

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since its clinical introduction in the 1980s, the high-field magnetic resonance (MR) scanners has been progressively developed to improve the signal-to noise ratio (SNR) and contrast susceptibility for the better human brain images (1, 2). The current use of higher-field MR scanners for brain tumors is limited to 3.0T because of technical and safety issues (3). There have been several reports of contrast-enhanced MR imaging (MRI) using high-field magnets such as 7.0T for the visualization of brain tumors in the rodent brain tumor animal model and some cases of human brain tumors (4, 5, 6). To our knowledge, however there was no report about the contrast-enhanced 7.0T MRI taken both before and after surgery in a patient with a glioblastoma. Hereby we reported a case of small cell glioblastoma in a 45-yr-old female patient with contrast-enhanced 7.0T brain MRI taken before surgery and at the time of recurrence in comparison of 1.5T and 3.0T brain MRI.
CLINICAL PRESENTATION
A 45-yr-old female patient was admitted with one-month history of headache and progressive left hemiparesis (grade IV/V) on January 8th, 2010. T2-weighted imaging (T2-WI) and pre- and post-contrast T1-weighted imaging (T1-WI) obtained at 1.5T (Fig. 1A-A', D-D') and 3T (Fig. 1B-B', F-F') demonstrated a mass lesion in her right frontal lobe. She had taken 7.0T MRI (Magnetom 7.0T, Siemens®) one day before initial surgery (Fig. 1C-C', E-E', G-G'). She underwent right fronto-parietal craniotomy and the tumor was subtotally resected (Fig. 2A, B). Her brain tumor was confirmed as a small cell glioblastoma (Fig. 2C). The tumor was composed of less pleomorphic small astrocytic cells but had high mitotic rate (6/10HPF), vascular endothelial hyperplasia and necrosis. On fluorescence in situ hybridization study, neither 1p nor 19q deletion was noted but epidermal growth factor receptor (EGFR) gene amplification was robust (Fig. 2D). O6-methylguanin-DNA methylatransferase was not hypermethylated on methylation specific PCR study. She underwent concomitant conventional radiation therapy with temozolomide (75 mg/m2/day) for 6 weeks. But she had refused to receive booster temozolomide against medical advice. A follow-up 1.5T brain MRI, taken at 8 months after initial surgery demonstrated tumor recurrence in the right frontal lobe adjacent to the anterior horn of the right lateral ventricle, remote from the original site (Fig. 3A, B, C). 7.0T MRI (Magnetom 7.0T, Siemens®, Erlagen, Germany) was performed again one day before second surgery (Fig. 3D, E, F). Her recurrent brain tumor was histologically confirmed the same as the previous one, a small cell glioblastoma with EGFR gene amplification. After surgery she was treated with six cycles of avastin (10 mg/kg/day) and irrinotecan (120 mg/m2/day) every 2 weeks but succumbed to death due to tumor progression at 15 months after her initial surgery.
We received the permission from the Korean Food and Drug Administration and the institutional review board of Seoul National University Hospital and the Neuroscience Research Institute of Gacheon Medical Center (IRB Number: 0802-046-234). A written consent was obtained from the patient. The 7.0T MRI (Magnetom 7.0T, Siemens®, Erlagen, Germany) at Neuroscience Research Institute of Gacheon University of Medicine and Science was used for imaging of the patient. The 7.0T magnet, with a clear bore of 90 cm, is equipped with a water cooled gradient and RF coils. The gradient system operates at 2,000 V/650 Amp with gradient amplitude of 40 mT/m, a maximum slew rate of 200 mT/m/ms, and a minimum gradient rise time of 200 microseconds. A home-made 8 channel TX/RX coil was used. High resolution T2*-weighted images were acquired as the following scanning parameters: TR=1,180 ms, TE=17.1 ms, thickness=1.5 mm, gap=1.5 mm, flip angle=30°, number of slices=20, voxel size=0.25×0.25×1.5 µL, and matrix size=704×1,024. T1-weighted