

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Smoking is a major risk factor for serious diseases such as cancer, coronary artery disease and respiratory diseases (1). It has been emphasized that smoking is a preventable cause of death. Besides the well-known harms of smoking alone, unhealthy lifestyles have been consistently reported to be more related to smoking (2-4). As dietary intake is an important health behavior, concerns for cancer-preventive and vascular-protective properties of nutrients are increasingly growing. Although there are extensive studies on the relationship between nutrient intake and smoking, most of them have been conducted in Western countries (5, 6). Food is influenced by cultural and regional characteristics, thus the dietary pattern of smokers in different cultures merits investigation. Korea is located in East Asia; the country's food and culture is different from those of adjacent countries such as China and Japan.
The smoking prevalence of Korean men is also substantially high at 47.7% (7), based on statistics from five years ago. This rate has since continually decreased over the last decade, but is still three times higher than the smoking rate in America. Traditional Korean food is generally low-fat and known to be healthy. However, the Korean lifestyle today reflects increasingly Westernized influences as the nation continues to develop rapidly in globalization. In fact, the ranking causes of death in Korea are similar to those of Western countries. Cancer is the most important cause of death in Korea, followed by cerebrovascular disease (8).
Previous Korean studies on the nutrient intake of smokers were only sporadically reported, and most subjects were too small or too focused on specific groups (9, 10). Therefore, further study on the nutrient intake and dietary pattern of smokers should broaden its approach to consider a nationally representative sample. While most nutritional research has focused on individual nutrients, the importance of dietary patterns has also recently emerged (11). This is because dietary patterns reflect the complexity of real eating behavior, and identifying such patterns is useful for correcting unhealthy eating habits. This study aimed to identify relationships between smoking status and dietary pattern among Korean men.
MATERIALS AND METHODS
Study population
The Korea Centers for Disease Control and Prevention conducted the fourth Korean National Health and Nutrition Examination Survey (KNHANES IV) in non-institutionalized Korean civilians from 2007 to 2009. A stratified, multistage probability sampling design was used; sampling units were based on geographic areas, sex, and age groups as listed on household registries. The staff conducted household surveys by administering a questionnaire to each participant. The surveys investigated the demographic, medical histories and dietary intake of each respondent. Considering the high smoking prevalence in Korean men, we confined the study population to male adults. The men over 19 yr of age who took participation in KNHANES IV were 7,924 persons. Subjects were excluded from analysis if they were on a restricted diet or if data for total calorie were invalid. Therefore, 5,339 men remained and then we selected participants who provided valid data for smoking. After applying the exclusion criteria, a total of 4,851 men comprised the study subjects.
Dietary assessments and measurements
The one day (24-hr) dietary recall method was used to assess dietary behavior. All participants were requested to maintain their usual diet and experienced interviewers instructed participants to recall and describe every food and beverage consumed during the previous 24 hr. Food models and measuring bowls, cups, and spoons were used to assist in estimating portion sizes. The record for each subject was coded, and standard reference tables were used to convert household portions to gram weights. Nutrient analysis of the records was based on the food composition table of the Rural Development Administration and the nutrient database of the Korea Health Industry Development Institute (12).
Participants were divided into current smokers and nonsmokers. According to World Health Organization's definition, current smokers were defined as smoking at present and having smoked more than 5 packs of cigarettes totaled up to the present date (12). Current smokers were asked the amount and duration of their smoking. Subjects were asked about the average frequency and the amount of coffee and alcoholic beverage consumption during a week. Preceding studies suggested exsmokers followed dietary pattern of nonsmokers (3, 6). Therefore, ex-smokers were classified into nonsmokers. 4,851 subjects were divided into 2,136 current smokers and 2,715 nonsmokers.
Height and weight were measured; body mass index (BMI) was calculated from measured height and weight. Regular exercise was assessed by asking how often and how much the subject engaged in moderate physical activity in a week. Moderate physical activity was defined as physical activities requiring a little shortness of breath. A participant was considered physically active if he engaged in moderate physical activity more than 5 times a week and for at least 30 min each session.
