

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary bifurcation lesions constitute a complex anatomy subset that is encountered in 15-20% of all percutaneous coronary intervention (PCI) (1). The trans-femoral (TF) approach is the usual and preferred vascular approach method used in PCI for coronary bifurcation lesions in most catheterization laboratories. However, significantly higher rates of local vascular complications have been reported in patients undergoing TF catheterization (2).
Compared with the TF approach, trans-radial (TR) PCI is associated with similar procedural success rates and clinically significant reductions in procedure-related bleeding complications (2-5). Thus, the TR approach is increasingly recognized as an alternative to the routine use of the TF approach (2, 4, 6). However, owing to practical, patient, and technical problems, the implementation of TR approach has remained limited in more complex coronary lesion subsets, such as coronary bifurcation lesions. There are limited data regarding the efficacy and safety of the TR PCI for coronary bifurcation lesions. The purpose of this study was to compare the impacts of the TR and TF approaches on efficacy and safety in patients with coronary bifurcation lesions.
MATERIALS AND METHODS
Study population
We conducted this study using the Coronary Bifurcation Stenting (COBIS) Registry. The methods and patient population of the COBIS registry have been described previously (7). Briefly, the COBIS registry is a retrospective multicenter registry dedicated to bifurcation lesion PCI that includes data for patients treated at 16 major coronary intervention centers in Korea. Inclusion criteria were: 1) coronary bifurcation lesions which were treated solely with at least 1 drug-eluting stent (DES) between January 2004 and June 2006; and 2) a main vessel diameter ≥ 2.5 mm and side branch diameter ≥ 2.0 mm. Exclusion criteria were the presence of cardiogenic shock, ST-segment elevation myocardial infarction (MI) within 48 hr, and left main coronary artery bifurcation lesions. Among 1,668 patients, a total of 753 patients were available for analysis of in-hospital bleeding. The registry was sponsored by the Korean Society of Interventional Cardiology.
Procedural details
The vascular approach method was decided by the operator's discretion for each patient. Intravascular ultrasound (IVUS) guided stenting was encouraged to achieve optimal stent expansion and lesion coverage. Stent type was selected per the treating physician's discretion at the time of the study, namely, sirolimus-eluting Cypher stent (Cordis, Johnson & Johnson, New Brunswick, NJ, USA), paclitaxel-eluting Taxus stent (Boston Scientific, Natick, MA, USA), and other. Stent techniques to treat coronary bifurcation lesions included: main vessel stenting only, T-stenting, crush, V-stenting, culotte, and other. Final kissing ballooning (FKB) was performed in cases with suboptimal results after crossover stenting at the ostium of the side branch and, in cases with 2-stent implantations.
All patients were administered loading doses of aspirin (300 mg) and clopidogrel (300 to 600 mg) or ticlopidine (500 mg) before coronary intervention, unless they had previously received these antiplatelet medications. During the procedure, anticoagulation therapy was performed according to current practice guidelines by the Korean Society of Interventional Cardiology (8), and use of glycoprotein IIb/IIIa inhibitors was determined by the operator. After procedures, aspirin was prescribed indefinitely and clopidogrel or ticlopidine was prescribed for at least 6 months.
Patient follow-up
Demographic, clinical, angiographic, procedural, and outcome data were collected with the use of a web-based reporting system. Additional information was obtained by further inquiries into medical records or telephone contact if necessary. All baseline and procedural cine coronary angiograms were reviewed and qualitatively analyzed at the angiographic core laboratory in the Cardiac and Vascular Center, Samsung Medical Center, Seoul, Korea. All patients were evaluated by a clinic visit or by phone at 1, 3, 6, and 12 months and annually thereafter.
Definition and study end points
Baseline bifurcation anatomy was assessed according to the Medina classification (9). Medina type (1.1.1), (1.0.1), and (0.1.1) lesions were defined as true bifurcation lesions. Angiographic success was defined as the achievement of a Thrombolysis In Myocardial Infarction (TIMI) flow grade of 3 with a final residual stenosis of < 30% for the main vessel or < 50% for the side branch by visual estimation. Procedural success was defined as angiographic success without in-hospital death, MI, or emergent coronary artery bypass surgery. After PCI, elevations of the creatine kinase-myocardial band greater than 3 times the upper limit of normal, assuming a normal baseline biomarker value, were considered indicative of peri-procedural MI (10).