MRI was scanned before and after injection of a contrast agent. The Magnevist (Bayer healthcare Pharmaceuticals Inc., Berlin, Germany) was used as the contrast agent by 0.2 mL/kg (0.01 mM/kg). Pulse sequence used was 3D MPRAGE (magnetization prepared rapid gradient echo) and the followings are the scanning parameters: TR=4,000 msec, TE=4.39 msec, TI=1,100 msec, Thickness=0.8 mm, flip angle=10°, number of slice=240, voxel size=0.4×0.4×0.8 mm, and matrix size=384×384. The 3.0T and 1.5T preoperative MRI were performed using a quadrature transmit-receive head coil. The 3.0T MRI protocol included the following: axial unenhanced and enhanced T1-weighted (TR=600 msec; TE=8.0 msec; flip angle=90°) 3-dimensional spoiled gradient acquisitions with a section thickness of 5.0 mm, field of view of 24 cm, and matrix size of 384×192 and T2-weighted acquisitions (TR=4,500 msec; TE=104.4 msec) in the axial planes with a section thickness of 5 mm, field of view of 24 cm, and matrix size of 448×256. The 1.5T MRI protocol included the following: axial unenhanced and enhanced T1-weighted (TR=400 msec; TE=8.0 msec; flip angle=65°) 3-dimensional spoiled gradient acquisitions with a section thickness of 5 mm, field of view of 24 cm, and matrix size of 256×192 and T2-weighted acquisitions (TR=4,000 msec; TE=115.2 msec) in the axial planes with a section thickness of 5 mm, field of view of 24 cm, and matrix size of 256×256. 7.0T axial images were co-registered to 1.5T axial images using a software, OnDemand3D™ (CyberMed, Seoul, Korea). Co-registration was automatically performed by an algorithm based on the mutual information method. Locations of AC and PC, and tumor margins were compared in both image sets five times with the program of OnDemand3D™ (CyberMed, Seoul, Korea).
Findings of 7.0T Brain MRI
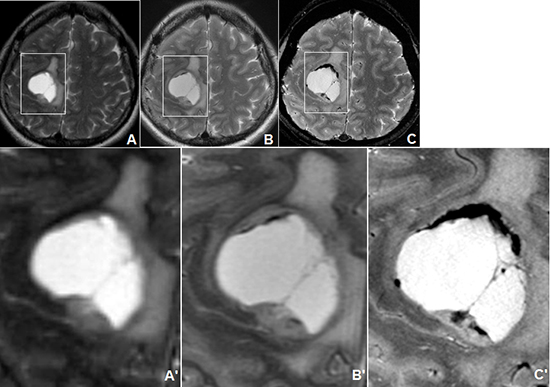
7.0T brain MRI with contrast enhancement was safely performed before surgery (Fig. 1C, E, G). Enhanced anatomical details of the brain tumor were provided by 7.0T MRI. The T2*-Weighted Image (T2*-WI) of 7.0 T brain MRI (Fig. 1C) provided a sharper delineation of the central necrosis and hemorrhage in the peripheral parts of the tumor bed with detailed anatomical information compared with the T2-WIs of 1.5T (Fig. 1A) and 3.0T (Fig. 1B) brain MRI. Irregular areas of heterogeneous signal intensity in the tumor area were best displayed on T2-WI of 7.0T brain MRI, presumably representing hemorrhage or tumor microvasculature (Fig. 1C). Fig. 1A', B', and C' which represent the four-times magnified vision of marked areas in Fig. 1A, B, and C, respectively, shows fine intratumoral structures such as cyst walls or small vessels in T2*-WI of 7.0T MRI (Fig. 1C') compared with those of the 1.5T (Fig. 1A') and 3.0T (Fig. 1B') brain MRIs. In the T1-WI of 7.0T MRI (Fig. 1E), we could clearly see heterogeneous component of the brain tumor clearly delineated from surrounding compressed brain cortex whereas only low signal intensity regions are identified in the T1WI of 1.5T brain MRI (Fig. 1D). Fig. 1D', and E' which represent the four-times magnified vision of marked areas in Fig. 1D and E, respectively, reveals better contrast between solid and cystic components, and more detailed intratumoral stuctures in T1-WI of 7T brain MRI (Fig. 1E') compared with that of 1.5T brain MRI (Fig. 1D').
The contrast- enhanced T1-WI of 7.0T brain MRI (Fig. 1G) showed a clearly defined rim-enhancing mass lesion with sharp margin from the surrounding compressed brain cortex whereas only low signal intensity regions are identified in the contrast-enhanced T1-WI of 3T brain MRI (Fig. 1F). Fig. 1F' and G' which represent the four-times magnified vision of marked areas in Fig. 1F and G, respectively. When we have a close look at the Fig. 1F' and G', shows the better contrast between enhancing and non-enhancing portion in the contrast-enhanced T1WI of 7.0T brain MRI (Fig. 1G') than that of 3.0T brain MRI (Fig. 1F').
