

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since the early 1980s, the number of incidentally discovered adrenal masses has increased as a result of the widespread use of imaging studies, such as computed tomography (CT) and magnetic resonance imaging (MRI) (1). The prevalence of adrenal incidentalomas is known to be as high as 3% in middle-aged people and 10% in the elderly (2). The prevalence of primary aldosteronism (PA) increases with the severity of hypertension and varies depending on the population under investigation. In a recent meta-analysis, Jansen et al. (3) determined a mean PA prevalence of 4.3% in hypertensive primary care patients and 9.0% in referred hypertensive patients. Currently, only a minority of PA requires surgery, in part because it is difficult to prove that the adenoma is the sole cause of PA (4). The assessment of eligibility for surgery requires differentiation of unilateral Conn's adenoma from cases of bilateral adrenal hyperplasia and nonfunctioning adrenal nodules (incidentalomas) (5). Adrenal vein sampling (AVS) is the most accurate standard test to distinguish these entities; however, it is commonly ineffective because the adenoma only intermittently secretes aldosterone or because of technical difficulties in cannulating the right adrenal vein (6). The purpose of this report is to describe the findings of non-invasive imaging methods that can be used to lateralize aldosterone secretion to one of the bilateral incidentally-detected adrenal masses. Here we report a case where unilateral PA was detected on 18F-fluorodeoxyglucose (FDG)-positron emission tomography (PET/CT) and confirmed by adrenal venous sampling of both adrenal incidentalomas.
CASE DESCRIPTION
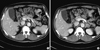
A 53-yr-old man was referred to our clinic on September 5, 2011 after bilateral adrenal masses (right: 1 cm, left: 2.5 cm) were discovered on an abdominal CT (Fig. 1). Two years prior, the patient underwent low anterior resection for sigmoid colon cancer and had received adjuvant chemotherapy. The patient had been prescribed antihypertensive medications (almodipine 10 mg, olmesartan 20 mg) for 12 yr, but his blood pressure could not be controlled well and was found to be 160/90 mmHg on presentation. He was generally well-appearing, but complained of a persistent mild headache. He demonstrated an increased deep tendon reflex in both knees and had no weight gain or edema. Blood analysis revealed persistent hypokalemia (serum potassium of 2.6 mM), but his medications did not include a potassium-wasting diuretic (e.g., thiazide, loop). Laboratory tests showed plasma renin activity (PRA) of 0.12 ng/mL/h and plasma aldosterone concentration (PAC) of 10.4 ng/dL with a PAC/PRA ratio of 86.6. And we confirmed diagnosis of primary aldosteronism with captopril challenge test (post-captopril aldosterone level was 18.5 ng/dL).
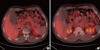
Given his history of colon cancer, we had to rule out metastatic disease before continuing to adrenal venous sampling. FDG-PET/CT of his torso incidentally revealed a focal hypermetabolic lesion in the right adrenal gland (Fig. 2). Generally, the larger tumor has more focal hypermetabolic uptake lesion. But in this case, although right adrenal incidentaloma was smaller than left that, only right adrenal gland had focal hypermetabolic uptake. There was no hypermetabolic uptake except adrenal gland in FDG-PET/CT, the patient was suspected primary aldosteronism clinically. So we thought that right adrenal incidentaloma was not metastatic lesion but benign functioning tumor. Adrenal venous sampling was performed at both adrenal glands, and the aldosterone/cortisol ratio was found to be 15 times higher on the right side than on the left (Table 1). This finding was consistent with the results of FDG-PET/CT.
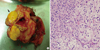
Surgical resection of the right adrenal gland was performed. Pathological examination showed a well-demarcated, golden yellow nodule grossly (Fig. 3A) with tumor cells that resembled cortical cells and showed lipid-laden clear cells microscopically (Fig. 3B). Three months after the operation, the patient's blood pressure, serum potassium level, and plasma renin-aldosterone activity were normalized.
DISCUSSION
The widespread use of CT and MRI has led to an increase in the incidental discovery of adrenal masses, requiring physicians to further evaluate whether the lesions are benign or malignant and lateralize symptoms to one lesion or the other. Many review articles reported that recent advances in CT, MRI, and PET/CT assist in the distinction between benign adenomas and malignant lesions of the adrenal glands (7). Only a few articles described the use of imaging techniques in distinguishing functional adenomas from nonfunctioning lesions of the adrenal glands (9).
F-18 FDG is widely used in clinical PET imaging. Until now, FDG-PET/CT has been used mainly for distinguishing between benign and malignant adrenal masses (8). The combination of FDG-PET/CT and CT in the evaluation of adrenal incidentalomas in patients without a history of cancer has been reported to have a 93% negative predictive value (NPV) for malignancy and a 97% positive predictive value (PPV) for detecting surgical lesions (9). Surgical lesions are defined as a malignancy or a benign secreting tumor. A high FDG uptake (maximum standardized uptake value ≥ 10) was highly predictive of malignancy (9). PET/CT performed for the characterization of adrenal masses in patients with cancer yielded a sensitivity of 100% for the detection of malignancy, in addition to a specificity of 99%, a PPV of 93%, a NPV of 100%, and an accuracy of 99% (10). Conversely, for the detection of benign tumor, the sensitivity, specificity, PPV, NPV, and accuracy were 99%, 100%, 100%, 93%, and 99%, respectively (10).
As mentioned above, FDG-PET/CT is a useful tool for differentiating malignancy, benign secreting tumors, and non-functioning benign tumors in adrenal masses. There are, however, some limitations of FDG-PET/CT in distinguishing adrenal masses. First, it is nonspecific for neoplasms, with uptake by macrophages and other immune cells. Second, neoplasms with low glucose metabolism, such as well-differentiated NET (Neuroendocrine tumor), show poor FDG uptake reflecting the degree of tumor differentiation and biological behavior (11). Third, FDG-PET/CT uptake does not show a consistent pattern for endocrine tumors, which is probably due to the variability inherent in FDG uptake (8). Although FDG-PET/CT has some limitations, it is helpful in lateralizing aldosterone secretion in patients with bilateral adrenal incidentalomas. Furthermore, some of its limitations can be overcome using laboratory tests.
Recently, some reports showed that C-11metomidate (MTO)-PET/CT is a sensitive and specific noninvasive alternative to AVS for lateralizing aldosterone secretion by Conn's adenoma (12). C-11 metomidate, a potent inhibitor of 11B-hydroylase andaldosterone synthase, has been advanced as a positron emission tomography (PET) radiotracer (12).
There was a case report of an adrenocortical adenoma with an increased FDG uptake in patient with subclinical Cushing's syndrome (13). That case suggested that increased FDG uptake may be relevant to hormonal function of an adrenocortical adeoma by glucose metabolism, even in a completely asymptomatic normocortisolism patient. About increased FDG uptake, our case may be related with similar mechanism.
In our case, F-18 FDG-PET/CT was helpful in characterizing adrenal masses and was consistent with the results of AVS, the conventional diagnostic study. Although there are some limitations of F-18 FDG PET/CT in the routine evaluation of adrenal incidentalomas, we propose that F-18 FDG PET/CT can play an additional role for identifying functioning adrenal tumor as an alternative to adrenal venous sampling. Especially in the absence of pre-existing malignancy.

 XML Download
XML Download