The peri-procedural period included the first 48 hr after PCI. Peri-procedural complications were defined as the occurrence of coronary arterial dissection or abrupt closure during PCI, cardiac death, emergent bypass surgery, coronary perforation or cardiac tamponade during PCI. Death that could not be attributed to non-cardiac etiology was considered cardiac death. MI was diagnosed by electrocardiographic changes and/or a rise and fall of cardiac biomarkers in the presence of ischemic symptoms that were not related to the index procedure during follow-up. Target lesion revascularization (TLR) was defined as any repeated PCI or bypass grafting surgery to treat a luminal re-narrowing in-stent or within a 5 mm border adjacent to the stent. Target vessel revascularization (TVR) was repeat revascularization of the target vessel by PCI or bypass graft surgery. Stent thrombosis was adjudicated according to Academic Research Consortium definitions as definite, probable, or possible (11). Bleeding events were evaluated during hospitalization and characterized according to TIMI study criteria (TIMI major, TIMI minor bleeding), in addition to any reported bleeding (12). Additionally, the amount of bleeding was measured by changes in hemoglobin or hematocrit pre- and post-intervention.
The primary objective of our study was to compare long-term major adverse cardiac events (MACE) between patients treated by TR and TF approaches. MACE was defined as the occurrence of cardiac death, MI, and TLR in hospital and during follow-up.
Statistical analysis
Patient demographics, clinical, angiographic, and procedural characteristics were described in the TR and TF groups using means for continuous variables and frequencies for categorical variables. Proportions were compared between groups using chi-square test and Fisher's exact test as appropriate. Group means were compared using Student's t test. Cumulative event rates were estimated by the Kaplan-Meier method and assessed by the log-rank statistic. Differences in the incidence rates of individual clinical outcomes and composite outcomes between TR and TF groups were investigated by multivariable Cox proportional hazards models after confirming that the proportional hazards assumption was met. Adjusted hazard ratios and their 95% confidence intervals were estimated with potential confounders entered as covariates (age, sex, diabetes, chronic renal failure, clinical presentation of acute coronary syndrome, FKB, periprocedural complications, and TR approach). To reduce selection bias for approach type and potential confounding, a 1:1 matched propensity score analysis was performed. Propensity scores were calculated using all variables listed in Table 1, and estimated using multiple logistic regression analysis. The TR patients were ordered and sequentially matched to the nearest unmatched TF patients according to the estimated propensity score. We assessed the balance in baseline covariates between the 2 groups in a propensity score-matched population. The discrimination and calibration abilities of the propensity score model were assessed using the c-statistic and the Hosmer-Lemeshow statistic. Additionally, to determine whether similar outcomes between the 2 groups were consistent in the various subgroups, we performed subgroup analyses. The ten pre-specified subgroups were age (<75 or ≥75 yr), sex, diabetes mellitus, acute coronary syndrome versus stable angina patients, and left ventricular ejection fraction (<50 or ≥50% by 2D-echocardiography), true bifurcation, guiding catheter (≤6 Fr or >6 Fr), IVUS, 2-stent technique, and FKB. All analyses were conducted using SPSS software, version 17 (SPSS Inc., Chicago, IL, USA), and 2-tailed P values of 0.05 or less were considered statistically significant.
Ethics statement
This study was approved by the institutional review board (IRB) of Samsung Medical Center (IRB approval number: 2007-04-042). In addition, the local IRB at each participating hospital approved this study and waived the requirement for informed consent for access to each institutional PCI registry.
RESULTS
Among 1,919 patients registered, 251 patients failed to fulfill the inclusion criteria as determined by core laboratory cineangiographic analysis and were excluded. A total of 1,668 patients were included in this study. TR PCI was performed in 503 (30%) patients and TF PCI was performed in 1,165 (70%) patients.
Baseline clinical, angiographic, and procedural characteristics
Overall Population: Baseline clinical characteristics are represented in Table 1. Significant differences in clinical characteristics were found between patients treated by the TR approach and those treated by the TF approach. Overall, patients in the TR group were less likely to have dyslipidemia, peripheral artery occlusive disease, and chronic renal failure, and were less likely to present with acute coronary syndrome.
