

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tension orbit is a clinical condition in which severe proptosis occurs with the intraorbital space compression that subsequently leads to severe stretching of the optic nerve and results in the deterioration of vision. This may be caused by trauma, infection, non-infectious orbital inflammation or tumors (1). Orbital cellulitis is one of the diseases known to cause tension orbit and occurs frequently through sinusitis, lid inflammation, dacryocystitis and hematogeneous spread of infection. Most of orbital cellulitis can be solved by antibiotics or surgical drainage without any complication. But complications such as extraocular muscle palsy, pupil dilation, rising of intraocular pressure and visual loss by optic nerve invasion can occur if the inflammation aggravates to cause severe intraorbital edema or spreads to orbital apex. Orbital cellulitis can also arise from odontogenic causes, even though its prevalence is rather infrequent, comprising only 2%-5% of all orbital cellulitis cases (2). In particular, cases of orbital cellulitis that had resulted in blindness are very rare. To our knowledge, there was no report thus far that shows typical tension orbit causing blindness in odontogenic orbital cellulitis.
We experienced a very rare case of odontogenic orbital cellulitis which caused the rapid progression to ischemic optic neuropathy and central retinal artery occlusion by severe tension orbit within a few days and consequently resulted in blindness in spite of antibiotic treatment. So, we intend to present the seriousness of such complications through this case.
CASE DESCRIPTION
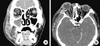
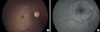
A 41-yr old male patient had visited our hospital due to symptoms of severe right facial and periorbital edema, proptosis, ocular pain, decreased visual acuity, diplopia and nasal stuffiness on June 11, 2011. The patient had dental root of the right upper premolar tooth broken accidentally 2 months ago. He endured the condition untreated until the pain became very severe. He visited a private dental clinic and was diagnosed with a periodontal abscess of the right upper premolar tooth 4 days before visiting our hospital. There he was treated with antibiotics, but swelling of the right mandible and cheek area began on the first following day. In addition, periorbital swelling, proptosis and nasal bleeding began on the second following day. The facial and periorbital swelling became more aggravated and the patient was referred to our hospital (Fig. 1A). The patient had no specific past medical history. From the ophthalmologic examination, his best corrected visual acuity was 20/100 for the right eye and 20/20 for the left eye. The intraocular pressure was 54 mmHg in the right eye and 12 mmHg in the left eye. In the examination of eyeball movement, his right eye had shown severe limitation of movement in all directions (Fig. 1B). Exophthalmometry was measured to be 20 mm in the right eye and 14 mm in the left eye. The right eyelid was very tight and tender at palpation. Severe conjunctival injection and chemosis were also observed. Because the right eyelid could not be closed completely due to proptosis, conjunctival prolapse was observed through the lid fissure. On the slit lamp examination, epithelial erosion and mild stromal edema of the cornea were observed. The anterior chamber of the right eye showed a center depth of 2.5 CT (corneal thickness) which was rather shallower than 4 CT in the left eye. But there was no floating inflammatory cell in the anterior chamber. At the time of the initial examination, pupillary response was normal and no abnormal finding was observed from fundus examination. The color vision test was also normal. In facial CT, findings of severe sinusitis in the right maxillary sinus and inflammation of the right temporalis and mastication muscles were observed. Also, findings of severe inflammation in orbital soft tissue and extraocular muscles, which is correspond with the findings of orbital cellulitis, were observed (Fig. 2A). Increase in leukocyte count, erythrocyte sedimentation rate, and C-reactive protein level were found in the blood sampling test. Upon diagnosis of orbital cellulitis spreading from odontogenic sinusitis, the patient was immediately hospitalized. Intravenous administration of ceftriaxone and clindamycin began with medications for lowering intraocular pressure. The intraocular pressure of the right eye had decreased to 34 mm Hg on the following day of hospitalization. However, the facial and periorbital swelling had not improved and further aggravated. Therefore, emergent maxillary sinus drainage was performed in the department of otolaryngology. On the day following surgery, the patient complained of a sudden deterioration of vision in the right eye. The measured visual acuity was only light perception and intraocular pressure was 42 mmHg with afferent pupillary defect in the right eye. Pale optic disc, cherry red spot in the fovea and retinal edema were found from the fundus examination (Fig. 3A). In fluorescein angiography, delay of retinal circulation was observed (Fig. 3B). Ischemic optic neuropathy and central retinal artery occlusion were diagnosed by these findings. Severe proptosis and deformation of the posterior pole of the right eye into a cone shape by severe stretching of the optic nerve were found in the orbital CT (Fig. 2B). Immediate ocular massage, emergent anterior chamber paracentesis and lateral canthotomy were performed. However, those trials were useless. While maintaining ocular hypotensives and antibiotics, the intravenous administration of high-dose steroid (methylprednisolone, 1 mg/kg/day) started. After 5 days, the intravenous steroid was replaced with oral prednisolone at a dosage of 60 mg/day for 1 week and thereafter the dosage was gradually reduced. Meanwhile, Staphylococcus epidermidis was identified from a microbiologic culture at the time of sinus drainage. The patient began to show improvement of facial and periorbital edema after 5 days of hospitalization and the intraocular pressure had returned to normal range. After 12 days of hospitalization, proptosis, limitation of eyeball movement, and afferent pupillary defect had been resolved, but the visual loss had not recovered at all (Fig. 4).
