

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Evidence of the value of primary care in health systems continues to accumulate. Research has confirmed that strong primary care health systems provide better population health, more equity in health throughout the populations, and greater economy in the use of resources (1). In the World Health Organization's 2008 World Health Report, all countries were encouraged to orient their health care systems toward strengthened primary care (2). Such reforms are unlikely to improve overall population health, equalize distribution of health care resources or reduce costs unless they address both the systemic and clinical characteristics of primary care (3).
In Korea, the health care system has been dominated by the private sector ( > 90% in health care facilities) (4), comprised of big hospitals owned by global companies (so-called 'chaebols') or private university foundations, and small-to-medium sized facilities of private medical doctors (mostly specialists). Hence the value of primary care has been often neglected by government, as well as providers and patients, for over 30 yr (5). Medical specialists who can run their own community clinics see patients directly without referrals by family physicians. Private sector dominance in health care has led Korea to exhibit the characteristics of a free market even in the National Health Insurance (NHI) system (6). Primary care does not have a gate-keeping role in Korea. The fee schedule for primary care providers is based on the fee-for-service (FFS) (rather than on capitation), resulting in physicians' lack of incentive to focus on health prevention and promotion (4). Under these circumstances, 'induced demand' by physicians and 'doctor shopping' by patients are more likely. It is not strange that Korea shows the high level of outpatient contacts per year per capita compared to the average level of all countries (including Korea) of the Organization for Economic Co-operation and Development (OECD) (6.5 vs 13.0 times in 2009) (7).
It is widely believed that a long-term, sustained doctor-patient relationship (DPR) is vital to good primary health care, promoting satisfaction, effectiveness, and reduced costs. Such relationships are thought to increase in value as the practitioners come to know patients over time, and vice versa. The benefits of this knowledge can be expected to accrue in a variety of ways. For example, patients should make fewer visits because many problems can be managed on the phone. Fewer hospitalizations should also result, since practitioners are more likely to be able to ascertain whether the problem can be managed at home (8). Literature suggests several further benefits of sustained relationships, including greater satisfaction among patients (9-17), physicians, and other staff (13); fewer and/or shorter hospitalizations (9); fewer broken appointments (18); decreased use of laboratory tests (17); and decreased use of emergency rooms for care (10). In addition, increased patient disclosure of personal problems (18) and better compliance with physician instructions have been reported (11).
Recognizing the benefits of primary care, the Government of Korea tried to introduce the family doctor registration system in 1996. This effort failed due to resistance from the Korean Medical Association (KMA), lack of consensus in public opinion, insufficient drive by the Government and scant evidence about the effectiveness of such a system in Korea (19, 20). Since 2003, the Government tried a few demonstration projects locally to induce patients with chronic conditions to enroll to their usual source of care (USC), using financial incentives. Recently, the Government has negotiated a new national program with the KMA. This program is expected to encourage patients with chronic conditions (initially, hypertension and diabetes) to designate a USC among community clinics to improve primary care efficiency by establishing a long-term DPR. Against this background, the authors intend to investigate influential factors associated with length of DPR in the Korean health care setting.
MATERIALS AND METHODS
Participant practices
We restricted subject selection to community clinics where family physicians serve, since family medicine is the only primary care specialty in Korea, and family physicians are relatively homogenous due to a standardized residency curriculum. The family medicine specialty was introduced in 1979. In addition, family practices are homogenous in that they are remunerated by the FFS method under the NHI system and own solo practices (93.5% in 2008) (21). We chose the study sample from the data collected to evaluate the validity of the Korean Primary Care Assessment Tool (K-PCAT) (22). Practices which had been established more than five years before were eligible. Among seven practices recruited, two were in Seoul (the biggest and the most populous city in Korea), two in its adjacent satellite cities (Seongnam and Hanam), and three in small cities remote from Seoul (Gyeongju and Pohang) (Table 1).
Patient selection and the definition of the USC
The patient sample consisted of patients (or guardians) who visited one of the participant practices and agreed to complete the questionnaire before seeing their physicians. Eligible participants were individuals for whom the practice served as their usual source of care. The usual source of care was defined as a provider whom the user had visited at least six times over a period of more than 6 months.
Data collection
The interviewers were trained for standardized technique. Interviewers visited each family practice and administered questionnaires to study subjects and helped them answer the structured questionnaires. The questionnaires included the K-PCAT items and demographic characteristics. The data collection was performed from April 23rd to June 23rd, 2007. For the patients who were less than 18 yr old or disabled, the guardian filled out the questionnaire.
