

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In the absence of thromboprophylaxis, venous thromboembolism (VTE) occurs in approximately 10% to 80% of critically ill patients (1). Risk factors for VTE in critically ill patients include acute illness such as sepsis, prolonged immobilization, hypercoagulability, vascular injury caused by invasive procedures, mechanical ventilation, and medications such as vasopressors and paralytic agents (1, 2). The early diagnosis of deep vein thromboses (DVTs) is difficult due to vague associated symptoms, with half of all untreated DVTs progressing to potentially fatal pulmonary thromboembolisms (PTEs) (1). As such, thromboprophylaxis for VTE is recommended in critically ill patients due to the high incidence, difficulty of early diagnosis, and high mortality rate of PTEs (1, 3).
Guidelines for patients admitted to intensive care units (ICUs) recommend routine thromboprophylaxis with low molecular weight heparin (LMWH) or low-dose unfractionated heparin (UFH) (1). Enoxaparin is one widely used LMWH, however, data about adequacy of once daily dose of enoxaparin are insufficient. Although some data in European critically ill patients which suggest once daily dose of 40 mg of enoxaparin may not be effective for this purpose (4, 5), it has never been evaluated in critically ill Asian patients. Since heparin is well known to be a drug which has different pharmacokinetic effect according to ethnicity (6-10), the study for adequacy of once daily dose of enoxaparin in Asian critically ill patients is needed.
Therefore, the aim of this study was to examine the time course of antifactor Xa (aFXa) levels after administration of once daily fixed-dose of 40 mg of enoxaparin, and to evaluate the factors associated with effective antithrombotic aFXa levels after administration of enoxaparin among Korean medical ICU patients.
MATERIALS AND METHODS
Patients
This was a prospective observational study. Between August and December of 2011, consecutive patients admitted to the two medical ICUs of Samsung Medical Center (a 1900-bed tertiary referral center in Seoul, Korea) were prospectively recruited. Inclusion criteria included: age greater than 18 yr and below 80 yr, a body weight above 40 kg and below 90 kg, and a predicted ICU stay of more than 24 hr. Enoxaparin (Clexane®; Sanofi Aventis Korea, Seoul, Korea) at a daily dose of 40 mg was administered subcutaneously to all study patients during the ICU stay. Exclusion criteria included: platelet count less than 100,000/µL, any degree of active bleeding, previous exposure to UFH or warfarin, current treatment with continuous renal replacement therapy, creatinine clearance (Ccr) less than 30 mL/min, readmission to the ICU during the same hospitalization, or refusal to provide informed consent.
Data collection and definition
The following data were collected from all patients: 1) general characteristics including age, sex, body weight, height, body mass index, comorbidities, and primary reason for ICU admission; 2) severity of illness as assessed by the Simplified Acute Physiology Score 3 (SAPS 3) (11, 12) and the Sequential Organ Failure Assessment (SOFA) score; and 3) laboratory data prior to the administration of enoxaparin including hematologic, coagulation and chemistry testing.
AFXa levels were measured prior to the subcutaneous administration of enoxaparin, as well as 4, 12, and 24 hr after the first dosing. A commercial clotting assay of heparins (UFH and LMWH) by aFXa (STA-STACLOT® Heparin①; Diagnostica Stago S.A.S, Paris, France) was employed for all analyses of plasma aFXa levels following the manufacturer's instructions. AFXa levels of 0.1-0.3 U/mL were defined as having effective antithrombotic activity (13).
Statistical analysis
STATA 12.0 (StataCorp LP, College Station, TX, USA) were used for statistical analysis. In all cases, continuous variables were shown as medians and interquartile ranges (IQR), while categorical data were displayed as counts (percentages). Univariate logistic regression analyses were performed to identify any factors of effective antithrombotic ranges of aFXa activity at 4 hr and 12 hr after enoxaparin administration. Among the variables used in univariate logistic regression model, factors with a P value less than 0.25 were selected for the multivariate logistic regression analysis. The presence of multicollinearity among two separate variables was evaluated by a variance inflation factor. A two-tailed P less than 0.05 was considered statistically significant in all cases.
Ethics statement
This prospective observational study was approved by the institutional review board of Samsung Medical Center (2011-06-038). In all cases, written informed consent was obtained from patients or their legal representatives to allow serial blood collection for the purpose of observing the time course of aFXa levels.
RESULTS
Baseline characteristics, laboratory findings and outcomes of the patients
During the five-month study period, 315 medical patients were admitted to the two participating ICUs. In total, 117 patients were excluded for thrombocytopenia, 42 patients for active bleeding, 33 patients for a Ccr less than 30 mL/min or concurrent use of continuous renal replacement therapy, 24 patients for previous heparin or warfarin use, 18 patients for ICU stays less than 24 hr, 6 patients for ICU readmission, 5 patients for a body weight less than 40 kg, 11 patients for an age older than 80 yr, and 4 patients for refusal to provide informed consent.
