

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Rheumatoid arthritis (RA) is a paradigm of chronic and inflammatory polyarthritis, particularly of the small joints of the hands and feet. RA causes joint swelling, pain, and bone and cartilage destruction leading to functional disability and reduced quality of life. In RA, osteoporosis occurs in two forms: periarticular osteoporosis around inflamed joints and generalized osteoporosis. Generalized bone loss may result from immobility, the inflammatory process per se, and treatments such as steroids. On the other hand, periarticular demineralization occurs because of local release of inflammatory molecules and is the earliest feature of RA, preceding bone erosion. It has been demonstrated that periarticular bone loss occurs before generalized osteoporosis.
Along with bony erosions and uniform joint space narrowing, periarticular osteoporosis is one of the imaging hallmarks of RA. Bone mineralization is usually normal in all arthropathies except RA. Nevertheless, radiographic changes were excluded in the new 2010 American College of Rheumatology (ACR)/European League Against Rheumatism classification criteria for RA. This is because periarticular demineralization is subjectively evaluated by a decrease in radiographic density in the osseous structure surrounding the joints and it is difficult to detect the apparent structural changes in the early stage of disease by conventional radiography. Although the new classification criteria is anticipated to identify RA at an early stage by the aid of anti-citrullinated protein antibody (ACPA) and rheumatoid factor (RF), physicians often are placed in an obstinate situation that a patient without RF, ACPA and evident radiographic changes is suspected to have RA. Because the marked radiographic changes including erosions and joint space narrowing appear over with time, early diagnosis is not easy in case of seronegative RA under the new 2010 classification criteria for RA. In seronegative RA, the quantification of periarticular osteopenia, which is a feature of early RA, could assist the identification of early RA.
Imaging findings provide an assessment of structural damage and help monitor the response to therapeutic intervention. Damage seen radiographically has been shown to be an important predictor of clinical outcome and progression (1). However, the radiographic definition of periarticular osteoporosis is obscure and the condition requires an optimal method for detection. Conventional radiography should be obtained on a single emulsion film, and digital radiographs must be obtained with appropriate parameters. Technical factors, such as film development, exposure, and soft tissue thickness, affect radiographic outcomes.
In the present study, we aimed to quantify localized hand bone mineral density (BMD) and convert this into a diagnostically applicable index. Our study was conducted in three steps. First, to evaluate subjective inconsistency, one radiologist and three rheumatologists reviewed X-ray images of hands to determine the presence of periarticular osteoporosis, and their interobserver agreement was evaluated. Second, we quantified the BMD of periarticular and shaft regions with dual-energy X-ray absorptiometry (DXA), calculated the ratio between the two, and compared ratios between RA and control subjects. Third, clinical information was collected to find conditions predisposing to the loss of juxta-articular bone minerals.
MATERIALS AND METHODS
Subjects
A total of 163 subjects were enrolled in our DXA-assisted hand BMD measurement study. To minimize the influence of comorbidities other than RA contributing to bone demineralization, our selection criteria excluded two populations: patients with a lumbar BMD Z-score of -2.0 or below based on DXA, and patients with complications owing to iatrogenic steroid consumption. Among the 12 excluded patients, one had Cushing's disease, another had avascular femoral head necrosis, and the others had a low Z-score. Forty five patients with RA and 106 control subjects, for a total of 151, finally remained for further study. Early RA was defined as patients with RA for 3 yr or less according to the 1987 ACR criteria. On the other hand, established RA was defined as patients with RA for longer than 3 yr according to these criteria. Control subjects consisted of 32 healthy subjects, 44 patients with osteoarthritis, 21 patients with ankylosing spondylitis, seven patients with Sjögren's syndrome, one patient with Behçet's disease, and one patient with gout. None of the control subjects showed any evidence of inflammatory arthritis. Clinical variables including disease duration, medication, and body mass index (BMI) were also noted. The bone turnover markers osteocalcin and C-terminal telopeptide were measured at the time of hand BMD measurement.
Evaluation of hand X-ray images
Three rheumatologists and one radiologist reviewed hand X-ray images from all the 151 subjects. The radiographic hand images were acquired using an AXIOM Aristos MX apparatus (SIEMENS, Erlangen, Germany). All the radiographs were exposed with an exposure voltage of 46.0 kV, current-time product of 4.11 mAs, exposure time of 11.3 ms, and exposure amount of 10.07 mR. All radiographs were obtained using the uniform digital technique of our institution. No postprocessing enhancement of bony detail was added. Each physician independently determined and recorded the presence or absence of periarticular osteoporosis. The physicians were blinded to patient identification, history, diagnosis, and their colleagues' interpretations. Interobserver agreement among four physicians was evaluated by Fleiss' ĸ value and agreement between two physicians was evaluated by Cohen's ĸ. The ĸ values were interpreted as poor (ĸ = 0), slight (ĸ = 0.0-0.2), fair (ĸ = 0.21-0.40), moderate (ĸ = 0.41-0.60), substantial (ĸ = 0.61-0.80), or almost perfect (ĸ = 0.81-1.00) (3).