Angiographic and procedural characteristics are shown in Table 1. There were also significant differences in angiographic and procedural characteristics between the two groups. Types of bifurcation defined by Medina classification were significantly different between the two groups. The prevalence of true bifurcation and glycoprotein IIb/IIIa inhibitor administration tended to be higher in the TR group but the differences were not statistically significant. In contrast, the rates of IVUS guidance, and use of the 2-stent technique were significantly higher in patients treated with a TF approach. FKB, however, was performed more frequently with TR access. For TR patients receiving 2-stents for PCI (10.9%, 55 patients), bifurcation stent techniques included T-stenting (85.5%), crush (7.2%), culotte (1.8%), and V-stenting (5.5%). Among TF bifurcation cases treated with a 2-stent strategy (20.3%, 236 patients), techniques were T-stenting (39.8%), crush (40.3%), culotte (3.0%), and V-stenting (16.9%). Total stent length in the main vessel was longer in the TF than TR group.
Propensity-Matched Population: After performing propensity score-matching for all patients, a total of 424 matched pairs of patients were created (Table 1). The c-statistic for the propensity score model was 0.869, which indicates good discrimination. There were no significant differences in the baseline clinical, angiographic, and procedural characteristics for the propensity-matched subjects except for prevalence of dyslipidemia, glycoprotein IIb/IIIa inhibitor use, and guiding catheter size.
Procedural and clinical outcomes
Overall Population: Despite differences in baseline characteristics, the overall procedural success rates were high and were similar between the two approaches (Table 2). The difference between the two groups in the occurrence of peri-procedural complications and peri-procedural MI were not statistically significant, although there was a tendency for more frequent occurrence of peri-procedural MI in the TR than TF group.
Complete clinical follow-up data were obtained for 97.8% of the overall patients with a median follow-up of 672 days (interquartile range 437-965 days), although the follow-up period was longer for TR patients (median 721 days vs 661 days, P<0.01). There were no significant differences in rates of MACEs (5.2% vs 7.0%, P=0.11, Fig. 1A), or individual endpoints, including cardiac death or MI (1.8% vs 2.2%, P=0.45), and TLR (4.1% vs 5.2%, P=0.22) between the TR and TF groups, respectively. Definite and probable stent thrombosis rates were also similar between the TR and TF groups (0.6% vs 0.5%, P=0.77). However, TVR rates were lower in TR group than in TF group (4.4% vs 6.9%, P=0.04). All hazard ratios and 95% confidence intervals for clinical endpoints were subjected to multivariable adjustment (Table 3). The TR approach was not an independent predictor of MACEs, cardiac death or MI, and TLR during follow-up.
Propensity-Matched Population: Procedural success rates in the main vessel were similar between the two groups, but procedural success rates in the side branch were lower with the TR approach than with the TF approach. Periprocedural complications occurred more frequently in the TF group (1 cardiac death, 3 emergent bypass surgery, and 3 coronary arterial dissection or abrupt closure during PCI) than in the TR group (1 cardiac death) (Table 2). There were also no significant differences in rates of MACEs (4.5% vs 6.8%, P=0.09, Fig. 1B), cardiac death or MI (1.4% vs 2.4%, P=0.32), TLR (3.3% vs 5.4%, P=0.09), or stent thrombosis (0.5% vs 0.5%, P=0.87) between the TR and TF groups. However, TVR rates were lower in TR group than in TF group (3.8% vs 7.1%, P=0.02). Even after multivariable adjustment in the propensity score-matched patients, the TR approach was not an independent factor predicting endpoints during follow-up (Table 3).
Bleeding events
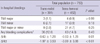
Among a total of 1,668 patients, records of in-hospital bleeding events were collected in 753 patients. When bleeding events were characterized according to TIMI study criteria, no differences were observed in the rates of in-hospital bleeding events between the TR group and the TF group, even though the amount of bleeding measured by changes in hemoglobin (-0.63±1.20 g/dL vs -0.93±1.28 g/dL, P=0.01) or hematocrit (-1.97±3.53% vs -3.00±3.88%, P<0.01) was significantly smaller in the TR group than in the TF group (Table 4).
Subgroup analysis
In subgroup analysis, there were no significant interactions between the effects on MACE of the vascular approach types (TR or TF) and the eight pre-specified subgroups of age (<75 or ≥75 yr), sex, diabetes mellitus, acute coronary syndrome versus stable angina patients, and left ventricular ejection fraction (<50 or ≥50% by 2D-echocardiography), guiding catheter (≤6 Fr or >6 Fr), IVUS and 2-stent technique (Fig. 2). However, there was a tendency for significant interactions to exist between the presence or absence of true bifurcation lesions and MACE (P for interaction=0.06). While the MACE rate was not significantly different between the groups in true bifurcations lesions, the MACE rate was substantially lower in the TR group than in the TF group among patients with non-true bifurcation lesions. In addition, there was a significant interaction between FKB and MACE (P for interaction=0.01). MACE rate was significantly higher in the FKB group than in non-FKB group and the MACE rate was substantially lower in the TR group than in the TF group among patients without FKB.
