

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Brain metastasis (BM) is a common oncologic problem. Historically, whole brain radiotherapy (WBRT) alone has been the most common treatment for patients with BMs, providing median overall survival (OS) of less than 6 months. Recently, invasive or highly technical treatments such as surgical resection, stereotactic radiosurgery (SRS), and fractionated stereotactic radiotherapy (FSRT) have been shown to improve long-term local tumor control of BMs and provide longer survival in some subgroups of patients (1-7). Although these treatments could provide long-term brain control for the remaining lifetime, they could represent overtreatment in patients with shortened survival times, typically the result of uncontrolled systemic disease. Thus, before performing invasive or highly technical treatments to address BMs, a useful prognostic index would be helpful in selecting the most appropriate treatment option for the individual patient and to properly stratify patients for future trials.
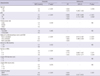
Many previous studies have reported that Karnofsky performance status (KPS), age, status of primary tumor and extracranial metastasis (ECM), and number of BMs as important factors in patients with BMs and several prognostic indices have been designed and tested in the patients with BMs as follow (Table 1) (8-15): 1) the Radiation Therapy Oncology Group (RTOG) recursive partitioning analysis (RPA), with three classes comprising combinations of four factors (age, KPS, and control of the primary tumor and ECM); 2) the Basic Score for BMs (BSBM), which is the sum of scores (0-1) for three prognostic factors (KPS, and control of the primary tumor and ECM); 3) the Score Index for Radiosurgery (SIR), which is the sum of scores (0-2) for five factors (age, KPS, status of systemic disease, number of BMs, and BM volume of the largest lesion); and 4) the Graded Prognostic Assessment (GPA), which is the sum of scores (0, 0.5, and 1) for four prognostic factors (age, KPS, number of BMs, and status of ECM) (Table 1). RPA and BSBM did not incorporate the number of BMs, SIR required a treatment factor (BM volume of the largest lesion at the time of SRS), and SIR and GPA did not consider the effects of the primary tumor status partly due to difficulties in objective assessment and separate evaluation of primary tumor and ECM status. However, both primary tumor and ECM status are important prognostic factors in patients with BMs, and thus it could be appropriate to evaluate status of combined primary tumor and ECM as constituent factor in prognostic indices rather than to neglect one of these factors or consider separately. In present study, to evaluate the role of status of combined primary tumor and ECM as constituent factor for prognostic indices, we retrospectively analyzed the prognostic factors in patients with BMs who were treated with radiotherapy (RT) for OS and compared the discriminating ability of several prognostic indices, i.e., RPA, BSBM, SIR, GPA, and modified prognostic index including the status of combined primary tumor and ECM.
MATERIALS AND METHODS
Patients
Between April 2003 and December 2009, 1112 consecutive patients with BMs received RT at the National Cancer Center (NCC) of Korea (Goyang). The diagnosis of BM was confirmed by brain magnetic resonance imaging (MRI) and/or computed tomography (CT). The inclusion criteria were: patients aged ≥ 20 yr; BMs from solid organ malignancies; no history of previous brain RT; and completion of the planned RT. A total of 899 patients met these criteria. Two patients who had BMs from malignant lymphoma were excluded. The remaining 897 patients were retrospectively analyzed.
The patient characteristics are summarized in Table 2. There were 453 men and 444 women, and the median age was 58 yr (range, 22-85 yr). The most common primary tumor sites were the lung (66.7%) and breast (20%). The most common histologies were adenocarcinoma (49.1%) and infiltrating ductal or lobular carcinoma (19.4%). The median time interval from the diagnosis of a primary tumor to the development of a BM was 12.2 months (range, 0-121.2 months). Of 897 patients, 548 (61.1%) had four or more BMs, and the median largest diameter of any brain lesion was 2.2 cm (range, 0.2-8.4 cm).