Quantification of hand BMD by localized DXA
From the second to fifth digits of both hands, eight regions of interest (ROIs) on proximal phalanges were designated. The four ROIs were located on proximal periarticular regions, and the other four ROIs were on the narrowest cortical regions of shaft to serve as individual reference values (Fig. 1). A DXA Expert XL densitometer (Lunar, Madison, WI, USA) was used to scan both hands and all eight BMDs were expressed in g/cm2. Each ROI was manually identified and its size was uniformly confined to a width of 0.5 cm or a pixel size of 0.25. The total dose of radiation from scanning was 2.0 µGy. After DXA measurement, we labeled the left and right hands with L and R, respectively, followed by numbers from 1 to 4 for periarticular (peri) BMDs and 1' to 4' for mid-bone (mid) BMDs (Fig. 1). To combine BMDs of the peri and mid regions, we designed simple formulae as follows. Mathematical equations are expressed within brackets for the readers' convenience. An unknown quantity of x or x' is used in the equations to represent any of the peri or mid BMDs from finger numbers 1 to 4.
Mid-to-peri BMD ratio (= x'/x). The mid BMD was divided by the peri BMD of the same finger. Thus, the larger the mid-to-peri BMD ratio, the more prominent the periarticular osteoporosis is on the finger of concern. For example, the equation for the left index finger was L1'/L1.
Mean of four mid-to-peri BMD ratios (= [∑1 x'/x]/4). As an extension of the first formula, the mean of four mid-to-peri BMD ratios was calculated. The equation for the left hand was (L1'/L1 + L2'/L2 + L3'/L3 + L4'/L4)/4.
Ratio of the sum of the mid BMDs to the sum of peri BMDs (= ∑1 x'/∑1 x). All four mid BMDs of one hand were divided by four peri BMDs of the same hand. The equation for the left hand was (L1' + L2' + L3' + L4')/(L1 + L2 + L3 + L4).
These mathematical variations were intended to simplify the interpretation and to clarify the extent of periarticular osteoporosis based on multiple dimensions ranging from the fingers, one hand, and both hands. For further analysis, the RA group was divided into two based on the disease duration (early RA versus established RA).
Statistical analyses
Statistical analyses were performed using the SPSS statistical software package (standard version 16.0; SPSS, Chicago, IL, USA). When comparing the groups, a Student t test or one-way analysis of variance was used for continuous variables and a chi-squared test was employed for categorical variables. Correlations between variables were evaluated using Pearson's correlation test. Cut-off values were determined by receiver operation characteristic (ROC) curves. All results are expressed as mean and standard deviation unless otherwise specified. P < 0.05 (two-tailed) was considered significant.
RESULTS
Baseline characteristics
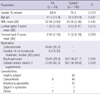
Baseline demographic and clinical characteristics in the study are shown in Table 1. All enrollees were Korean. Four patients in the RA group also had osteoarthritis (8.9%). A single case of comorbid systemic lupus erythematosus was also noted in the RA group. No other type of degenerative or erosive arthrosis on hands was documented in the RA group. There were no statistically significant differences in terms of gender, age, body mass index (BMI), or lumbar T-score. However, the T-score of the femoral neck was lower in patients with RA than in controls. The majority (95.6%) of patients with RA had been treated with corticosteroids, whereas none of the control subjects had been. Larger proportions of RA patients had been given calcium or vitamin D supplements (60.0% vs 40.6%).
Interobserver agreement for the radiographic detection of periarticular osteoporosis
Three rheumatologists and one radiologist individually determined the presence of periarticular osteoporosis based on conventional hand X-ray images. The ĸ value was 0.472, which signified a moderate degree of interobserver agreement among the four physicians (P < 0.001). More disagreement was found among the three rheumatologists, with their ĸ falling to 0.408 (P < 0.001). When a comparison was made with two physicians at a time-each rheumatologist's decision was compared with the radiologist's-Cohen's ĸ values varied from 0.464 to 0.646. We concluded that a physician's interpretation of periarticular osteopenia was prone to inconsistency, and this finding called for a more reliable method to identify the periarticular bone loss.
Quantification of hand BMD by DXA in the RA and control groups
The raw quantified hand BMD values were uniformly lower in RA patients regardless of its location, but this lacked statistical significance. To measure the BMD gap between the periarticular (peri) and nonperiarticular area, the peri BMD of one finger was subtracted from the mid BMD of the same finger, and the remainder was compared between two groups (=x - x'). Unexpectedly, this BMD gap was not higher in the RA group. We concluded that a direct comparison of BMD and the simple BMD gap measurement were insufficient for distinguishing between the RA and control groups.