Description of the K-PCAT
The K-PCAT is a validated tool based on the Korean primary care definition, consists of five domains and 21 items including first contact (5), comprehensiveness (4), coordination function (3), personalized care (5), and family/community orientation (4). The Cronbach's alpha within each domain for the K-PCAT ranged from 0.69 to 0.78, except within the first contact domain which consists of five independent subscales (first contact-utilization, facility accessibility, cost appropriateness, demographic accessibility, and basic health care) (22). Each response is on a 5-point Likert scale from 0 to 4. Means of item scores in the same domain are multiplied by 25 to yield domain scores (0-100). Total primary care average score representing primary care quality is the mean of five domain scores. The K-PCAT has been introduced in the Care Coordination Measures Atlas issued by the Agency for Healthcare Research and Quality of the US Government (24).
Statistical analysis
The length of DPR, which was a main topic in this article, was categorized into 3 categories; " < 2 yr", "2-3 yr", and " ≥ 4 yr". Socio-demographic data of participant patients by the length of DPR were analyzed by Mantel-Haenszel chi-square test. Attribute scores of primary care on the K-PCAT were analyzed by one-way analysis of variance. Although the distribution of our outcome measure was not normal, parametric methods could still be used in situations where the sample size was as large as ours (25). We established four logistic regression models for investigating the effects of providers' factors, patients' characteristics and K-PCAT scores on the long term ( ≥ 4 yr) DPR: model 1 including only providers' factor, model 2 including providers' factors and patients' characteristics, model 3 including providers' factors, patients' characteristics and total primary care quality score, and model 4 including providers' factors, patients' characteristics and the five domain scores. Statistical software SAS 9.1.3 (SAS Institute, Cary, NC, USA) was used for the analysis.
RESULTS
Among those who visited their family practice as a USC and were eligible to participate in this survey (n = 591), there were no significant differences between the participants (n = 495, 83.7%) and non-participants (n = 96, 16.3%) in terms of age and sex. The most common reason for refusing to complete the questionnaire was that the patient was too busy. After excluding samples with more than three missing responses (n = 6), a total of 489 effective samples were used for the analysis.
Distributions of socio-demographic variables by the length of DPR
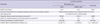
The average age of the patients, who participated in this study, was 47.1 ( ± 21.4) yr (Table 2). When patients' age was categorized as young ( < 40 yr), middle (40-64 yr), and aged ( ≥ 65 yr) groups, the older the age of patient, the longer the length of DPR (P < 0.001). In the old age ( ≥ 65 yr) group, those patients who had a long-term ( ≥ 4 yr) relationship with their physicians was 76.1%. In contrast, that was only 38.8% in the young age ( < 40 yr) group. Female patients were 63.8% and did not show longer term relationship with their family physicians than males. The lower income ( < 1,500 USD equivalent per month) group tended to have longer term ( ≤ 4 yr) relationship with their family physicians. In contrast to the upper income group, middle income (1,500-2,900 USD equivalent per month) group tended to have shorter term ( < 2 yr) relationship with their family physicians (P = 0.007). University graduates (education ≥ 13 yr) tended to have a shorter term relationship with their family physicians, in contrast with groups of education years less than 13 yr (P = 0.037). The number of the diseases being treated showed a significant difference by the length of physician-patient relationship, the more the number ( ≥ 2 or more) of the diseases being treated patients had, the longer ( ≥ 4 yr) the length of physician-patient relationship patients showed (P = 0.008). Patients of the practices in small cities tended to have the longer term DPR, comparing to those in Seoul or its satellite cities (P < 0.001).
Primary care scores of the five domains of the K-PCAT by the length of DPR
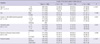
Among 5 domains of primary care of the K-PCAT, the personalized care (91.1 ± 10.5) and the first contact (89.5 ± 10.5) showed relatively high scores compared to the coordination function (62.3 ± 29.6) and the comprehensiveness (50.1 ± 23.5) domains (Table 3). The total primary care quality score (the average of the 5 domain scores) was 71.7 ± 12.8 on a 100 point scale. By the bivariate analysis, primary care scores of the 3 domains, i.e., coordination function (P = 0.026), comprehensiveness (P = 0.001), and family/community orientation (P = 0.030), were significantly different by the length of DPR. Among 5 subscales of the first contact domain, only the first contact-utilization was significantly different in scores with the length of DPR. Between the shorter and middle term DPR, there was no significant relationship in the total primary care quality score. After the length of the DPR became ≥ 4 yr, the total primary care quality score care showed a significant difference (P = 0.001) from those of the other two terms.
