

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
So-called "common mental disorders" like depressive and anxiety disorders are important concerns in communities. They are important public health issues in that they are prevalent throughout communities and inflict a significant loss in daily functioning (1); furthermore, they tend to go undetected and undertreated because of low awareness and a still-prevalent stigma of mental disorders (2). Many community mental health workers are continually working to promote awareness of depressive disorders among the public.
Surprisingly, epidemiological studies for mental disorders have reported a low prevalence of depressive disorders in Korea. Particularly, 2 nation-wide psychiatric epidemiological studies in Korea conducted in 2001 and 2006 confirmed a low prevalence of both major depressive disorder and dysthymic disorder. One-year prevalence estimates for major depressive disorder were 1.7% in 2001 and 2.5% in 2006. For dysthymia, the 1-yr prevalence was 0.3% and 0.4% in 2001 and 2006, respectively (3, 4). These studies used the Korean version of the Composite International Diagnostic Interview (CIDI; 5), so the results can be directly compared with the results from the National Comorbidity Study in the United States or the World Mental Health Survey. When compared with CIDI-based epidemiologic reports of mental disorders from other countries, the Korean prevalence of depressive disorder is quite low, especially when compared with Western countries (6). There is a unique pattern of prevalence of major depressive disorder in the Korean population, in that the geriatric prevalence is not lower than that of younger adults. Still, these estimates remain lower than that of the elderly prevalence in some Western countries (7). Although neighboring Asian countries such as Japan and China have similarly low prevalence of major depressive disorder, the low prevalence in Korea is still unexpected, because Korea also sports a high suicide rate, unlike its neighboring countries (8). China has recently reported relatively low suicide rate (9). Similarly, while Japan also has a considerably high suicide rate among OECD countries, the suicide rate is higher and the prevalence of depressive disorder is lower in Korea than in Japan. Thus, it may be possible that the low prevalence is because of a diagnostic threshold due to the categorical approach of diagnosing disease (10), rather than any protective factors of East Asian culture. Indeed, using the dimensional approach, the prevalence of depressive symptoms has been shown to be higher than the prevalence when assessed using the categorical (CIDI) approach (11).
It might be that Korea has prevalent subclinical or subthreshold depression, which often has enough symptoms but cannot achieve a formal diagnosis of depressive disorder according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth edition (DSM-IV), or the International Classification of Diseases, 10th edition (ICD-10). Major depressive disorder entails very severe functional loss (12). If subthreshold depression also has a similar disruption of functioning, then these subclinical symptoms might be a grave public health concern that has not yet been brought to the awareness of the public or clinicians. Several previous studies have focused on subthreshold depression (13-16), but few have reported on the situation in Korea. Thus, exploring the severity of functional impairment due to subthreshold depression in Korean society is paramount, in order to identify the reason for the low prevalence of formal depressive disorder and the high prevalence of depressive symptoms. This might explain the difference between the reported prevalence of major depressive disorder and the field experience of clinicians. In experience, many clinicians in Korea do not rely on formal diagnosis when deciding to initiate anti-depression treatment.
With backgrounds in mind, we examined the prevalence of depressive symptoms and formal depressive diagnosis in adult community-dwelling residents. In addition, we compared the functional disability of the subjects with only depressive symptoms (e.g. subthreshold depression) and subjects with DSM-IV diagnosis of major depressive disorder and dysthymic disorder.
MATERIALS AND METHODS
Study subjects
The sample of this study was collected during the community survey conducted by a community mental health center. This community mental health center is located in the urban center of Seoul and provides mental health services for a population of around 160,000. The community survey was designed to assess the mental health statuses of community residents between 18 to 64 yr of age. Using the household registry of the district office, we randomly chose 1,500 of the roughly 75,000 households in the coverage area. Trained interviewers visited those households in person, and among the residents who met the study enrollment criteria, interviewer select one person per household for interview according to randomization algorithm. Of chosen households, 210 households are either non-existent or inaccessible, so the final number that we made contact with was 1,290. Among these, 1,080 subjects or 83.7% of final sample list completed the interview, but data from 51 subjects was discarded as incomplete; thus, the final sample size was 1,029.