Contrast-enhanced 7.0T brain MRI safely performed without any distortion caused by CranioFix®2 (Aesculap Inc. PA) at the craniotomy site (Fig. 2A, B) at the time of recurrence (Fig. 3). In comparison with 1.5T brain MRI (Fig. 3A, B, C), enhanced anatomical details of the brain tumor were provided by 7.0T MRI (Fig. 3D, E, F) as the same as the preoperative 7.0T MRI.
We found that there was no significant discrepancy of the location of the AC and PC as well as the margin of the tumor in the right frontal lobe in the co-registered images of the 1.5T MRI (Fig. 3G, H) and 7.0T MRI (Fig. 3I, J) taken at the time of recurrence.
DISCUSSION
We have demonstrated in this case that contrast-enhanced 7.0T MRIs were safely taken before surgery and at the time of recurrence in a patient with a small cell glioblastoma. In the past, there were several anecdotic reports of high field MRI of 7.0T or higher performed in a small group of normal subjects or patients (2, 4, 5, 6, 7, 8). Thomas et al. (2) described the in vivo 7.0T MRI of higher signal-to-noise and novel contrast to provide enhanced scrutiny of hippocampal anatomy with their micro-venous structures in six normal subjects. Kollia et al. (7) compared the 7.0T MRI with conventional 1.5T MRI in twelve consecutive patients with clinically definite multiple sclerosis. They have reported that ultra-high-field imaging of patients with multiple sclerosis at 7.0T MRI was well tolerated and provided better visualization of multiple sclerosis lesions in the gray matter.
There have been several reports of contrast-enhanced MRI using high-field magnets such as 7.0T for the visualization of brain tumors in the rodent brain tumor animal model and human brain tumors (2, 4, 5, 6, 7, 8). Cha et al. (4) evaluated the growth and vascularity of implanted GL261 mouse gliomas by using 7.0T MRI with conventional T1- and T2-WI and dynamic, contrast-enhanced T2-WI in 34 C57BL6 mice at different stages of tumor development. Lupo et al. (5) assessed the feasibility of g Generalized Autocalibrating Partially Parallel Acquisition (GRAPPA)-based susceptibility-weighted imaging (SWI) technique at 7.0T in healthy volunteers and 11 brain tumor patients. They suggested that unique forms of contrast in 7.0T SWI may be useful for assessing response to both radiation and antiangiogenic therapies for patients with brain tumors (5). Moenninghoff et al. (6) reported 7.0T MR findings of astrocytic brain tumors (WHO grades II-IV) in comparison with 1.5T MRI. They described that 7.0T MRI offers more detailed depiction of tumor microvascularity and necrosis within intracranial gliomas because of higher achievable spatial resolution and increased sensitivity for susceptibility contrast compared with 1.5T MRI (6). Paek et al. (8) reported pre- and post-contrast 7.0T MR findings of twenty-three patients with brain tumors (WHO grades I-IV) in comparison with 1.5T MRI. They described that the T2*-weighted images from 7.0T brain MRI revealed detailed microvasculature and the internal contents of supratentorial brain tumors better than that of 1.5T brain MRI. For brain tumors located in parasellar areas or areas adjacent to major cerebral vessels, flow-related artifacts were exaggerated in the 7.0T brain MRIs. For brain tumors adjacent to the skull base, susceptibility artifacts in the interfacing areas of the paranasal sinus and skull base hampered the aquisition of detailed images and information on brain tumors in the 7.0T brain MRIs in the study (8).
However, there was no report about the 7.0T MRI with contrast enhancement taken both before and after surgery in a patient with a glioblastoma until now. Our study demonstrated that the contrast-enhanced T1-WI of 7.0T MRI, using 3D MPRAGE sequence can show detailed brain imaging of a small cell glioblastoma as Takeda et al. (9) reported the superiority of 3D MPRAGE in the brain tumor imaging. Geometric distortion due to static field and local susceptibility effects has been a major concern in high-field MRI (10). Despite these technical issues, we found that the co-registered 7.0T MRI have only a little discrepancy in the positions of the physiological landmarks such as AC and PC as well as the location and shape of the brain tumor from 1.5T MRI.
In conclusion, we report that 7T.0 MRI can be safely utilized before and after surgery for the treatment of a patient with a small cell glioblastoma. We think this case report is an important landmark for the clinical application of ultra-high field MRI in the field of neuro-oncology in near future.



 XML Download
XML Download