DISCUSSION
There are few data comparing TR and TF approaches for the treatment of coronary bifurcation lesions in the DES era. To our knowledge, this study represents one of the largest surveys of TR PCI for coronary bifurcation lesions and the only comparative study of vascular approach methods for coronary bifurcation lesions.
The main findings of this study are: 1) TR PCI for coronary bifurcation lesion is associated with a high procedural success rate; and 2) TR PCI, compared with TF PCI for coronary bifurcation lesions, is associated with similar long-term clinical outcomes, even after propensity score-matched adjustment.
When compared with earlier studies (2), contemporary trials demonstrate no differences in procedural failure between vascular approach strategies for coronary intervention (5, 13-15). However, the expansion of TR PCI to more complex and high risk lesion subsets has been restricted by several limitations. This perception is especially relevant for coronary bifurcation lesions, considering the technical challenges of guiding catheter support, limitations of catheter size and often the simultaneous need for multiple angioplasty catheters. Even though there are limitations of TR PCI, procedural success rates in our study were similar between the two vascular approach methods, demonstrating the feasibility of TR PCI for coronary bifurcation lesions. The choice of interventional guiding catheter is influenced by the site of arterial access. Although radial artery size generally limits the arterial sheath to 6-French, advanced PCI devices, the increased inner diameter of guiding catheters combined with the decreased profile of balloons and stents have allowed bifurcation procedures through radial access. There were no differences in the procedural outcomes between the two vascular approaches for bifurcation PCI in our study. Similar procedural success rates may be attributed in part to techniques, such as provisional 1-stent technique, that are now regarded as standard techniques for most bifurcation PCI and are feasible through radial 6-French access, and the use of IVUS guidance (16, 17) which is not excluded by a TR approach.
TR PCI had a tendency to have more favorable long-term clinical outcomes than TF PCI, but the difference was not statistically significant in our study. Our results do not differ from those of larger comparative studies that established the relationship between TR PCI and decreased early- and late-term mortality (3, 18). Bleeding amounts measured by hemoglobin or hematocrit changes before and after PCI were lower in the TR group than in the TF group. While the in-hospital bleeding complication rates were not significantly different between the two groups, TIMI major or minor bleeding had a tendency to occur less frequently in the TR group than in the TF group in our study. These findings may in part be due to the tendency for lower MACE rate in the TR group than in the TF group in our study. Bleeding complications after PCI are associated with increased risk of post-PCI morbidity and mortality (19, 20). However, as our results are based on inadequate data, they should be interpreted carefully. FKB was more frequently performed in TR patients, which may account for the similar rates of MACEs between the two groups, even though there was a lower cardiac risk profile in TR patients. Our COBIS investigators previously suggested that FKB might be harmful for coronary bifurcation lesions treated with 1-stent technique mainly due to increased TLR (21).
We recognize that the present study has several limitations. First, comparisons to this analysis are limited by its non-randomized and retrospective design, in which operator bias and unmeasured confounders may preclude any definite conclusions, despite multivariable adjustment. However, we tried to overcome this limitation through propensity score-matching analysis. Second, we did not have data describing procedure time, contrast amount, radiation times, length of hospital stay, or data for the numbers or ratio of crossover between the TR group and TF group due to technical reasons. By way of example, crossover from TR to TF vascular approach is one of the important determining factors of procedural success during challenging PCI. Another important consideration is that there were insufficient data available for bleeding events. Among a total of 1,668 patients, records of in-hospital bleeding events were collected in 753 patients. These inadequate data might explain the lack of statistically significant differences in bleeding events between the two groups, even though changes in hemoglobin or hematocrit were significantly less in the TR group than in TF group. These results should be confirmed by a well designed large randomized trial.
In the present study, we evaluated the use of TR PCI for bifurcation lesions and compared our results with those for TF PCI. Compared with the TF approach, TR PCI for coronary bifurcation lesions is feasible and is associated with similar procedural success rates, as well as comparable long-term clinical safety and efficacy. Based on the results of the present study, we conclude that PCI with the TR approach is a good alternative strategy in coronary bifurcation lesions intervention.





 XML Download
XML Download