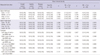
To avoid simple comparison of raw values and to set a value that reflects each person's background bone quality, we adopted the idea of an individually tailored BMD index and devised the aforementioned equations based on BMD ratios. Table 2 shows that the mean values of mid-to-peri BMD ratios tend to be higher in patients with RA (see the details under 1) in the Methods), although the difference was not statistically significant. As an extension from the previous ratio, the mean of mid-to-peri BMD ratios was calculated (see 2) in the Methods). Although the values tended to be higher in RA patients, the differences from controls also failed to reach statistical significance. To assess osteopenic changes from the perspective of a hand, all four mid BMDs of one hand were divided by the four peri BMDs of the same hand (see 3) in the Methods). Those values showed a similar result.
Distribution of the calculated values according to the intuitive interpretation of periarticular osteoporosis
Sixty-six of the 151 subjects displayed periarticular osteoporosis in their finger bones. Twenty-three (51.1%) of overall RA patients were interpreted to show periarticular osteoporosis in their hand X-ray. Periarticular osteoporosis was also diagnosed in 43 (40.6%) control subjects. Fig. 2 shows the each calculated values according to the interpretation of periarticular osteoporosis assessed by one expert radiologist. The mean value of L1'/L1, L2'/L2, L3'/L3 and L4'/L4 in the group of periarticular osteoporosis was 2.13, 2.11, 2.23, and 2.10, respectively. On the other hand, the mean value of L1'/L1, L2'/L2, L3'/L3, and L4'/L4 in the group of absence of periarticular osteoporosis was 1.68, 1.77, 1.96, and 1.84, respectively. The mean values between the two groups were significantly different in the all fingers (P<0.001).
Periarticular osteoporosis as a distinct feature of early RA
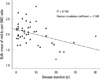
Overall control subjects were divided into healthy control (n= 32) and disease control (n=74). Table 2 demonstrats that the calculated values were not different between the healthy control group and the disease control group. For further analysis, the RA patients were divided into two subgroups according to the duration of their disease: 17 patients had early RA and 28 had established RA (as defined in the Methods). A post hoc analysis disclosed a more refined and significant difference from controls (Table 2). Patients with early RA revealed much higher values than the control group for the mid-to-peri BMD ratios of both index fingers. The mean mid-to-peri BMD ratio and the ratio of the sum of mid BMDs to the sum of the peri BMDs were also higher for the left and for both hands of early RA patients. On the other hand, these values did not differ between the patients with established RA and control subjects. As Fig. 3 shows, the mean mid-to-peri BMD ratio for both hands was negatively correlated with RA disease duration (R2=0.158, Pearson correlation coefficient=-0.398). In summary, the relative radiolucency of the periarticular bone region was most marked in patients with early RA, and such distinction was reduced as the disease was prolonged.
Cut-off values for the quantified hand BMD ratios in RA patients
ROC curves were used to determine cut-off values of selected formulae, which were three means of the mid-to-peri BMD ratio, and three ratio of the sum of mid BMDs to the sum of the peri BMDs. The cut-offs of all six formulae were located between 2.06 and 2.08 in diagnosing early RA with sensitivities ranging from 47.1% to 52.9% and specificities from 68.7% to 73.9%. The formula with the highest specificity was the sum of both hands' mid BMD divided by the sum of both hands' peri BMD (sensitivity 52.9%, specificity 73.9%, positive predictive value 20.5%, and accuracy 71.5%).
Risk factors for periarticular osteoporosis
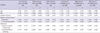
Clinical variables from the 45 patients with RA were collected to determine clinical conditions related to the loss of juxta-articular bone minerals. As Table 3 shows, BMI and RA duration were inversely correlated with the BMD formulae. In terms of steroid use, cumulative dose and treatment duration were negatively correlated with the formulae. C-terminal telopeptide, a serum biomarker used to measure the rate of bone turnover, showed a strong positive correlation with all six ratios. In our study, gender and administered medications were revealed to be unassociated with the six BMD formulae described above.
Correlation between periarticular bone mineral and generalized osteoporosis
As shown in Table 4, significant correlation was found between the left mid-to-peri BMD ratio and femoral bone density (BMD and T-score). Neither L-spine BMD nor T-score showed a significant correlation with periarticular osteoporosis. In contrast with the left hand, mid-to-peri BMD ratios of the right and both hands were not correlated with femoral and L-spine bone mineral loss.
DISCUSSION
We demonstrated that periarticular osteoporosis, as evaluated by DXA, is a prominent feature of early RA. Furthermore, relationships between the shaft-to-peri BMD ratio and steroid use, bone turnover marker, and RA disease duration were identified. Our study results show that a negative correlation exists between our BMD formulae and generalized bone density (femur).