Treatment
At our center, the treatment of patients with BMs is based primarily on five factors: extent of the primary tumor and ECM, KPS, and size and number of BMs. Briefly, patients with progressive disease or poor KPS are generally recommended for treatment with WBRT alone, except for patients with symptomatic mass effects from the tumor. In those cases, patients generally undergo surgical resection followed by WBRT. Alternatively, patients with a stable primary tumor without ECM and good KPS are considered to be candidates for intensive treatment such as SRS, FSRT, surgical resection, or some combination of these. Based on these treatment guidelines, 725 of the 897 patients were treated with WBRT alone, 76 were treated with surgical resection + WBRT; 48, with FSRT; 37, with SRS; five, with surgical resection + FSRT; three, with WBRT + FSRT; and three, with WBRT + SRS. The median doses for WBRT, FSRT, and SRS were 30 Gy in 10 fractions, 36 Gy in six fractions (range, 15-54 Gy in 5-18 fractions), and 20 Gy in one fraction (range, 17.5-22 Gy), respectively. Details of the RT techniques were described previously (16).
Follow-up and statistical analysis
Patients were followed with serial neurological and radiological examinations. Follow-up MRI scans were usually obtained at 1 month and then at 3-month intervals, or in the event of unexpected neurological deterioration. Control of the primary tumor and ECM was defined as remission or stable disease, without any clinical, laboratory, or radiological findings suggestive of primary tumor or ECM progression, at 2 months before RT. The status of combined primary tumor and ECM was defined as follows: none controlled = uncontrolled primary tumor with ECM; one uncontrolled = uncontrolled primary tumor without ECM or controlled primary tumor with ECM; or both controlled = controlled primary tumor without ECM. Regarding to histological classifications, adenocarcinoma, infiltrating ductal or lobular carcinoma, non-small cell carcinoma, and squamous cell carcinoma were defined as 'favorable' histologies; other tumor histologies were defined as 'unfavorable.' For analysis, because invasive or highly technical treatments, such as surgical resection, SRS, and FSRT, have been shown to improve long-term local tumor control of BMs, patients were divided into two treatment groups: the WBRT group comprised patients treated with WBRT alone, and the Intensive Treatment (Intensive Tx) group consisted of patients treated with surgical resection + WBRT, SRS, FSRT, or combinations of these. Categorical variables included the following pretreatment and treatment parameters: age, KPS, primary tumor site, histology, status of primary tumor and ECM, time interval to BM, number of BMs, largest diameter of BMs, BM volume of the largest brain lesion, and treatment group (WBRT vs Intensive Tx). The prognostic indices (RPA, BSBM, SIR, and GPA) were considered to be ordinal variables.
Survival time was defined as the interval from the initial date of RT to the date of death. OS was calculated using the Kaplan-Meier method. Fisher's exact test was used to compare the distribution of pretreatment parameters between the WBRT and Intensive Tx groups. Correlations among five prognostic indices were assessed using Spearman's correlation coefficient test. The univariate analysis evaluating factors associated OS was performed by comparing OS rates using the log-rank test. For multivariate analysis to evaluate the prognostic values of pretreatment parameters, stepwise procedure was performed using Cox proportional hazards model containing various pretreatment parameters that attained or had a trend toward univariate statistical significance. In this procedure, forward selection of the parameter was processed by the scored chi-square test and the backward elimination by the Wald test. To compare the discriminatory prognostic ability of five prognostic indices with avoiding the problem of colinearity among these, Akaike information criteria (AIC) (17) were calculated; a smaller AIC value indicated a more desirable model for outcome prediction. The AIC statistic was defined as follows: AIC = -2 log (maximum likelihood) + 2 × number of model parameters, where the number of parameters equals one less than the total number of response levels plus the number of explanatory effects. All statistical tests were two-sided and were performed using STATA software (version 9.0; Stata Corp., College Station, TX, USA). Values of P < 0.05 indicated statistical significance.
RESULTS
Survival
Of the 897 patients, 819 (91.3%) patients had died at the time of the data analysis, and 78 (8.7%) patients were alive. The median follow-up time was 18 months (range, 5.1-63.7 months) for the surviving patients. The median survival times for all patients, the WBRT group, and the Intensive Tx group were 5.7, 4.9, and 10.6 months, respectively (P < 0.001). Table 2 compares the pretreatment parameters between the WBRT and Intensive Tx groups. Six potential prognostic factors (KPS, primary tumor site, status of combined primary tumor and ECM, time interval to BM, number of BMs, and BM volume of largest lesion) were not distributed equally between the two groups. A KPS ≥ 80, primary lung tumor, controlled primary tumor without ECM, time interval to BM > 24 months, single BM, and largest BM volume > 13 mL occurred with significantly higher frequently in the Intensive Tx group than in the WBRT group.
