

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recent reports have linked hyperuricemia to the increased risk of hypertension, and the progression of renal disease (1). Hyperuricemia was found to precede the development of hypertension and to be present in the majority of newly diagnosed hypertensive adolescents (2, 3). In a recent cohort study in Japan, hyperuricemia was associated with a greater incidence of patients developing end-stage renal disease (ESRD) and was an independent predictor of ESRD in women (4). A high uric acid level also correlated with the development of renal insufficiency in patients with type 2 diabetes (5). However, many confounding factors have made it difficult to draw firm conclusions from epidemiological studies examining the influence of hyperuricemia on blood pressure (BP) and renal function. Recent studies have shown that allopurinol therapy decreased BP and helped preserve kidney function in hyperuricemic subjects, suggesting a direct causative role for hyperuricemia (6). In line with these results, a Japanese survey revealed that most nephrologists recommended uric acid lowering therapy (UALT) in patients in chronic kidney disease (7). The effects of UALT on BP and kidney function in gouty subjects, however, have been scarcely reported, especially in a randomized controlled trial setting. The aim of this study was to observe the short-term effects of UALT, febuxostat and allopurinol, on BP and serum creatinine level, through a post-hoc analysis of data from a randomised controlled trial of gouty patients with normal renal function.
MATERIALS AND METHODS
The data were derived from a phase-III, randomised, double-blind, 4-week trial that compared the safety and efficacy of febuxostat and allopurinol in adult subjects with gout. The subjects met the preliminary criteria of the American College of Rheumatology for gout and had serum urate concentrations ≥ 8.0 mg/dL at screening (8). The ineligibility criteria included a serum creatinine concentration>1.5 mg/dL (133 µM/L), use of thiazide diuretics or medications containing aspirin or other salicylates, active liver disease, and an alcohol intake of more than 14 drinks/week. The study was performed at 10 university-affiliated hospitals in Korea. Approval was obtained from the institutional review boards of each center and all subjects provided written informed consent.
Subjects already on UALT underwent a 2-week washout before the trial. The subjects were then randomly assigned to one of five groups: three febuxostat (Pantheon, Bourgoin-Jallieu, France) groups receiving 40, 80, and 120 mg/d, an allopurinol (Samil Pharmaceuticals, Seoul, Korea) group receiving 300 mg/d, and a control group receiving a placebo. Each patient underwent physical and laboratory examinations at baseline and at weeks 2 and 4. Laboratory samples were collected from each patient following a 12-hr fast, and tests (including serum uric acid and creatinine) were performed using standard assays at the central study laboratory. BP was measured with a sphygmomanometer and the second and third of three measurements were averaged to estimate systolic and diastolic pressure. eGFR was calculated according to the following formula: eGFR = 186×Creatinie-1.154×Age-0.203×(0.742 if female)×(1.210 if black).
Because continuous variables did not follow normal distribution according to Sharpiro-Wilk test except for creatinine level, baseline differences between treatment groups were evaluated using Kruskal-Wallis test (SAS, version 9.2, SAS Institute, Cary, NC, USA). Chi-square tests were used for categorical variables. Differences between results at baseline and week 2 or 4 were tested using the Mann-Whitney U and chi-square tests for continuous and categorical variables, respectively. Changes in BP, serum creatinine levels and eGFR among the experimental groups were compared using a linear mixed-effects model after adjustment for age, body mass index (BMI), smoking, and baseline BP, creatinine, and eGFR. To observe the relationship between decreases in serum uric acid and decrease in BP, serum creatinine, or eGFR, the correlation between decrease in uric acid level and the decrease in BP, serum creatinine or eGFR level were examined using linear regression analysis with generalized estimating equation (GEE) after adjusting for age, BMI, treatment group, and baseline serum uric acid, baseline BP, baseline serum creatinine and eGFR.
Data were available for 179 patients (febuxostat 40 mg/d, n = 35, 80 mg/d, n = 35, 120 mg/d, n = 36; allopurinol 300 mg/d, n = 36; placebo, n = 37). Seven patients (2 placebo, 1 febuxostat 80 mg/d, 2 febuxostat 120 mg/d, 2 allopurinol) missed a follow-up or withdrew prematurely after week 2. Missing data were analysed by applying the last-observation-carried-forward method. Significance was established at the 95% confidence level (P<0.05). All reported P values are two-sided.
RESULTS
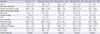
Demographic and laboratory parameters, including mean age, BMI, systolic and diastolic BP, serum creatinine, and fasting glucose, did not differ among the experimental groups at baseline (Table 1). All subjects were male.
Changes in BP and laboratory parameters
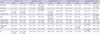
Table 2 presents changes in systolic and diastolic BP and laboratory parameters of all subjects from baseline to weeks 2 and 4. At week 4, diastolic BP had increased significantly in the control group and decreased significantly in the allopurinol group. Systolic BP had decreased significantly in the allopurinol and febuxostat 120 mg/d group. Serum creatinine levels and eGFR had decreased significantly in the febuxostat 40 mg/d group at week 2 and in the febuxostat 120 mg/d group at week 4. After adjusting for confounding variables, no significant difference compared to baseline in changes of BP and serum creatinine levels was observed in any of the five groups (data not shown). Comparison of the four UALT groups combined (any UALT) with the control group revealed no significant difference in systolic BP at any time point (data not shown). Any UALT group showed significantly decreased diastolic BP and serum creatinine at week 4 compared to control. The same analysis was performed to compare the control, allopurinol, and 3 febuxostat combined groups. At week 4, diastolic BP had decreased significantly in the allopurinol group compared with the other two groups (Table 3), and serum creatinine level had decreased significantly and eGFR increased significantly in the febuxostat group compared with the control group.