Statistical analysis
To identify the dietary patterns, we used factor analysis based on the 18 food groups from the Korean nutrition database (13). Food groups were expressed as the percentage of energy of each food group and were adjusted by weight differences between solid and liquid foods. Principal component analysis was performed to extract factors. As a first step in factor analysis, we selected food groups with the eigenvalues > 1.1. Then, the factors were rotated using the varimax rotation technique. Five factors revealed distinctive dietary patterns of the study population. Dietary factor scores were categorized into two groups based on the median.
Data were expressed as the means ± standard error for continuous variables. For categorical variables, data were expressed as percentages ± standard error. The chi-square test was performed to demonstrate differences between health behaviors and socio-economic status by smoking group. An independent t test was used to compare age and BMI between smoking groups. Multivariate logistic regression was performed to examine the odds ratios (ORs) for smoking status across the tertile categories of the dietary pattern scores. Logistic models were adjusted for potential confounders such as age, education, regular exercise, BMI and total energy intake. Multivariate logistic regression was also performed to compare the frequency of consumption of coffee and alcohol. And, it was used to compare prevalence of dyslipidemia between smoking groups.
The general linear model was used to test the differences between smoking groups for dependent variables such as nutrient intake, food group after adjustment for sociodemographic variables, BMI and total energy intake. All statistical analyses were performed using the survey analysis method except for factor analysis and correlation.
Analyses were conducted using SPSS 16.02 (SPSS Inc, Chicago, IL, USA) and SAS 9.1 (SAS Institute, Cary, NC, USA). Statistical significance was defined as a P value < 0.05.
RESULTS
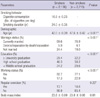
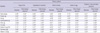
Our study subjects consisted of 2,136 current smokers and 2,715 nonsmokers. Their demographic and clinical characteristics are shown in Table 1. The average smoking amount and duration were 16.9 cigarettes/day and 24.0 yr, respectively. Smokers were significantly younger and more employed than nonsmokers (P < 0.001 and P < 0.001, Table 1). Nonsmokers were more likely to be married (Table 1). Five dietary patterns were found after factor analysis; and the factor loadings of each pattern are shown in Table 2. These five factors explained 50.9% of the variance in total food intake. The five patterns were labeled according to the food groups with high loadings: 'Sugar & fat' pattern; 'Vegetables & seafood' pattern; 'Meat & drinks' pattern; 'Grains & egg' pattern; 'Potatoes, fruits & dairy products' pattern (Table 2). We named pattern according to related food groups with high factor loadings. If a food group was related to more than 2 patterns, we categorized it to a pattern with bigger factor loading value. Because positive factor loadings implied more correlation to patterns, while negative factor loadings meant inverse relation. Blank suggested the food group had the eigenvalues < 1.1. For instance, sugars, eggs, fat and oils showed high loadings for pattern 1. Of those, 'eggs' food group was also related to pattern 4. Thus we thought sugars and fat groups were characteristic of pattern 1. Accordingly, pattern 1 was given a name of 'Sugar & fat'.
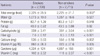
Most patterns were significantly correlated with nutrient intake as expected (Table 3). The 'Vegetables & seafood' pattern showed the highest significantly positive correlation with carotene among all patterns (r = 0.28, P < 0.001, Table 3); the 'Sugar & fat' pattern correlated positively with fat (r = 0.39, P < 0.001); and the 'Grains & egg' pattern correlated positively with carbohydrates (r = 0.49, P < 0.001). The most positive correlation coefficients for dietary fiber were observed in the 'Vegetables & seafood' and 'Potatoes, fruits & dairy products' patterns (r = 0.40 and 0.38, P < 0.001 and P < 0.001, respectively). The 'Potatoes, fruits & dairy products' pattern also showed strong correlation with vitamin C and calcium (r = 0.52 and 0.23, P < 0.001 and P < 0.001, respectively).
