the severity of liver disease, and the diagnostic criteria (1, 2). Nonalcoholic fatty liver disease (NAFLD), chronic hepatitis C (CHC), hemochromatosis, and alcoholic liver disease (ALD) are regarded as major chronic liver diseases associated with diabetes (2). The prevalence of diabetes was reported to be between 21% and 45% in NAFLD (3), between 17% and 33% in CHC (1, 4), between 50% and 85% in advanced hemochromatosis (1), and 18% in ALD (5), respectively. The relationship of diabetes with chronic hepatitis B (CHB) is uncertain (6, 7, 8), although the prevalence of diabetes increases in patients with hepatitis B-related liver cirrhosis (2). The relationship of diabetes in patients with chronic liver disease can be explained by the simultaneous occurrence of the following two abnormalities: an inadequate secretion of insulin due to decreased response of the beta-cells and insulin resistance in muscle and adipose tissue (1).
Many studies have reported the association between liver cirrhosis or steatosis and diabetes. However, most of the previous studies were small-scale studies where liver biopsy was performed to measure the degree of liver fibrosis or steatosis. Liver biopsy has been regarded as the gold standard for the assessment of fibrosis or steatosis. However, a biopsy sample represents only 1/50,000 of the total liver volume, and therefore biopsy has its limitation in accurate assessment of the whole liver. Moreover, it has a limited use because of possible complications due to its invasive nature (9). Regarding the relationship between steatosis and diabetes, several large-scaled studies have used abdominal ultrasonography to assess fatty liver change. However abdominal ultrasonography has a limitation to assess the degree of fatty liver because of the subjective interpretation by sonographers (10, 11, 12, 13).
Recently, transient elastography has been emerging as a relevant tool for assessing hepatic steatosis as well as hepatic fibrosis. In transient elastography, liver fibrosis is indicated by liver stiffness measurement (LSM), and steatosis, by controlled attenuation parameter (CAP) score (14, 15, 16, 17). Several meta-analyses have demonstrated the usefulness of transient elastography: sensitivity of 87%, and specificity of 91% for the diagnosis of liver cirrhosis (14). In addition, CAP score in transient elastography has been shown to be significantly correlated with the grade of steatosis in several studies (15, 16, 17). Transient elastography has several advantages; it is quick, inexpensive, reproducible, and noninvasive and it can sample about 100 times larger portion of liver tissue than liver biopsy (16, 18).
We aimed to evaluate the relationship of hepatic fibrosis and steatosis assessed by transient elastography with diabetes mellitus in patients with chronic liver disease, especially CHB.
MATERIALS AND METHODS
Study population
The study population consisted of 1,383 patients who underwent transient elastography from August 2012 to March 2013 at Samsung Medical Center, Seoul, Korea. Among these patients, those who had one of the following 4 etiologies of liver disease were included; CHB, CHC, ALD, and NAFLD. Exclusion criteria were as follows: 1) alanine aminotransferase (ALT) level>2 x upper normal limit; 2) total bilirubin (TB)>1.5 mg/dL; 3) interquartile ratio (IQR)/median of both LSM and CAP score >0.3; 4) miscellaneous other etiologies of liver disease; 5) overlapping etiologies; 6) lack of data. After exclusion, a total of 979 patients were analyzed in the study.
Assessment of lifestyle and biochemical parameters
At the time of performing transient elastography, information regarding alcohol consumption (quantity and frequency), smoking (none, past, current, pack-years), exercise (time, frequency), and comorbidity (hypertension, hypercholesterolemia, diabetes mellitus) was collected through questionnaires. The body mass index (BMI) for each patient was calculated as body weight in kilograms divided by height in meters squared (kg/m2).
Laboratory examination including aspartate aminotransferase (AST), ALT, TB, triglyceride (TG), fasting plasma glucose, and hemoglobin A1c (HbA1C) was performed after an 8 hr overnight fast.