Identifying depressive symptoms and diagnosis of depressive disorder
The survey was conducted in 2 steps. First, trained lay interviewers conducted face-to-face interviews with all subjects. The interviewers were undergraduate students who were trained by a psychiatrist for this survey. With the help of Dong (basic urban administrative division of Korea) community centers, interviewers visited the homes of study subjects 1 week after the subjects had received a notification letter from the district health office. Subjects were interviewed using the Korean version of the Center for Epidemiological Studies Depression Scale (CES-D), and then the Korean version of the Mini International Neuropsychiatric Interview (MINI-K). The CES-D is a screening tool for depressive disorder, and has been translated into numerous languages and is used worldwide, including Korea (17, 18). Many countries, including the USA, use a score of 16 as the cut-off point to indicate that depressive symptoms are present; however, in the Korean version, the cut-off point for depressive symptoms is 21, and the cut-off for diagnosis is 25. The MINI-K is a semi-structured interview tool, and can be used to diagnose mental disorders according to DSM-IV criteria (19). This tool covers many of the DSM-IV disorders, and has been validated in the Korean language (20).
Those with significant depressive symptoms (e.g., CES-D scores over 21) were invited for another interview with a research psychiatrist. The psychiatrist interview was conducted within 10 days of the household survey. The research psychiatrist confirmed the diagnosis, and ruled out the possibility of other psychiatric disorders using the MINI-K and a clinical diagnostic interview. We used the diagnostic criteria of the DSM-IV in this interview. From this interview, subjects with major depressive disorder and dysthymic disorder were grouped as the depressive disorder group. Subjects who had CES-D scores over 21, but were not diagnosed with a formal depressive disorder (major depressive or dysthymic disorder) were categorized as the "depressive symptoms not diagnosable as depressive disorder" group.
Measurement of quality of life and work-loss days
We used the Korean version of the World Health Organization Quality of Life scale, abbreviated version (WHOQOL-BREF) to assess quality of life (21). This scale assesses subjects' quality of life across 4 domains: physical health, psychological health, social relationships, and environment. In this study, we used the abbreviated version with 26 items, the results of which can be converted into a 100-point scale. This scale does not have a cut-off point, and higher scores in each domain reflect higher quality of life. We also measured the functional disability of the subjects using the Korean version of the WHO Disability Assessment Scale, version 2 (WHODAS-II) (22). The WHODAS-II is a tool used to measure a person's functioning and disability levels in the last 30 days. It measures disability using various dimensions, including work-loss days. We used the composite index (Work Loss Day Index [WLDI]) from this scale, which has been used by several previous studies dealing with the relationship between work-loss days and common mental disorders (1, 23, 24). The WLDI was calculated by adding a half day per "cut back day" (H5) to the total loss days (H4), as described in Table 1.
Statistical analysis
We weighted the data with the district population's age and sex structure. The main comparison was done between the depressive symptoms group (who had depressive symptoms not diagnosable as DSM-IV major depressive disorder or dysthymic disorder) and the depressive disorder group, which included subjects with a DSM-IV diagnosis of major depressive disorder or dysthymic disorder. We compared the demographics between the 2 groups using chi-square tests. We compared functional disability and quality of life between normal, depressive symptoms, and depressive disorder subjects using analysis of variance (ANOVA) with Bonferroni post-hoc analysis. All analysis was done with SPSS version 19.
Ethics statement
Informed consent was obtained from every subject who participated in the survey. The analysis was done from a survey dataset that contained no personal identification information, and was exempted from institutional review board approval by the Seoul National University Hospital Institutional Review Board (E-1211-003-436).
RESULTS
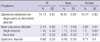
The weighted demographic profile of the study sample is shown in Table 2. The mean age of the sample was 40.1 yr, and the male to female ratio was about 1:1. About half of the study sample was married, and 12% of subjects were living alone. About half of the subjects had more than 13 yr of education, with 80% having income over the minimum cost of living. Of the study subjects, 17% of men and 6% of women were unemployed (excluding housewives).