Analysis of factors associated with OS
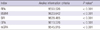
The results of the univariate and multivariate analyses for evaluating prognostic factors for OS are summarized in Table 3. Univariate analysis showed that all pretreatment parameters except histology, time interval to BM, largest diameter of BM, and BM volume of the largest lesion were significantly associated with OS (P < 0.05). In multivariate analysis, age, KPS, status of combined primary tumor and ECM, number of BMs, and treatment group were significant prognostic factors for OS (P < 0.05).
Basically, a prognostic index is developed from regression analysis to calculate the weighted relatives to the magnitude of significant prognostic factors, but four factors that were significant in the multivariate analysis were constituent variables of the GPA, one of well-known prognostic indices, and the aim of present study was to evaluate the role of the status of combined primary tumor and ECM as constituent factor in a prognostic index. Therefore, instead of developing a new prognostic index, we made a modified GPA (mGPA) which four factors, i.e., age (> 60, ≤ 60), KPS (≤ 60, 70, ≥ 80), the status of combined primary tumor and ECM (none controlled, one controlled, both controlled), and number of BMs (≥ 4, 2-3, 1), were used as constituent factors (Table 1). All five prognostic indices were all closely interrelated (mGPA vs RPA: r = 0.547, P < 0.001; mGPA vs BSBM: r = 0.617, P < 0.001; mGPA vs SIR: r = 0.727, P < 0.001; and mGPA vs GPA: r = 0.833, P < 0.001) and thus, to avoid the problem of colinearity among the five prognostic indices, we calculated the AIC value to compare the discriminatory abilities of prognostic indices, i.e., RPA, BSBM, SIR, GPA, and mGPA. All five prognostic indices, RPA, BSBM, SIR, GPA, and mGPA, were significantly associated with OS (P < 0.05 for each) (Fig. 1). The AIC value was lowest for mGPA and highest for BSBM (P < 0.001 for each) (Table 4). Based on the AIC values, mGPA had the best discriminatory prognostic ability for OS, followed by RPA, GPA, SIR, and BSBM, in that order. It implicated that modified score of pre-existing factors (i.e., age and KPS) and addition of the combined primary tumor and ECM status to the prognostic index could improve its' discriminatory ability and the combined primary tumor and ECM status might be useful as one of constituent factors for prognostic index.
DISCUSSION
Recent advances in imaging and RT technical procedures have improved the control of BMs in patients. A better understanding of the prognostic implications of pretreatment factors in patients with BMs would be useful to both clinicians and patients with regard to predicting survival and making appropriate treatment decisions. To date, KPS, age, status of primary tumor and ECM, and number of BMs have been considered to be the important prognostic factors for predicting OS (8-12). Our data also showed that these four factors were significantly associated with OS (Table 2). The sizes of BMs and interval to BM development have been proposed as possible determinants of OS. Primary tumor site, BM location, and histology have not been clearly shown to have a significant influence on survival (13, 14, 18-20). Regarding to the primary tumor sites, because cancer could behave differently in terms of patterns of progression and response to treatment according to the primary tumor sites, diagnosisspecific prognostic factors and prognostic index has been studied and proposed (13-15, 21). In the present study, patients with a primary breast tumor had a significantly better prognosis than patients with a primary lung tumor and other primary tumors in univariate analysis (7.1 vs 5.4 and 4.2 months, respectively; P = 0.044), but primary tumor site had no statistical significance in multivariate analysis. However, because other primary tumor sites, except for lung (66.7%) and breast (20%), was relative small (13.3%) in present study, we could not evaluate thoroughly the prognostic value of the primary tumor sites and thus further larger scale and comprehensive studies should be warranted.