Diagnosis of diabetes mellitus
Diagnosis of diabetes mellitus was made if this condition was previously diagnosed by a physician or if the fasting plasma glucose level was greater than or equal to 126 mg/dL or HbA1C was greater than or equal to 6.5% on at least 2 occasions according to the 2011 American Diabetes Association (ADA) criteria (19).
LSM and CAP assessed by transient elastography
Transient elastography was performed on the right lobe of the liver through intercostal spaces on patients lying in the decubitus position with the right arm in abduction. The success rate was calculated as the number of successful measurements divided by total number of acquisitions. The median value of the successful LSM was expressed in kilopascal (kPa), whereas the median value of the successful CAP score was expressed in decibel per meter (db/m). Only LSM and CAP score data, acquired from at least ten successful measurements, success rate of 100%, and IQR/median for both LSM and CAP score of less than 0.3, were considered reliable. LSM and CAP score were assessed by a professionally trained operator.
As previously published, the LSM was graded according to Metavir fibrosis staging by using the following cutoffs: For CHB and CHC, <8 kPa for no or mild fibrosis (F0/1), 8-14 kPa for significant fibrosis (F2/3), and >14 kPa for cirrhosis (F4). For ALD and NAFLD, <8 kPa for no or mild fibrosis (F0/1), 8-19 kPa for significant fibrosis (F2/3), and >19 kPa for cirrhosis (F4) (3, 18, 20, 21, 22, 23, 24). The CAP score was scored according to steatosis grade by using the following cutoffs: <239 db/m for no steatosis (S0), 239-258 db/m for mild steatosis (S1), 259-292 db/m for moderate steatosis (S2), and >292 db/m for severe steatosis (S3) (15).
Statistical analysis
Continuous variables were expressed as means±SD. Comparisons between groups were made using the chi-square or Fisher's exact test for categorical variables and Student's t-test or the Mann-Whitney U-test for continuous variables. We used logistic regression analyses to evaluate the predictive variables associated with the prevalence of diabetes, such as age, gender, BMI, hypertension, hypercholesterolemia, smoking, alcohol consumption, exercise, etiology of liver disease, LSM, CAP score, AST, ALT, and TG; and to determine the odds ratios (OR) for risk factors. Non-parametric Spearman test was used for determining statistical correlations between LSM and CAP score. All analyses were performed using SPSS software (version 21.0 for Windows; SPSS, Chicago, IL, USA).
RESULTS
Patient characteristics
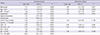
The clinical and laboratory data of the patients are summarized in Table 1. Diabetes was diagnosed in 165 (16.9%) of 979 patients. Regarding the etiology of liver disease, 830 (84.8%) patients had CHB, 101 (10.3%) patients had CHC, 35 (3.6%) patients had ALD, and 13 (1.3%) patients had NAFLD. The mean LSM was 8.61±8.00 kPa, and the mean CAP score was 233.15±47.35 dB/m.
Also, the clinical and laboratory data classified according to the diabetes group and the non-diabetes group were shown in Table 1. Most of the characteristics except for exercise, TG, and TB were significantly different between the diabetes group and the non-diabetes group. Regarding the etiology of chronic liver disease, there was a significant difference between the diabetes and the non-diabetes groups (P=0.001). The mean LSM in the diabetes group (11.22±10.51 kPa) was significantly higher compared to that in the non-diabetes group (8.07±7.29 kPa) (P<0.001). Furthermore, the mean CAP score in the diabetes group (241.65±51.68 dB/m) was significantly higher compared to that in the non-diabetes group (231.42±46.27 dB/m) (P=0.019).
Comparison of prevalence of diabetes according to the etiologies of liver disease
Regarding the etiology of chronic liver disease, patients with ALD and NAFLD showed a significantly higher prevalence of diabetes than those with CHB (OR, 3.21; P=0.001, OR, 3.40; P=0.034). Patients with CHC did not show a significant difference in the prevalence of diabetes compared with those with CHB (OR, 1.18; P=0.553).