Prevalence of depressive symptoms and depressive disorders
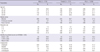
Table 3 shows that more than 17% of the study subjects had significant depressive symptoms, as defined by CES-D scores over 21. Women had a higher prevalence, at around 18.8%, compared with the 14.9% that men had. For men, teenagers and those in their 30s and 40s had a higher prevalence of symptoms; among women, teenagers and those in their 20s and 40s had a higher prevalence of symptoms (data not shown in the Table). We also observed reduced depressive symptoms after 60 yr of age.
Among these, we found that about 2.24% of the study sample had a major depressive disorder at the time of the diagnostic interview, and another 0.68% had dysthymic disorder. As expected, women had a higher prevalence of major depressive disorder than men (2.65% vs 1.75%, respectively). Single episode disorders were slightly more frequent than recurrent disorders. For dysthymia, the prevalence was 0.68%, and it was more common in women than in men. These results indicate that only 13% of all depressive subjects in the sample could be diagnosed with formal depressive disorders. The rest of the subjects with depressive symptoms were grouped as having "depressive symptoms not diagnosable as a depressive disorder." The prevalence of subjects who had depressive symptoms not diagnosable as a depressive disorder was 14.1%. Notably, while the formal disorders like major depressive or dysthymic disorder were more common in women, subclinical depressive symptoms were slightly more common in men (Table 3). We compared the demographic profiles between subjects with depressive symptoms and subjects with depressive disorders, and found no significant difference between those 2 groups (Table 4).
Table 5 and Fig. 1 show the pattern of quality of life and functioning across the spectrum of depressive symptoms. In all 4 domains, the normal group had the best quality of life scores, and the depressive disorder group the worst scores, with the depressive symptoms group in between. All 4 domains of quality of life were significantly different across the spectrum of depressive symptoms, according to the ANOVA. In the Bonferroni post-hoc analysis, the physical health, psychological health, and environmental domains showed a clear order of deterioration across the spectrum from normal to disordered subjects. In the social relationships domain, normal subjects had better quality of life compared with the other 2 groups, but there was no significant difference between the depressive symptoms and disorder groups.
For work functioning, the normal group had a mean of 4.6% work loss days according to the WLDI, meaning that they could not function properly for around 1.4 days per month. This increased to 17.2% or 5.2 days per month in subjects with depressive symptoms only. Finally, the depressive disorder group had 24.7%, or 7.4 days per month work loss. The means of the WLDI scores across the groups were significantly different, and post-hoc analysis showed significant between-group differences.
DISCUSSION
We have explored functional impairment and quality of life across the spectrum of depressive symptoms. The sample studied here was randomly chosen from information provided by an urban community mental health center in Seoul, and the response rate was quite robust; thus, it is likely that the results reflect the general characteristics of the adult metropolitan population of Korea.
The main findings of this study were that significant depressive symptoms that did not meet criteria for a DSM-IV diagnosis of major depressive disorder or dysthymic disorder were very prevalent among the community-dwelling adult population. In this study, the prevalence rates of major depressive disorder and dysthymic disorder were similar to the 12-month prevalence rates of these 2 disorders reported in a nationwide study (2.5% and 0.3%, respectively) despite the differences in interviewing tools (3). The prevalence of depressive symptoms was much higher: 1 in every 6 (approximately 17%) of the study subjects reported having significant depressive symptoms. This means that only 17% of subjects with significant depressive symptoms can be diagnosed as having a disorder, according to the DSM-IV.
These depressive symptoms inflicted significant functional loss, even when a formal diagnosis could not be made. The loss of work days in the depressive disorder group was 7.4 days per month on average, comparable with the 6.2 days from an earlier Korean report utilizing the CIDI and WHODAS II (25). However, even without a formal depressive disorder diagnosis, depressive symptoms were related to a higher loss of work, and in the pentagonal graph of functional impairment and quality of life status (Fig. 1), the depressive symptom group seems closer to the depressive disorder group, rather than the normal group. Thus, depressive symptoms that fail to reach a "disorder" status clearly still have both clinical and public health significance. This finding would justify interventions for those who do not meet the diagnosis for a DSM-IV disorder, but are still complaining of depressive symptoms. Of note, the average number of work loss days of those with major depressive disorder, according to the National Comorbidity Study (NCS) in the USA, was 2.6 days per month, indicating that in this study, the level of disability from major depressive disorder in Korea was quite high.