DISCUSSION
Orbital cellulitis or subperiosteal abscess from odontogenic causes are relatively rare complications and these can occur along several pathways due to specific anatomic structure of facial bone. The first pathway is the most common one via the sinus because the roots of molar and premolar tooth are adjacent to the base of maxillary sinus, the infection of a tooth invades the maxillary sinus directly. Then the inflammation or infection of the sinus spreads into the orbit through bone erosion between the orbit and the maxillary sinus or through ethmoid sinus or infraorbital canals (3, 4). The second pathway is the one through the facial soft tissue over buccal cortical plate, spreading to periorbital tissues. The third pathway is the one that infection of a molar or premolar tooth invades the infratemporal and pterygopalatine fossa, spreading into the orbit through the inferior orbital fissure (4-6). Infection of a tooth can also spread into the orbit along the facial vein and the ophthalmic vein by hematogeneous regurgitation because the veins of the face, eyes, nasal cavity and sinus are all connected without valves (4). With regard to our patient, it is thought that the findings of severe sinusitis and widespread invasion to the cheek area demonstrate the correspondence with the aforementioned first and second pathways. There are normal floras such as Staphylococus epidermidis, S. aureus, Streptococcus salivarius, S. mutans, Lactobacillus sp., Eubacterium sp., and Bacteroides gingivalis in the mouth, which can cause infection (7-9). As S. epidermidis had been identified from the microbiologic culture of the patient, it was highly suspected that this complication was induced by odontogenic infection.
There are some case reports which described a visual loss from an odontogenic complication (10), but the cases had not shown typical findings of tension orbit and eyeball deformation caused by severe proptosis and optic nerve traction. The direct dissemination of infection to the optic nerve may be considered the possible cause of visual loss that occurred in our patient. Yet the argument of Dolman et al. (11) may reveal a more feasible cause of visual loss in our patient. Dolman et al. (11) stated that severe proptosis suddenly stretches the optic nerve and the central retinal artery, causing reduction of vessel diameter leading to the impairment of blood circulation. Additionally, severe intraorbital edema directly compresses the optic nerve as well as the nutrient vessel so as to trigger ischemic optic neuropathy and central retinal artery occlusion. In the orbital CT of our patient, we observed a very severely stretched optic nerve caused by severe proptosis that changed the eyeball posterior pole into a cone shape due to severe optic nerve traction. These findings are highly correlated with the mechanism of visual loss proposed by Dolman et al. (11).
Administration of high-dose steroid in the patient with infection can be controversial. But some authors reported that active administration of steroid at an early stage may be helpful for faster symptomatic improvement (12, 13). Although co-administration of high-dose steroid along with antibiotics did not aid in the recovery of vision in our patient, it is considered somewhat helpful for blocking further aggravation of inflammation.
Odontogenic orbital cellulitis is a relatively rare complication, but it can cause blindness via rapidly progressing tension orbit in spite of antibiotic treatment. Therefore even the simplest of dental problems require careful attention.


 XML Download
XML Download