Several prognostic indices (RPA, BSBM, SIR, and GPA) have been developed based on identified prognostic factors such as KPS, age, status of primary tumor and ECM, and number of BMs (8-12). One important application of prognostic indices is in making treatment decisions for individual patients. Thus, the discriminatory capabilities of prognostic indices for predicting OS are important, but this aspect of prognostic indices has not been thoroughly evaluated. The AIC value is a reliable statistical indicator useful in the search for an appropriate model; it compares model predictive values even when collinear factors are included. In our study, although all five prognostic indices (RPA, BSBM, SIR, GPA, and mGPA) were significant predictors of OS, an AIC analysis indicated that mGPA was the most discriminatory index for predicting OS, followed by RPA, GPA, SIR, and BSBM, in that order. The latter four indices have limitations that reduce their predictive ability. RPA and BSBM do not incorporate the number of BMs (0, 2-3, or ≥ 4), which was shown to be a significant prognostic factor in a randomized trial (1) and in our data. The status of both the primary tumor and ECM are significantly associated with OS, but to simplify quantification, SIR and GPA consider only ECM (none, stable, and progressive; and absent, or present, respectively). Although it is conceptually difficult to separate the influence of the primary tumor status from that of the ECM status, both factors contribute to OS. To address this, we classified the status of combined primary tumor and ECM into three groups (both controlled, one controlled, and none controlled) and showed that median OS differed significantly among these groups (13.4 months, 5.5 months, and 3.4 months, respectively; P < 0.001) (Table 3). Although the difference of median OS time between the groups of one controlled and none controlled was relatively smaller than that of between the groups of both controlled and one controlled, multivariate analysis consistently showed an increasing trend of hazard ratio among three groups of both controlled, one controlled, and none controlled (1, 1.825, and 2.534, respectively, P < 0.001) (Table 3).
Our data showed that the AIC value of mGPA including the status of combined primary tumor and ECM was lowest among the prognostic indices and suggested that, based on AIC value, mGPA had the best discriminatory prognostic ability for OS, followed by RPA, GPA, SIR, and BSBM, in that order. It implicated that addition of the status of combined primary tumor and ECM to the prognostic index could improve its discriminatory ability. For example, using RPA, BSBM, SIR, and GPA, 5% (45/897), 4.9% (44/897), 3.5% (31/897), and 9.3% (83/897) of the patients had a favorable prognosis with median survival time of > 12 months, respectively, whereas 20.4% (183/897) of the patients had a favorable prognosis with median survival time of > 12 months according to mGPA (Fig. 1). Thus, RPA, BSBM, SIR, and GPA appear to underestimate the prognosis of some patients. This means that some of the patients with a favorable prognosis based on mGPA may not receive treatment if RPA, BSBM, SIR, or GPA were used to determine prognosis. Recent advances in RT techniques provide improved long-term brain control and minimize toxicities, and thus the issue of patient selection has been become more important (4-7, 21). Proper stratification according to prognostic indices can help to identify subgroups that would benefit from invasive or highly technical treatments. Although our study did not stratify the patients by aforementioned prognostic indices, such as RPA, BSBM, SIR, GPA, and mGPA, and did not evaluate the effect of patient selection directly, our data suggests that all these prognostic indices could be helpful to identify subgroups that would benefit from intensive treatments for BMs and addition of the status of combined primary tumor and ECM to the prognostic index could improve its discriminatory ability.
Our study was retrospective and possessed certain inherent limitations. First, the present study involved a heterogeneous population representing a range of different primary tumors, from breast tumors to unusual primary tumors, and this can limit the interpretation of the OS analysis. Second, classification regarding to status of combined primary tumor and ECM (none controlled, one controlled, and both controlled) is a relatively subjective and/or uncertain process compared with determining ECM status alone (absent vs present). However, both the primary tumor and ECM status are important factors influencing OS, and prognostic indices considering both primary tumor and ECM status, such as mGPA and RPA, could provide better discrimination than GPA in our data. Thus, some subjectivity or uncertainty may be necessary in order to avoid excluding an important factor (control of the primary tumor). Finally, because present study retrospectively included heterogeneous patients treated with various treatments (i.e., intensive Tx, and/or WBRT) based on several pretreatment parameters (i.e., the status of the primary tumor and ECM, KPS, and size and number of BMs), not based on those prognostic indices, we did not evaluate the details of treatments, such as compliance of treatment guidelines, benefit of intensive treatments comparing with WBRT alone, etc., and the effect of patient selection using those prognostic indices directly. Thus, our results should be carefully interpreted and validated by more comprehensive and larger-scale studies.
In conclusion, it is suggested that age, KPS, primary tumor site, status of combined primary tumor and ECM, and number of BMs are significant to predict OS, and all prognostic indices, such as RPA, BSBM, SIR, and GPA, are significantly associated with OS. Additionally, our data suggest that modified score of pre-existing factors (i.e., age and KPS) and addition of the combined primary tumor and ECM status to the prognostic index can improve its discriminatory ability and the combined primary tumor and ECM status may be useful as one of constituent factors for prognostic index.



 XML Download
XML Download