Relationship between changes in uric acid level and changes in blood pressure or serum creatinine level
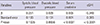
Analysis was performed to determine associations between the change in uric acid and changes in BP, serum creatinine levels and eGFR. Lower target uric acid levels tended to be associated with decreased diastolic BP and serum creatinine levels (data not shown). After adjusting for age, BMI, treatment group, and baseline serum uric acid, baseline BP, baseline serum creatinine level and baseline eGFR, changes in serum uric acid level were not associated with changes in systolic or diastolic BP (Table 4), but were significantly associated with changes in serum creatinine level and eGFR (0.005 mg/dL decrease in serum creatinine and 0.34 increase in eGFR for every 1 mg/dL decrease in uric acid, P<0.001).
DISCUSSION
This post-hoc analysis of a double-blind, 4-week, randomised controlled trial comparing the efficacy of three different doses of febuxostat, allopurinol and a placebo found that UALT significantly decreased diastolic BP and serum creatinine. Comparison of the control, allopurinol, and combined febuxostat groups demonstrated that diastolic BP decreased in the allopurinol group and serum creatinine decreased in the febuxostat group. Changes in uric acid level were significantly correlated with changes in serum creatinine level.
The mechanism of BP elevation and renal injury by increased serum uric acid has been investigated in animal models. Elevation of serum uric acid by the inhibition of uricase in the rat results in development of hypertension mediated by endothelial dysfunction and activation of the renin-angiotensin system (9). Over time, the rats developed renal microvascular disease with arteriolosclerotic-type lesions. Renal injury in hyperuricemic rats consisted of afferent arteriolopathy, mild tubulointerstitial fibrosis, glomerular hypertrophy, and eventually, glomerulosclerosis (10). Uric acid may increase BP by inhibiting nitric oxide (NO) bioavailability, thereby inducing endothelial dysfunction (11).
In a prospective study, hyperuricemic patients with normal renal function showed decreased systolic and diastolic BP and C-reactive protein (CRP) after treatment with 300 mg/d allopurinol for 3 months (12). Systolic and diatolic BP decreased by 4 mmHg and 2 mmHg, respectively in the allopurinol treated group. This result is comparable to our allopurinol-treated subjects, who showed decrease of 6 and 4 mmHg in systolic and diastolic pressure, respectively. In another prospective, randomised, controlled trial including 54 hyperuricemic patients with chronic kidney disease, patients treated with allopurinol for 12 months showed no decrease in systolic or diastolic BP (6). This discrepancy may stem from differences in study subjects (normal vs. compromised renal function). The lowering of uric acid may not effectively normalise BP in arteries with irreversible structural changes, highlighting the importance of early correction of hyperuricemia. In our study, diastolic BP decreased significantly in the combined UALT groups, especially in the allopurinol group. Although allopurinol and febuxostat are both xanthine oxidase inhibitors, allopurinol differs from febuxostat in the inhibition of additional enzymes in the purine and pyrimidine metabolism pathways (13). A study comparing allopurinol and probenecid showed that probenecid improved endothelial function less effectively (14), raising the possibility that the effects of allopurinol are mediated by its ability to reduce vascular oxidative stress rather than by urate reduction. This hypothesis is commensurate with our result that the change in serum uric acid was not associated with the change in systolic or diastolic BP. On the other hand, a longer-term study showed that febuxostat significantly ameliorated systolic and diastolic blood pressures in gouty patients with hypertension following a treatment period for 28 weeks (15). Furthermore, a recent study showed that although febuxosat and allopurinol both effectively lower uric acid levels in patients with severe gout, after 1 yr of therapy, a carotid-femoral pulse wave velocity, an index of arterial stiffening increased only in the allopurinol group (16).
Significant changes in serum creatinine were achieved after only 1 month in any UALT group in our study. The decrease in serum creatinine was significant only in the febuxostat group in 3 group comparison. In a recent post-hoc analysis of an open-label clinical trial of febuxostat in 116 gouty subjects, 1 mL/min improvement of glomerular filtration rate was observed for each 1 mg/dL decrease in serum uric acid (17). On the other hand, another study showed that treatment with allopurinol led to decreases in serum creatinine after 3 months (12). The absence of such effects caused by allopurinol in our study may, thus, be due to our small sample size or short follow-up period.
Our study has strengths and limitations. Our data were derived from a randomised controlled trial, eliminating potential biases associated with a non-controlled setting. The significance of the hypertension data in this study, on the other hand, may be limited due to a small number of study patients with few patients defined as hypertensive, and short study duration. Larger, longer-term studies may establish the influence of anti-hyperuricemic drugs on blood pressure. Although febuxostat group showed significantly decreased serum creatinine level, the absolute value of this decrease was small (0.03 mg/dL). Considering that the study duration was only 4 weeks, more sustained suppression might have led to further change. In a recent report, for every 1-mg/dL decrease in serum uric acid level from baseline, an improvement of 1.15 mL/min in eGFR per year was observed within the 4-yr period of study (18). The study was performed in male gouty patients with normal kidney function, and the results may not be extrapolated to female patients or to those with renal insufficiency.
In conclusion, UALT in male gouty subjects significantly decreases diastolic BP and serum creatinine level. Changes in uric acid level are significantly correlated with changes in serum creatinine level, suggesting the feasibility of preventing renal function deterioration through UALT in gouty subjects.

 XML Download
XML Download