

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The introduction of antiretroviral therapy (ART) has led to profound reduction in morbidity and mortality among people living with HIV (1, 2). Despite of availability of ART, a substantial portion of human immunodeficiency virus (HIV) infected patients has continued to die from both AIDS-related and non-AIDS-related causes (3). A number of factors may contribute to these deaths, but the mortality rate, cause of death, and risk factors for death are variable between countries, depending on several factors such as socio-economic, cultural, and health-care factors (4-7). In low- and middle-income countries, disproportionately high mortality has been observed in the first few months after ART initiation, especially among profoundly immunosuppressed patients (7-10). In addition, advanced age, anemia, low body mass index, and malnutrition were independent risk factors for early mortality (7, 8). In high-income countries, along with increased survival, the causes of death among HIV-infected patients have gradually changed. Although a substantial proportion of deaths continue to be AIDS-related, particularly among those with lower CD4 cell counts and those presenting late to care, the proportion of non-AIDS-related death has increased in ART era (3, 11, 12).
As of December 2010, a total of 7,656 individuals were diagnosed with HIV infection in Korea (13). Despite improved survival in ART era in Korea, there was still a high risk of death at early time points after diagnosis of HIV infection amongst patients with HIV diagnosed late or patients presenting for care with advanced immunodeficiency in ART era (14, 15). In a recent study, we compared the causes of death between pre-ART era and ART era among HIV infected patients in Korea (16). AIDS-related death still remained the leading cause of death in ART era. Overall, tuberculosis and Pneumocystis pneumonia (PCP) were the most common causes of death in pre-ART era and ART era, respectively. There was a trend toward increasing number of PCP and decreasing frequency of tuberculosis as cause of death over time (16). These findings also seem to be the result of the increase of the proportion of late presenter to care in ART era. Nevertheless, there are few descriptions of either the causes of death or the associated risk factors for death among HIV infected patients receiving ART in Korea. The objective of this study was to assess mortality rate, specific causes of death, and risk factors associated with death in adults receiving ART in Korea. We also investigated whether cause of death and the determinants for death differ between during the first year of ART and during 1-5 yr after ART initiation.
MATERIALS AND METHODS
Study Design
A retrospective study was conducted to assess the causes of death and the factors associated with mortality among HIV-infected patients receiving ART. Pusan National University Hospital is a 1,220 bed, university-affiliated teaching hospital and provides HIV care for HIV infected patients in southeastern region of Korea, in close collaboration with the local Public Health Centers (PHCs) in this area. An observational, longitudinal database including epidemiological data, clinical courses, laboratory results and treatment records of all patients had been maintained. It was regularly updated on each visit including inpatient and outpatients care.
The study included HIV infected patients aged 18 yr and older who started ART at the study hospital between 1998 and 2006. Patients who had been started ART in other hospitals before they referred to the study hospital were excluded. Patients who had undergone zidovudine mono-therapy or dual-therapy with two nucleoside reverse transcriptase inhibitors before starting ART were included. After ART initiation, patients visited HIV care clinic every 2-4 weeks until their HIV-RNA load became undetectable, and then they were followed up every 1-3 months with CD4 cell count and HIV-RNA load measurement every 3-6 months. All medical cost for HIV care including antiretroviral drugs was provided free of charge by the Republic of Korea Government through medical aid or National Health Insurance program, in which local PHCs reimbursed medical expenses for which receipts were provided. Based on the follow-up status of patients to the study hospital as of 60 months after ART initiation, each patient was initially classified as remained in care, dead at the study hospital, transfer-out to other hospitals, or lost. The survival of patients initially categorized as lost was traced in collaboration with local PHCs. We ascertained survival status and, if alive, whether or not the subject was on ART from different hospitals. After tracing, each patient was reclassified as alive or dead.
For the purpose of assessing the difference in mortality rate, cause of death and risk factors associated mortality over time after ART initiation, we divided the 60 month observation time into two time periods, first 12 months after ART initiation and a later 13-60 month period. Mortality rates, causes of death and the determinants for death were analyzed respectively and compared between two time periods. The indications for initiation of ART and choice of the initial regimen for ART-naive patients were based on the U.S. Department of Health and Human Services guidelines (17).