Comparison of prevalence of diabetes according to LSM and CAP score
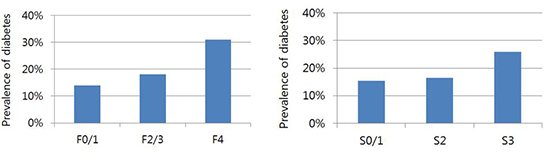
As shown in Fig. 1, the prevalence of diabetes was significantly different among the degrees of LSM or CAP score (F0/1 [14%], F2/3 [18%], F4 [31%], P<0.001; S0/1 [15%], S2 [17%], S3 [26%], P=0.021). The prevalence of diabetes in F4 group was significantly higher than that in F0/1 group or F2/3 group (OR, 2.70; P<0.001, OR, 2.02; P=0.011). The prevalence of diabetes in F2/3 group was higher than that in F0/1 group but there was no significant difference between them (OR, 1.34; P=0.191). Regarding steatosis, represented by the CAP score, the prevalence of diabetes in S3 group was significantly higher than that in S0/1 group (OR, 1.91; P=0.006). The prevalence of diabetes in S3 group was higher than that in S2 group with borderline P value (OR, 1.77; P=0.054). However there was no significant difference between the prevalence of diabetes in S2 group and S0/1 group (OR, 1.08; P=0.740).
A significant correlation was observed between LSM and CAP score in the total patients (r=0.079, P=0.013). In patients without diabetes, there was a mild but a significant correlation between LSM and CAP score (r=0.106, P=0.002), whereas in those with diabetes, there was no significant correlation between LSM and CAP score (r=-0.125, P=0.109).
Predictive risk factors of diabetes
Table 2 shows the significant predictive variables associated with the prevalence of diabetes in univariate analysis including hypertension (OR, 2.65; P<0.001), LSM F4 (OR, 2.53; P<0.001), alcohol abuse (OR, 2.39; P=0.006), current heavy smoking (OR, 2.09; P=0.001), AST>40 U/L (OR, 1.93; P=0.002), CAP score S3 (OR, 1.88; P=0.006), age>50 yr (OR, 1.87; P=0.001), non-CHB etiology (OR, 1.73; P=0.010), male gender (OR, 1.70; P=0.005), BMI>25 kg/m2 (OR, 1.69; P=0.002), hypercholesterolemia (OR, 1.68; P=0.040), and ALT>40 U/L (OR, 1.67; P=0.015). Multivariate analysis showed that the significant independent predictors of diabetes were hypertension (OR, 1.98; P=0.001), LSM F4 (OR, 1.86; P=0.010), male gender (OR, 1.60; P=0.027), and age >50 yr (OR, 1.52; P=0.046) (Table 2).
Subgroup analysis in patients with CHB
In the subgroup analysis with CHB, the prevalence of diabetes also showed significant difference among the groups of LSM or CAP score (F0/1 [12.7%], F2/3 [15.4%], F4 [33.7%], P<0.001; S0/1 [14.4%], S2 [13.2%], S3 [25.8%], P=0.012) (Fig. 2). The prevalence of diabetes in F4 group was significantly higher than that in F0/1 group and F2/3 group (OR, 3.48; P<0.001, OR, 2.79; P=0.001). The prevalence of diabetes in F2/3 group was higher than that in F0/1 group but there was no significant difference between them (OR, 1.25; P=0.386). Regarding steatosis, represented by the CAP score, the prevalence of diabetes in S3 group was significantly higher than that in S0/1 group or S2 group (OR, 2.06; P=0.005, OR, 2.27; P=0.016). However there was no significant difference between the prevalence of diabetes in S2 group and S0/1 group (OR, 0.91; P=0.731).
The significant independent predictors of diabetes in patients with CHB were LSM F4 (OR, 2.48; P=0.001), age>50 yr (OR, 1.83; P=0.010), hypertension (OR, 1.75; P=0.014), and male gender (OR, 1.60; P=0.047) (Table 3).