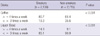
Current smoking was inversely associated with a healthy dietary pattern as indicated in the 'Vegetables & seafood' and 'Potatoes, fruits & dairy products' patterns in multivariate analysis (P = 0.011 and P < 0.001 respectively, Table 4). Smoking status was positively related to the 'Sugar & fat' pattern (P = 0.001, Table 4). The results were adjusted for age, sociodemographic variables, BMI and total energy intake.
The differences of nutrient intake between smoking groups were analyzed with adjustment for total energy intake, BMI and sociodemographic variables. The smoking group showed significantly lower consumption of dietary fiber, calcium, carotene and vitamin C (P < 0.001, P = 0.002, P = 0.001, and P < 0.001, Table 5); on the other hand, total energy intake was significantly higher (P = 0.002). Coffee and alcohol consumption were also different by smoking status. Smokers drank both coffee and alcohol more frequently than nonsmokers significantly (P < 0.001, Table 6). Prevalence of dyslipidemia was significantly higher in smoking group. Namely, high total cholesterol and high triglyceride were more found in smokers (P < 0.001, Table 7). Also low HDL (high density lipoprotein) cholesterol was significantly common in smokers (P = 0.026, Table 7)
DISCUSSION
Using a nationally representative sample, this study showed that current Korean male smokers follow less healthy dietary patterns than nonsmokers. Smokers showed a more significant 'Sugar and fat' dietary pattern and less of the 'Vegetables & seafood' and 'Potatoes, fruits & dairy products' patterns. The findings were compatible with differences in micronutrient intake between smoking groups. Smokers consumed significantly less dietary antioxidants such as vitamin C and carotene than nonsmokers. They also consumed less dietary fiber and calcium but more total energy, as well as greater amounts of alcohol and coffee. Our findings were consistent with the preceding Western studies of the same nature (3, 5, 6).
The importance of dietary pattern is emphasized in recent studies (14). It better reflects real food selection and nutrient intake because people habitually consume diverse nutrients together (15). Therefore, identification of dietary patterns is essential to educating the public on healthy eating habits. Previous studies showed that a prudent dietary pattern with higher fruit, vegetable and dairy product intake was related to lower risk of metabolic syndrome and diabetes (16-18). Inversely, higher consumption of sugars, meats and fat may increase the risk of cardiovascular disease, cancer and diabetes (17). Our results were consistent with other studies which have shown that dietary patterns are correlated to nutritional intake (16, 19). The differences in dietary patterns were concordant with the results of nutrient analysis in terms of fiber, carotene, vitamin C and calcium.
The significance of our study is the close relation between dietary pattern and smoking in Korea, as it is in many Western countries. Therefore, this finding confirmed the conclusion that smoking is associated with less healthy dietary behavior regardless of culture, ethnicity or region. Korean male smokers have similar tendencies to results from preceding studies to follow a 'Sugar & fat' pattern and drink strong alcohol more, but eat less fruit and dairy products (10, 20). In contrast to Western studies, however, our study differs in the consumption of seaweed, starches, and meat. As the Korean peninsula is surrounded by the sea, our culture integrates a diversity of seafood; thus, seaweed is unique and beneficial to the Korean diet because it contains dietary fiber and minerals. Starches were classified within the 'Potatoes and starches' food group and they appear in healthy dietary patterns in our study. Although starches usually belong to Western foods like bread, potatoes are commonly used in Korean side dishes. Potatoes, corn and noodles - which were represented as starches - are also often suitable substitutes for rice, the staple of Korean food. According to a recent Korean study, meat was related to the risk of metabolic syndrome. However, in our study, meat consumption was not prominent in Korean male smokers. This phenomenon merits further investigations.