Definitions
Based on the survival and follow-up status of patients after tracing, the observation periods were measured from the date of ART initiation to the earliest of the following dates: the date of death, the date of the last follow-up visit if the patients were transfer-out, or 12 months after ART initiation for the analysis of the first 12 months (or 60 months after ART initiation for the analysis of a later 13-60 month period) if the patients were alive at that point in time (Fig. 1).
Retention in care was measured by hospital visit constancy during the observation period after initiating ART (18-21). The observation period after starting ART was divided into 3-month time intervals, and the number of 3-month time interval in which patients had at least 1 hospital visit for HIV care was examined. Hospital visit constancy was expressed by percentage, by dividing the numbers of 3-month time interval with at least 1 completed hospital visit for HIV care by the total numbers of 3-month time interval during observation period of interest (Fig. 1). Medical subspecialty appointment except HIV care visit was excluded, but urgent care visit for HIV care was included.
Cause of death was defined as the main condition that initiated the sequence of events resulting in death. Details of the methodology have been previously described (16).
Statistical analysis
Categorical variables were compared using Pearson's chi-square test or Fisher's exact test, whereas non-categorical variables were tested with the Mann-Whitney U-test. The mortality rate for each time period was calculated as the number of deaths per 100 person-years (PY) of observation. Cox proportional hazard regression analyses were used to determine the risk factors associated with mortality for both the first year after ART and a period of 1-5 yr. All variables associated mortality (P < 0.25) in univariate Cox models were assessed in multivariate models using stepwise forward selection. All tests were considered statistically significant at P < 0.05. The statistical analyses were conducted using PASW Statistics 18 (SPSS Inc., Chicago, IL, USA) and STATA 11.1 (StataCorp LP., College Station, TX, USA).
RESULTS
Subjects
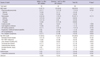
Between 1998 and 2006, a total of 341 patients received ART in the study hospital. Of these, 14 patients who had taken ART before visiting study hospital were excluded, leaving 327 patients for analyses. The baseline characteristics of the study population are presented in Table 1. As of 60 months after ART initiation, 178 patients (54.4%) remained in care in the study hospital, 30 patients (8.8%) were transferred out to other hospitals, 27 patients (8.3%) died in the study hospital, and 92 patients (28.1%) was lost. Of the 92 patients initially categorized as lost, after tracing, 41 patients (44.6%) were known to have died and 51 patients (55.4%) were alive (Fig. 1).
Mortality and cause of death
A total of 68 patients (20.8%) died during the 5-yr observation period; 26 (38.2%) during the first year of ART, and 42 (61.8%) between 1 and 5 yr after start of ART. Overall 5-yr mortality rate was 5.19 per 100 PY (95% confidence interval [CI], 4.03-6.58) and median time from ART initiation to death was 21.1 months (interquartile range [IQR], 4.85-38.83). Mortality rate per 100 PY was higher during the first year of ART (8.69; 95% CI, 5.68-12.73) than the period between 1 and 5 yr after start of ART (4.13; 95% CI, 2.98-5.59). Among 26 deaths occurred during the first year of ART, 15 (57.7%) were AIDS-related death, and tuberculosis (n=8, 30.8%) was the most common clinical condition associated with death (Table 2). Ten patients (38.5%) died of non-AIDS-related death, and non-AIDS infection (n=3, 11.5%) was the most frequent cause of death. Of the 42 deaths occurred between 1 and 5 yr after ART initiation, 23 deaths (54.8%) were AIDS-related and 15 deaths (35.7%) were non-AIDS-related (Table 2). Tuberculosis (n=7, 14.3%) was the most frequent cause of AIDS-related death. Of the non-AIDS-related deaths, liver disease (n=4, 9.5%) was the most common condition associated with death.