DISCUSSION
In our study, the patients with chronic liver disease had a high prevalence of diabetes compared with that in the general population, which is known to be about 9% in Korea (25). Especially, the patients with ALD and NAFLD showed a significantly higher prevalence of diabetes than those with CHB. Previous studies also showed a high prevalence of diabetes in patients with CHC, ALD, NAFLD (1, 2, 26, 27). However, for the patients with CHB, the results for the prevalence of diabetes have been conflicting (2, 7, 8). Our data indicate that patients with CHB had a higher prevalence of diabetes than the general population, but it was lower than that in patients with other etiologies of chronic liver disease. The prevalence of diabetes in CHC was higher than that in CHB, but there was no significant difference.
Our results demonstrate that the degree of liver fibrosis assessed by transient elastography has a significant relationship with the prevalence of diabetes in patients with chronic liver disease. Moreover, these results were similarly observed in patients with CHB. Previous studies in which liver biopsy was performed for assessing the fibrosis stage also showed similar results (28). However, liver biopsy has limitations such as invasiveness, and hence small-scale studies were reported. On the other hand, our study that is large-scaled and in which a non-invasive method, transient elastography, was used showed that liver fibrosis has a significant relationship with diabetes.
This study identified the significant independent predictive factors of diabetes such as hypertension, liver cirrhosis, male gender, and old age in patients with chronic liver disease including CHB. More important predictors were hypertension and liver cirrhosis (LSM F4). These risk factors shown in our study were quite different from the risk factors of diabetes in the general population such as obesity, low exercise, smoking, alcohol consumption, and family history of diabetes (29). Like our study, previous studies also identified different risk factors of diabetes in patients with chronic liver disease compared with those in the general population; however, these risk factors were different among studies (28, 29, 30).
In our study, univariate analysis showed that severe steatosis is significant risk factor for diabetes. However multivariate analysis did not show significant independent relationship between severe steatosis and diabetes. These findings indicate that liver fibrosis is a more important factor for the development of diabetes than steatosis in patients with chronic liver disease, especially CHB. Previous study which was conducted in patients with CHC also showed similar results through liver biopsy (28). Several mechanisms could be suggested: blood shunting due to portal hypertension and secretion of pro-inflammatory cytokines (TNF-α, NF-κB) from liver cirrhosis mainly result in diabetes in chronic liver disease (2, 29, 31). Additionally, our study consisted of a large number of CHB group (84.8%) compared to NAFLD group (1.3%). Previous studies with NAFLD have shown that steatosis is an independent risk factor of diabetes (26, 27). Considering this, if our study had had a large number of patients with NAFLD, steatosis might have been an independent predictive factor of diabetes.
Among the etiology of the chronic liver disease, the proportion of CHB was more than 70%, whereas the total proportion of other etiologies was less than 30%. Thus we analyzed data limited to the patients with CHB. The subgroup analysis of patients with CHB showed the similar results as those with chronic liver disease.
Our study demonstrates the prevalence of diabetes in a relatively larger population with major chronic liver diseases, especially CHB, using a non-invasive transient elastography. Especially the CAP score, assessed by transient elastography, was recently found to be a promising measurement of steatosis, although further studies are needed for the CAP score to be accepted as a standard measurement of steatosis. It is noteworthy to apply this method in practice for the first time. Moreover, our study excluded the patients with the factors, which may influence values in transient elastography, such as high level of transaminase, TB, and IQR/median (22, 32, 33). Therefore the diagnostic accuracy of transient elastography was increased. In addition, the data about life style were prospectively collected with accuracy.
However, there were several limitations of this study. First, we did not apply all of the ADA criteria to diagnose diabetes such as post prandial or random glucose levels. Therefore, some of the patients with diabetes might not be included in the diabetes group. Second, there was a lack of pathologic data. Although transient elastography is known to be a relevant method, especially in patients with chronic liver disease, liver biopsy is still regarded as the gold standard for assessment of liver fibrosis.
In conclusion, there is a significant association of diabetes with hypertension, liver cirrhosis (LSM F4), male gender, and old age in patients with chronic liver disease. The degree of liver fibrosis, but not steatosis, assessed by transient elastography has a significant relationship with the prevalence of diabetes in patients with chronic liver disease, especially CHB.

 XML Download
XML Download