Factors associated with the length of DPR
In the model 1, the long term DPR was significantly associated with practice location (small cities vs metropolitan area; odds ratio [OR], 2.08; 95%confidence interval [CI], 1.18-3.66) and duration after the establishment of practice ( ≥ 7 yr vs < 7 yr; OR, 6.08; 95% CI, 3.29-11.23) (Table 4). In the model 2 after adjusting providers' factors, the long term DPR was significantly associated with some patients' characteristics including age (unit: year) ([40-64 vs < 40; OR, 3.53; 95% CI, 2.01-6.20] and [ ≥ 65 vs < 40; OR, 5.91; 95% CI, 2.83-12.35]), and household income per month (unit: USD) ( ≥ 3.0 vs < 1.5; OR, 2.00; 95% CI, 1.04-3.84). After adjusting providers' factors and patients' characteristics, the long term DPR was significantly associated with total primary care quality score (upper [ ≥ 71.4] vs lower [ < 71.4]; OR, 1.74; 95% CI, 1.10-2.76) in the model 3 and the coordination function (OR, 1.01; 95%CI, 1.00-1.02: P = 0.044) in the model 4.
DISCUSSION
The aim of this study was to investigate the influential attributes of primary care associated with length of DPR. The previous study demonstrated that the socio-demographic variables of this study were significantly associated with primary care domain scores of the K-PCAT (22). Therefore the authors controlled these confounding variables by multivariate analysis. The study showed that long-term duration ( ≥ 4 yr) of DPR of family practice was positively associated with total primary care quality score of the K-PCAT in both bivariate and multivariate analysis. The more interesting finding was that this long-term DPR was positively associated specifically with the coordination function among the 5 domains of the K-PCAT in both bivariate and multivariate analysis. Coordination is essential for the attainment of each of the other primary care features. Without it, longitudinality would lose much of its potential, comprehensiveness would be made difficult, and the first-contact function would become purely administrative. Descriptions of primary care from the physician's vantage often refer to the primary care professional as the patient's advocate or in terms of the primary care physician's commitment to people. To accomplish what these terms imply, the primary care physician must be aware of all of the patient's health-related problems in whatever context they arise (26). The concept of the primary care physician as a chief agent and coordinator has been the professional response to the increasing complexity of medical knowledge and specialization. Countries where patient choice was limited have taken steps to extend it, while countries with unlimited choice have been trying to promote rational health care pathways, notably by implementing gate-keeping. The effectiveness of gate-keeping depends however on the ability of primary care physicians acting as effective agents managing and co-coordinating the follow-up of patient care, while utilizing information available on the quality and prices of services supplied by providers of secondary care (27).
Initiatives measuring patients' experiences with individual primary care physicians will achieve different results if studies include patients who have seen the physician versus those whom administrative data indicate as established members of the physician's panel (28). In measuring patients' experience with primary care physicians, patients should have a USC and have experienced its services before. Therefore, to compare the patient assessment of primary care internationally or among institutions, it is required to have a common definition of USC. The PCAT originally invented by Shi et al. (29) used 3 questions to identify a USC and the strength of that affiliation: 1) Is there a doctor or place that you usually go if you are sick or need advice about your health? (usual source), 2) Is there a doctor or place that knows you best as a person? (knows best), and 3) Is there a doctor or place that is most responsible for your health care? (most responsible). On the other hand, however, in using the K-PCAT, the authors applied the different definition of USC (22), considering the health care context of Korea where the choice of provider by patients was virtually open, even under the NHI.
The temporal length of DPR is one of the quantitative aspects of longitudinality in primary care (30). Longitudinality, in the context of primary care, is a long-term personal relationship between physicians and the patients in their practice. Having longitudinal care means that individuals in the population identify with a source of care as "theirs"; that the provider at least implicitly recognize the existence of a formal or informal contract to be their regular source of person-focused (not disease-focused) care and that this relationship exists for a defined period of time or indefinitely until explicitly changed. Although the word continuity is usually used instead of longitudinality, the latter conveys the spirit better than the former (26). On the other hand, continuity has been defined in numerous ways. For example, Saultz proposed a hierarchical definition of continuity from informational to longitudinal to interpersonal (31). However, in primary care it is "mainly viewed as the relationship between a single practitioner and a patient that extends beyond specific episodes of illness or disease" (32). The US Institute of Medicine holds that continuity, defined as an ongoing partnership between patients and physicians, is a central and important component of primary care (33).