Factors associated with mortality within the first year after starting ART
In univariate analysis, CD4 cell count ≤ 50 cells/µL at ART initiation (hazard ratio [HR], 9.14; 95% CI, 2.66-31.37, P < 0.001), clinical category B (HR, 7.55; 95% CI, 1.38-41.21, P = 0.020) and C (HR, 20.99; 95% CI, 4.91-89.83, P < 0.001) at ART initiation, and underlying malignancy (HR, 3.47; 95% CI, 1.04-11.57, P = 0.043) were significant risk factors associated with mortality within the first year after ART initiation (Table 3). Multivariate analysis showed that clinical category B (adjusted hazard ratio [AHR], 7.41; 95% CI, 1.36-40.45, P = 0.021) and C (AHR, 22.24; 95% CI, 5.19-95.43, P < 0.001) at ART initiation, and underlying malignancy (AHR, 4.65; 95% CI, 1.38-15.65, P = 0.013) were significant risk factors associated with mortality during the first year of ART.
Factors associated with mortality between 1 and 5 yr after starting ART
Univariate analysis showed that site of HIV acquisition (HR, 2.61; 95% CI, 1.42-4.81, P = 0.002), underlying malignancy (HR, 4.76; 95% CI, 1.87-12.15, P = 0.001), hepatitis B virus (HBV) co-infection (HR, 6.51; 95% CI, 3.0-14.16, P < 0.001), ART initiation in 1998-2001 (HR, 3.35; 95% CI, 1.78-6.3, P < 0.001), duration from HIV diagnosis to ART initiation 5-10 yr (HR, 2.41; 95% CI, 1.06-5.45, P = 0.035) and > 10 yr (HR, 5.38; 95% CI, 2.21-13.08, P < 0.001), and visit constancy 51-99% (HR, 4.21; 95% CI, 1.5-11.83, P=0.006) and ≤ 50% (HR, 10.16; 95% CI, 4.19-24.62, P < 0.001) were significant risk factors associated with mortality between 1 and 5 yr after ART initiation (Table 4). Multivariate analysis revealed that HBV co-infection (AHR, 4.39; 95% CI, 1.81-10.62, P = 0.001), CD4 cell count at ART initiation ≤50 cells/µL (AHR, 6.68; 95% CI, 2.4-18.6, P < 0.001), and visit constancy ≤50% (AHR, 12.54; 95% CI, 4.3-36.61, P < 0.001) were significant risk factors associated with mortality between 1 and 5 yr after ART initiation (Table 4).
DISCUSSION
Following HIV diagnosis, timely linkage to care, prompt initiation of ART when indicated, and maintaining good adherence to ART are critical for successful HIV treatment. Delayed linkage and poor retention in care have been associated with deleterious clinical outcomes including delayed ART initiation, high rate of ART failure, and worse survival (19, 22, 23). The present analysis showed that the mortality rate and the risk factors for death were different over time after ART initiation. The first year mortality after ART initiation was about 2-fold higher than that of a period of 1-5 yr after ART initiation. During the first year after ART initiation, CDC clinical categories B or C on ART initiation and underlying malignancy were significant risk factors for death. The patients with clinical category C were about 22 times more likely to die than those with clinical category A. These findings are consistent with other studies that have shown that early mortality after ART initiation is related to the delayed treatment initiation due to late presentation to care (4, 24-26). Baseline CD4 cell counts ≤50 cells/µL was associated with early mortality in univariate analyses, however, it was not associated in multivariate models, probably because clinical staging was a better indicator of early death (26). In addition, visit constancy to hospital was not associated with early mortality, suggesting that the patients with high risk opportunistic infections (OIs) for death remained increased risk for early death after ART initiation, even though they remained in good retention in care, before the full effect of therapy had not yet been obtained (9, 10, 27).
Between 1 and 5 yr after ART initiation, poor retention in care, baseline CD4 cell counts ≤ 50 cells/µL on ART initiation, and HBV co-infection were significant risk factors for death. However, clinical category B or C on ART initiation which were risk factors for early mortality were not associated with mortality in 1-5 yr on ART, suggesting that patients with high risk OIs for death initially do not have persistently increased risk for death if they survive the first 12 months of ART (24). In contrast, baseline CD4 cell counts ≤ 50 cells/µL on ART initiation was associated with mortality in 1-5 yr on ART, suggesting that severely immunosuppressed patients still have increased risk for death, even though they survive the first 12 month of ART (28).