The structural changes of RA, including bone erosion and decalcification, are conventionally believed to be irreversible. The development of biological agents, however, has dramatically altered the potential course of this disease and extended the therapeutic possibility toward a level of structural repair. Benefits seen radiographically after anti-tumor necrosis factor treatment have been reported after prospective and individual case studies (4-6). Because it has been recognized that early therapeutic intervention improves clinical outcomes and reduces the accrual of joint damage and functional impairment, early diagnosis and therapeutic intervention have become important goals for rheumatologists (7, 8). For this reason, prompt detection of bone mineral loss may be critical for superior functional outcome (9).
However, bone mineral wasting is silent, and the clinical definition of periarticular osteoporosis is very subtle. Its detection has been empirically notorious with high observational variation (10). Our analysis also revealed that the visual perception of periarticular radiolucency is frequently liable to misinterpretation. Because human eyes cannot conserve the "absolute pitch" of bone density, a more objective method for the assessment of periarticular BMD loss has been a latent question for physicians.
One of the first attempts in answering this question was reported by Deodhar et al., who measured whole hand BMD of 56 RA patients with DXA (11). The concept of quantification of periarticular osteoporosis was developed over several trials with variations in ROIs and quantifying instruments (9, 12-14). Considering that RA involves about 1% of the population and hand bone destruction occurs in fewer people, it is plausible to make a case-sensitive method, if not supported by a large-scale age-matched reference population within an ethnic group of concern. We conducted this study on the assumption that periarticular osteoporosis is relative, comparing it with that of the phalangeal bone shaft. To our knowledge, this is the first report of a study of patients with RA that directly compares periarticular BMD with that of the shaft in the same finger bone. Our present study is also the first to report the design of three types of BMD formulae to render an individually tailored assessment of periarticular BMD loss in patients with RA. Quantification of localized hand BMD revealed that periarticular osteoporosis was indeed present in proximal phalanges of RA patients. The uniformly high ratios in RA can be interpreted as an ascertainment of periarticular bone loss and the compensatory accentuation of density of the remaining area. Our study results show that absolute periarticular BMD is not correlated with RA disease duration. Some studies show that periarticular BMD decreases as the disease progresses (15, 16). On the other hand, other studies show that periarticular BMD does not differ between early and established RA (17). The majority of previous studies that assessed periarticular BMD according to disease duration measured periarticular BMD only. They did not consider the BMD of the bone shaft. The present study conclusively determined that DXA-assisted relative periarticular osteoporosis is an apparent character of early RA.
Interestingly, systemic bone loss may dilute the early emphasis on localized loss of bone minerals. Dilution of the disease hallmark can be theoretically explained by low BMD of generalized skeletal structures. As the disease progresses, patients with RA are exposed to inflammatory stimuli and tend to receive high doses of steroids for long periods. Thus, they inevitably undergo systemic bone loss. This expectation is evident in the decreasing BMD ratio as RA elapsed, as shown in Fig. 3. A longitudinal study of 29 RA patients also reported that hand bone loss was most distinctive in the first 3 yr of their disease (18).
Few clinical risk factors are known to be associated with periarticular BMD decline in RA patients. BMI, disease duration, and the cumulative dose of steroids demonstrated a significant correlation with periarticular osteoporosis in our present study. Even though RA duration and steroid treatment are well known to be major risk factors for systemic osteoporosis, their influence on local bone minerals requires further deliberate prospective studies. Bisphosphonate and calcium supplements were not related to favorable hand BMD ratios, thus their use in RA patients should be aimed at systemic benefits rather than local bone protection (19).
In this study, BMD ratios in the left hand of patients with early RA showed significant differences from those of control subjects. However, those in their right hands did not. We postulate that mobility is a possible negative risk factor for periarticular osteoporosis. The majority of Koreans are right handed. Discrepancies in motor function because of handedness (20) and hand-exploiting occupations (21) have been previously reported to affect hand bone density. In this context, the BMD discrepancy between right and left hands in our data can be interpreted as a bone protective effect of habitual loading.
Potential limitations of our study are the putative effects of gender and the use of medications. Pharmacologic effects on hand BMD are difficult to evaluate because each individual was exposed to a distinct regimen that varied in type of drug, dosing, duration, and clinical response. A randomized controlled study with a detailed stratification in medications would provide stronger evidence while minimizing these limitations. Nevertheless, our study attempts to raise awareness of objective methods to detect periarticular bone mineral loss in early RA.
Our findings suggest that bone mineral loss from periarticular regions precedes diffuse osteoporosis and is a distinct feature of early RA. Conclusively, DXA could play a potential role in the detection of periarticular osteoporosis, and thus the earliest radiographic changes in RA.


 XML Download
XML Download