In total, 55 patients were included in this study, with all patients available for follow-up and analysis. Table 1 lists the baseline characteristics of the 55 patients upon admission. Among the 55 patients included, 38 (69.1%) patients were male, and the median age was 64 yr (IQR 53-72), the median body weight was 57 kg (IQR 53-67), the median body mass index was 21.7 (IQR 19.6-23.4), the median SAPS 3 was 42 (IQR 33-51), the predicted in-hospital death rate was 28.5% (IQR 14-48.4), and the median SOFA score was 5 (IQR 3-7). Cancer patients accounted for 36.4% (20/55) of the study sample, with respiratory problems accounting for the most frequent reason for ICU admission (39/55, 70.9%). Median duration of use of enoxaparin was 6 days (IQR 3-12). The median laboratory parameters were as follows: prothrombin time of 1.19 INR (IQR 1.05-1.29), activated partial thromboplastin time of 41 sec (IQR 36-47), antithrombin III of 76% (IQR 62-87), Ccr of 90 mL/min (IQR 67-126), and total bilirubin of 0.7 mg/dL (IQR 0.4-1.7). The incidences of DVT and PTE during the stay of ICU were 12.7% and 1.8%, respectively. There were no bleeding complications. The percentages of severe sepsis or septic shock and use of vasopressors were 38.2% and 36.4%, respectively. ICU mortality was 12.7% and hospital mortality was 12.7%.
AFXa levels of before and 4, 12, and 24 hr after administration of enoxaparin
Four hours after enoxaparin administration, the median aFXa level was 0.22 U/mL (IQR 0.17-0.26). More specifically, 3 patients (5.5%) had aFXa levels below 0.1 U/mL and 4 patients (7.3%) had aFXa levels above 0.3 U/mL, while the percentage of patients within effective antithrombotic range was 87.3% (48/55). Twelve hours after enoxaparin administration, the median aFXa level was 0.06 U/mL (IQR 0.02-0.1). At this time, 37 patients (67.3%) had aFXa levels below 0.1 U/mL and none had an aFXa level over 0.3 U/mL, with 18 patients (32.7%) falling in the effective antithrombotic range. At 24 hr after enoxaparin administration, median aFXa level was 0 U/mL (IQR 0-0.03), and all patients had aFXa levels below 0.1 U/mL (Fig. 1).
Factors associated with effective antithrombotic aFXa levels at 4 hr and 12 hr after enoxaparin administration
Univariate logistic regression analyses were performed in order to look for associations between factors and effective antithrombotic aFXa levels at 4 hr and again 12 hr after enoxaparin administration. There were no factors significantly associated with effective antithrombotic range at 4 hr. At 12 hr, univariate logistic regression analysis revealed that SOFA (odds ratio, 0.58; 95% confidence interval, 0.42-0.81; P = 0.002), total bilirubin (0.04, 0.004-0.39, 0.006), severe sepsis or septic shock (0.21, 0.05-0.85, 0.03), and use of vasopressors (0.24, 0.06-0.95, 0.04) were significantly associated with effective antithrombotic aFXa levels.
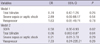
The multivariate logistic regression models were used to determine independent predictors of effective antithrmobotic aFXa levels at 4 hr and 12 hr (Table 2). There were no significant predictors for effective antithrombotic aFXa levels at 4 hr after administration of enoxaparin. At 12 hr, SOFA (0.58, 0.36-0.93, 0.002) and total bilirubin (0.06, 0.003-0.87, 0.04) were independently associated with effective aFXa levels at 12 hr.
DISCUSSION
In this study, we demonstrated low efficacy of once daily fixed dose (40 mg) of enoxaparin for maintaining the effective antithrombotic aFXa levels in Korean medical ICU patients. The low efficacy was more salient for patients with high SOFA scores and hyperbilirubinemia.
According to previous studies, the thromboprophylactic effect of low-dose UFH or LMWH is controversial (14-17). The trials of low-dose UFH or LMWH reported that thromboprophylaxis by heparin was associated with a reduced risk of asymptomatic DVT but failed to demonstrate or exclude a beneficial or detrimental effect of heparin on symptomatic DVT or PTE or major bleeding or mortality. Therefore, further study of adequate dose of UFH or LMWH is needed for effective thromboprophylaxis.