Many studies suggest that continuity of care can be regarded as an outcome, and research are needed in how to better achieve it (34-36). If continuity of care is deemed an outcome, then it can become a benchmark of the quality of care rather than an independent variable (37). In our study the length of DPR, one of the measures for the continuity of care, was treated as a dependent variable.
The longer the duration of the DPR, the higher the satisfaction, even when factors such as number of consultations; age and sex of patient; age, sex, location, and type of practice and reimbursement of provider; and type of consultation, illness, and duration of problem are taken into account. For example, patients in 133 Norwegian general practices who had duration of relationship of more than 5 yr were over one-third more likely to report being very satisfied than those with relationships of 1-5 yr (12). In our study, it was interesting that the total primary care quality score of the K-PCAT was not significantly different in the bivariate analysis until the length of DPR reached 4 yr. This suggests that a good quality of primary care will support patients to establish long-term DPR based on mutual trust.
In Korea, expanded access to health care by the introduction of the National Health Insurance (since 1989) has contributed to a marked increase in health spending (38). The health sector has evolved based on competition among private-sector providers that maximize their profits in practice. More than 90% of physicians work in private clinics or hospitals. In addition, 96% of hospitals and clinics are privately-owned and they account for 90% of beds. There is intense competition between hospitals, which run large outpatient centers, and physician clinics, some of which have inpatient care (4). Under this laissez-faire system, even with the NHI, it may be natural that the Korean people who have a USC comprise only 30% of the adult population (39), contrasted with other OECD countries over 80% (40). Patients are free to consult any provider at any time without proof of medical necessity and with reimbursement by the NHI. In addition, family physicians are only 8.2% (6,285/76,379) of all physicians officially trained after the graduation of medical school in 2011 (41). In this health care background, the quality of primary care, especially coordination, can be expected to be poor in Korea.
Since most patients enter the health system at the primary care level, primary care is frequently seen as key to improving the coherence and coordination of care (27). Primary health care is often fragmented in many countries, with little coordination among providers and among levels of care. Those most affected by poor co-ordination are older people and people with chronic conditions. They may require a long term DPR by high quality services in primary care with coordination function. In our study it is expected that patients more than 65 yr old had much longer DPR compared to those less than 40 yr old.
Lack of primary care coordination in Korea can be explained by our finding that practice location was a significantly associated with long-term DPR. Rural areas have 19% of the population but just 10% of the physicians, indicating that the physician to population ratio is about two times higher in urban areas. Large regional variations in the supply of medical facilities also create questions about access (27). Seoul has 25.5 % of all healthcare facilities and the highest facility density per 100,000 population (207.6) in 2011 in Korea (42). This study shows that the continuity of care (the temporal length of DPR in this study) can be hampered by the poor coordination in primary care in metropolitan areas like Seoul where health care providers are abundant and competitive.
The strength of the Korean primary care evaluated by the Starfield's approach has been reported as the weakest comparing to the other 13 OECD countries (43). Therefore, the key policy priority for improving the quality of care in Korea should be the development of a strong primary care sector. This study shows the importance of the coordination function of primary care in the future primary care reform plan for long-term DPR.
This study has several limitations. First, in the context of the Korean health care delivery system, the data obtained only from family medicine practices are not enough to represent primary care in Korea. However, because there has been no official consensus about the range of primary care provider, regarding a family physician as a primary care provider is more reasonable than any other combination of providers for the homogeneity of data, in that family medicine is the only medical discipline claiming to stand for primary care and having an official residency program in Korea. Second, the participant practices were not sampled randomly and were too few (n = 7) to represent family practices in Korea. Third, other factors likely to affect the length of DPR were not controlled in the regression analysis, e.g. other practice characteristics such as the number and kind of staffs, the number of patients a day, and medical equipments as well as the mode of health care coverage (the NHI vs Medical Aid). However, providers were homogenous in that they are family physicians who have experienced the formal residency program and run a solo community-based private practice. In addition, it is not likely that the mode of coverage affected the results, because Medical Aid beneficiaries are only 3% of the Korean people.
In conclusion, the study shows that the quality in primary care is significantly improved after 4 yr of DPR and the long-term DPR is significantly associated with the coordination function among the 5 primary care attribute domains of the K-PCAT. In Korea, primary care policies may require having a focus on strengthening the coordination function, such as the gate-keeping role of the General Practitioner in the several European countries, to establish a long term DPR in primary care. The results of this study would help policy makers design a plan to enhance primary care in countries with weak primary care infrastructures.


 XML Download
XML Download