This finding is in line with previous studies exploring subthreshold depression or minor depressive disorder. Although not many studies have explored the quality of life and work functioning of those with subthreshold depression, there is growing evidence that depressive symptoms might be a risk factor for developing major depressive disorder (14, 26), and they might also have significant psychosocial impairment (27). In addition to the adult population, there are also growing concerns about the significance of subthreshold depression in both the adolescent (28) and elderly populations (29).
This significant disability due to subthreshold depression would be especially relevant in Korea. There might have been problems related to interviewing with trained but non-professional interviewers and the strictness of the CIDI criteria used in previous nationwide studies. However, in our study, the final diagnosis was made by a clinical diagnosis and the much less structured MINI-K, and the prevalence of depressive disorders was still low. In contrast, the prevalence of positive depressive symptoms was not low; we found it to be around 16.3%, according to the CES-D scores. Furthermore, we used a CES-D cut-off point of 21, which has been reported as optimal in Korea (18), but as other countries generally use cut-off points of around 16, the results between the present study and previous studies in other countries cannot be compared directly. However, a large nationwide community study using the CES-D in Korea had a cut-off score of 16, and reported that 25.3% of the sample had depressive symptoms (11); they pointed out that this was a higher prevalence than most reports from other countries that had a cut-off of 16.
These findings might constitute a "categorical fallacy" in the diagnosis of depressive disorders in the Korean population. Current operational criteria like the DSM-IV and ICD-10 are both categorical diagnosis. Subjects can only be classified as having a disorder or not. Screening questionnaires like CES-D are dimensionally oriented. The total score of questionnaires can be interpreted as a seriousness of symptoms. It is still debatable which approach-categorical or dimensional-is preferable for diagnosing common mental disorders (10). Our findings support the spectrum or dimensional approach to depressive illness, at least for community residents. One earlier study utilizing CES-D compared the usual simple scoring method for the CES-D with alternative scoring method, in which only "persistent" symptoms are counted in yes/no fashion. This categorical method using "persistence" is similar to the method used in DSM-IV or ICD-10. The study concluded that in a community, using the simple score method (e.g. dimensional approach) is more useful than categorical method (30). Indeed, the frequent "psychiatric comorbidity" among common mental disorders makes formal diagnostic criteria like the DSM-IV or ICD-10 less useful; in addition, many clinicians rely on symptom profiles rather than a strict diagnosis by formal criteria in deciding treatment options. However, health insurance and government policies still adhere to these diagnostic criteria, and these discrepancies between policy and clinician experience have created much confusion in the field. Some government officials and public media seem to discredit depressive disorder as an important cause of suicide because of the low prevalence of "formal" depressive disorders according to nationwide studies.
There are a few limitations in this study. Firstly, we performed a diagnostic interview only for subjects with CES-D scores over 21. We did this according to a recommendation from an earlier study about the use of the CES-D as a screening tool in a community (18), but we still might have missed people who could be diagnosable as having a depressive disorder, especially those who fell within the CES-D range of 16 to 21. However, since there were only 3 cases of major depressive disorder and 1 case of dysthymia according to the MINI-K results among subjects with CES-D scores below 21, this likely did not affect the results considerably. Secondly, as a cross-sectional study, we cannot really ascertain whether the disability and loss of quality of life was the result or the cause of the depressive symptoms or depressive disorders. Further longitudinal research is needed to elucidate the cause-effect relationship between depressive symptoms and disability.
In conclusion, significant depressive symptoms below the threshold of a DSM-IV diagnosis of major depressive disorder or dysthymic disorder are prevalent in Korea, and cause substantial loss of everyday functions and quality of life in community. Only a small proportion of these depressive subjects in community can be diagnosed as having a DSM-IV depressive disorder. This study provides some evidence favoring the dimensional approach to common mental disorders in community, and also supports the need for public mental health initiatives including early screening, education, and psychiatric interventions targeting subjects with mild depressive symptoms.




 XML Download
XML Download