In the present study, we traced the patients initially categorized as lost in collaboration with local PHCs. Previous studies conducted in sub-Saharan Africa showed that survival rates may be inaccurate and important risk factors for death may be missed if patients are not actively traced, due to high rates of death among patients lost to follow-up after ART (24, 29). In our study, of 92 patients initially categorized lost, 44.6% were confirmed dead after tracing, resulting in 12.5% increase of number of death after tracing.
In our study, we measured retention in care by hospital visit constancy during the observation period after ART initiation (19-21, 30). This measure is less detail to assess retention in care than appointment adherence, and is computationally more challenging (21). The missed visit within an interval of interest cannot be measured and retention can be overestimated or underestimated by the timing of visit (18, 21). However, this measure is known to be preferable for research for longer observation periods, particularly relevant for patient starting ART, and is better accounts for loss to follow-up (LTFU) than other measures such as missed visit or adherence measure (21). Previous studies have typically included only scheduled outpatient medical appointment for HIV care (19, 22, 23, 31). In this study, however, we included urgent care visit for HIV care to measure the retention because patients who returned to care after LTFU were frequently hospitalized via urgent care, and thereafter successfully retained in care if they survived.
In our study, suboptimal retention in care was common during 5-yr observation period. Among patients who survived more than 12 months after starting ART, 53.5% was regular clinic attendance, whereas 46.5% had various durations of LTFU. Our data showed that patients with ≤ 50% visit constancy were about 13 times more likely to die than those who attended hospital regularly during 5-yr observation period. The patterns of healthcare usage and the duration of LTFU among patients with LTFU were also considerably variable, and 49% of the patients with LTFU demonstrated a cyclical pattern of being in and out of care (32, 33), leading to measuring retention in care more complex in our study.
In addition, HBV co-infection was also independent risk factor for death between 1 and 5 yr after start of ART. HIV infection is associated with more rapid progression to cirrhosis or hepatocellular carcinoma (34, 35). HBV is the most common cause of cirrhosis and hepatocellular carcinoma in Korea, and the prevalence rate in twenties and over showed 7.6% in men and 3.4% in women (36). In our study, the prevalence rate of HBV was 9% in men and 7.5% in women, and slightly higher than that of general population. Because tenofovir has not been available and other anti-HBV drugs, such as entecavir and adefovir have not been covered by public health insurance until end of 2011 in Korea, many HBV/HIV co-infected patients have been treated with lamivudine as monotherapy against HBV in their ART regimen. At present, there are few published data regarding the clinical outcomes of HBV/HIV co-infected patients treated with ART in Korea, and further studies are needed.
Although the mortality rate and the risk factors associated with mortality after initiating ART were different in these two time periods, the causes of death were similar over time on ART. AIDS-related death was more common and tuberculosis remained the most frequent OI associated with death in both time periods.
This study has some limitations. First, this study is an observational study, so we cannot rule out the presence of unmeasured confounding. Second, our study was conducted at a single center in the southeastern region of Korea, and the numbers of death are relatively small, therefore our findings may not be generalized to other region of the country. Third, there was the lack of detailed information about the reason that tuberculosis is the most frequent cause of death, reasons for LTFU after ART initiation, and some missing data on serology for hepatitis due to its retrospective design.
In summary, the mortality rate, cause of death, and risk factors associated with death in adults receiving ART in Korea were different over time after ART initiation. Late presentation to care with AIDS-defining OIs is an important risk factor for early death in the first year of ART, whereas poor retention in care, CD4 cell counts ≤ 50 cells/µL on ART initiation, and HBV co-infection are significant risk factors of late mortality. Different strategies to reduce mortality according to the time period after ART initiation are needed.




 XML Download
XML Download