The strengths of this study are as follows: first, the study subjects made up a nationally representative sample, thus the generalization of the findings to the entire nation are reliable; second, the dietary data was derived from a validated questionnaire, and the food groups were suggested by a validated computerized process (12); third, Korea is one of the East Asian countries which has its own unique foods and culture. Korean food is known to be healthy, rich in vegetables and seafood but relatively low in proportion of meat consumption; fourth, due to the high smoking rate, an investigation on the relationship between smoking and nutrient intake yields prominent results and carries a substantial impact on general public health in Korea. Therefore, our study findings emphasized that smokers' dietary patterns are unhealthy and that the phenomenon is universal across cultures.
The male smoking prevalence in Korea is almost as high as 50%. This places Korea in the group with the highest male smoking rate, along with Turkey and Greece, among the countries of the Organization for Economic Cooperation and Development. Ten years ago, the smoking prevalence of Korean men was 66.3% (21). This may be explained by the provision of free cigarettes while serving in the military, which has been compulsory for all young men in Korea since the division of the Korean peninsula. Consequently, dietary patterns associated with smoking potentially have greater impact on the public health of Koreans than on other populations.
The nutrient status and antioxidant metabolism of smokers have been investigated extensively. According to preceding studies, smoking is not only associated with reduced antioxidant intake but also with an increased turnover of these micronutrients (6, 22, 23). Smokers therefore need more dietary antioxidants such as vitamin C and carotenoids to correct for disadvantageous metabolism as compared to nonsmokers. Smoking in itself is hazardous because of the thousands of alkaloids and carcinogenic chemicals, besides nicotine, which make smokers more susceptible to oxidative stress. Moreover, inflammatory change in the metabolism induces a rapid turnover of antioxidants. Therefore, insufficient and unhealthy dietary intake leaves smokers much more vulnerable to the risk of chronic diseases. Our finding showed dyslipidemia was more found in smokers. This could result from both unhealthy dietary pattern and harmful oxidants of smoking. An imbalanced diet may be one of the reasons for the low health-related quality of life in smokers (24). Also, Korean male smokers consumed less calcium but more coffee and alcohol, which is obviously detrimental to their bone health (9). There is even a theory suggesting that caffeinated or alcoholic beverages may enhance the taste of smoking (10).
The mechanism of the harmful effects of smoking is postulated to explain why their influence on nutrient intake shows so persistently across regional and ethnic differences. Nicotine addiction could induce biological and physiological change of taste or appetite. After adjustment for level of education, job and marital status, the relationship between smoking and diet did not change. Thus, our study did not support the hypothesis that smokers involuntarily maintain an unhealthy diet because they generally belong to a lower socio-economic class. Another hypothesis is that they are less health-conscious; our findings were consistent with the latter in terms of higher alcohol and coffee consumption in smokers. According to a domestic study, smoking was reported to increase health behavioral risks in men (25). This phenomenon is called a clustering of health behavioral risks and is known to have a negative synergistic effect on health outcomes (20). It is therefore important to identify the clustering of risky behaviors to plan and implement a public education program to stop smoking. Although a validated measurement for psychological stress was not available, stress is assumed to act a mediator between health behavioral risks and smoking (26).
We recognize some limitations in this study. First, the 24-hr recall method for dietary assessment may not reflect usual food consumption in some cases. Second, this study was cross-sectional, thus, we could not attribute causal relationships with this design. Third, the factor analysis method to define dietary patterns was somewhat empirical and subjective. For example, the 'grain and egg' pattern in this study was neither a traditional pattern nor one found in Western studies.
In conclusion, Korean male smokers followed a more evident 'Sugar & fat' pattern and less of the 'Vegetables & seafood' and 'Potatoes, fruits & dairy products' patterns compared to nonsmokers. Dietary intake can increase the risk for cancer, cardiovascular diseases and osteoporosis, to which smokers are already susceptible from smoking itself. When designing an intervention for smoking, it is necessary for health professionals to recommend corrections in dietary patterns as well. Future interventional studies may clarify the complex relationship between diverse dietary patterns and smoking in the Korean population.


 XML Download
XML Download