Priglinger et al. (18) and Mayr et al. (4) reported the low efficacy of this standard dose in achieving effective antithrombotic aFXa levels among critically ill European patients. However, we must take caution in generalizing these limited data from predominantly Caucasian population (4, 5, 18, 19) to Asian critically ill patients who are different in terms of genetic and environmental factors. Most drugs exhibit significant inter-subject variability in pharmacokinetics and pharmacologic response, and such differences depend on a variety of intrinsic factors (6, 20). The one of the important intrinsic factors affecting response of a drug is genetic factors which determine drug metabolism and its pharmacologic response. Doses of heparin required to reach therapeutic levels have been reported to be significantly lower in Asians compared to Caucasians (6-9). Also there are differences in genetic make-up of proteins involved in coagulation system factors between Asians and Caucasians (10). Factor V Leiden, a common and well-known prothrombotic mutation in Caucasians has very low prevalence in Korea (21). These known and unknown differences are sure to have influence on how a drug like enoxaparin will behave in different populations.
We sought independent factors associated with effective aFXa levels at 4 hr and 12 hr. Those two times were chosen because at 4 hr, the aFXa would be at its peak activity and aFXa at 12 hr has been shown to correlate with clinical efficacy (13, 22). At 4 hr, none of the factors examined were associated with effective aFXa levels while at 12 hr, independent factors that negatively influenced achieving effective aFXa levels and SOFA scores and hyperbilirubinemia. These results are similar to those of Mayr et al. (4) which reported that enoxaparin was less effective in achieving the target aFXa levels among ICU patients with high multiple organ dysfunction scores. Hemodynamic instability is more common in patients with multi-organ dysfunction, and use of a vasopressor may compromise enoxaparin metabolism by reducing skin blood flow and drug absorption (4, 18, 23). Moreover, organ dysfunction itself may alter drug metabolism by affecting the absorption, distribution, biotransformation and excretion of the agent. Severe subcutaneous edema which may also decrease enoxaparin absorption, decreases in extracellular pH, altered albumin binding, and increase in any number of acute phase reactants may further influence drug pharmacokinetics (4, 18). Additionally, hyperbilirubinemia, which is one of the components of SOFA score, may interfere with color detection and give inaccurate aFXa readings (24).
Unlike previous studies, this study did not find significant association between body weight and aFXa levels. Mayr et al. (4) reported that high body weight is associated with lower aFXa levels, and Kessler et al. (25) reported that aFXa levels were progressively lower as body weight increased in patients receiving ardeparine sodium. In patients with high body weight, reduced blood flow to adipose tissue is thought to result in decreased absorption of drugs administered by subcutaneous injection. However, Asians tend to be slender and extreme obesity is far less common in Asians. In this study, the median body weight was 57 kg, and individuals weighing more than 90 kg were not included.
When interpreting the results of this study, it should be noted that aFXa level is not a direct measurement of the efficacy of thromboprophylaxis, but is only a surrogate marker and can only be considered a research tool. Although Levine et al. (13) demonstrated a relationship between aFXa level and anticoagulant clinical efficacy, some argue that aFXa levels are not ideal for assessing anticoagulant effects (26, 27). Furthermore, just increasing the dose of enoxaparin based on the low aFXa levels shown in this study could result in higher incidence of bleeding complications. Thus, further studies on the efficacy of thromboprophylaxis measuring clinically important outcomes are needed to resolve this issue.
This study has several limitations. First, it was a single center study, thus limiting its external validity. To better address the findings presented here and compare them to findings in other Korean critically ill patients in different settings, further large prospective studies are needed. Second, as noted above, we assessed surrogate marker increased of direct measurement of drug concentration or firm clinical end-points. Third, only 55 of 315 patients initially screened were included in the study limiting generalizability of our findings to patient groups who were not included in the study. Finally, this study did not have a control group and our findings cannot be generalized to patients who are not critically-ill.
However, this study has several strengths. First, this is the first prospective study to address the adequacy of once daily fixed dose enoxaparin for preventing VTE in Asian critically ill patients. Because prophylaxis of VTE is an important issue for critically ill patients, the results of this study are highly relevant for intensivists caring for patients of Asian ethnicity when deciding whether to use fixed dose enoxaparin for the prevention of VTE. Second, previous studies were conducted in mixed ICU or surgical patients (4, 5, 19, 28), and there are no studies being conducted in medical ICU patients. Our study targeted only medical patients, and will give useful information to patients with medical conditions.
In conclusion, once daily dose of 40 mg of enoxaparin is inadequate for maintaining effective antithrombotic aFXa levels for a period of 24 hr among Korean medical ICU patients, and the inadequacy is more salient for patients with high SOFA scores and hyperbilirubinemia. Further studies on the efficacy of thromboprophylaxis measuring clinically important outcomes are needed.


 XML Download
XML Download