

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Somatostatinergic tone (SST) can be defined as the inhibiting potential of somatostatin against the secretion of various hormones including GH. It was reported a positive correlation between pituitary tumor volumes and pre-surgical levels of GH (1, 2), and thus it may be assumed that an inappropriate SST response in tumoral status may also contribute to this relationship. However, few studies have documented how SST responses or varies with the size of pituitary adenomas because there has been no direct method developed to quantitatively measure SST. The very short half-life of endogenous somatostatin may complicate the development of such methods. Our previous study attempted to evaluate SST by performing the combined glucose and thyrotropin-releasing hormone (TRH) test. It was found that hyperglycemia suppressed TRH-induced TSH secretion by enhancing SST in healthy volunteers (3).
There are various methods available that measure GH level by manipulating glucose levels or adding somatostatin analogues. The oral glucose tolerance test (OGTT) and insulin tolerance test (ITT), for example, measure the variation in GH secretion due to changes in blood glucose levels. In addition, the octreotide suppression test (OST) is often used to predict the response to long-term treatment with somatostatin analogues or to verify their gastrointestinal tolerability (3, 4). All of these tests should inevitably accompany a change of SST secondary to either the change in glucose levels or the action of somatostatin analogues. Rapid inhibitory effect of hyperglycemia upon GH secretion may be due to somatostatin from hypothalamus (5), and it has been also suggested that this somatostatin release accompanies the modulation of SST (6). Therefore, the change in SST can be regarded as an intermediate link between glucose and GH secretion, and integrated analysis of the results of these tests could be a practical tool to evaluate SST in pituitary adenomas.
It is well known that the GH secretion in acromegalic patients is characterized by enhanced basal secretion (7). We hypothesized that one of the reasons for such changes in GH secretion profile in acromegalic patients may be due to the inappropriate SST response in tumoral status. There are currently no published reports regarding the analysis of SST according to the size of pituitary adenomas. The purpose of this study was to observe how SST responded in association with changes in glucose levels and how such responses differed according to tumor size. SST responses according to the responsiveness of macroadenomas to acute octreotide administration were also investigated.
MATERIALS AND METHODS
Patients
A total of 167 patients newly diagnosed with acromegaly at Kyung Hee University Hospital between 1991 and 2008 was initially screened. Among these patients, 29 patients (14 men and 15 women, aged 22-69 yr) who underwent both the ITT and the OST during the diagnostic work-up procedure for acromegaly were enrolled. None of these patients had received treatment before the study. The diagnosis of acromegaly was made when insulin-like growth factor-I (IGF-I) was above the age- and sex-adjusted reference range and an OGTT failed to suppress GH levels below 1 µg/L. Pituitary adenomas were identified in all patients by magnetic resonance imaging (MRI). Microadenoma was defined as an intrasellar tumor with a diameter less than 10 mm, and macroadenoma was defined as a tumor having a diameter greater than 10 mm and impinging upon adjacent sellar structures. All endocrine tests were performed on separate days. Blood samples from each patient were run in the same assay and in duplicate.
Oral glucose tolerance test
The OGTT was performed after an overnight fast. Patients had blood samples taken at baseline (0 min) and then at 30, 60, 90, and 120 min after drinking 75 g of a glucose solution. Blood was allowed to clot at room temperature for 15 min, after which the blood was centrifuged and the serum frozen at -80℃ in multiple aliquots. Fasting blood samples were assayed for IGF-I. Blood samples from all time points were assayed for GH levels.
Insulin tolerance test
Patients fasted overnight for at least 10 hr before undergoing the ITT. After sampling baseline GH levels, regular human insulin (RI) (0.15-0.20 U/kg) was administered intravenously with a target blood glucose level of less than 40 mg/dL (8). All of patients reached their blood glucose level below 40 mg/dL at 30 min. Additional insulin boluses were administered if needed to achieve the target glucose value unless the investigator believed this to be unsafe. Intravenous administration of dextrose was allowed if the patient experienced hypoglycemic symptoms. Patients had blood samples taken at 30, 60, 90, and 120 min. Blood samples from all time points were assayed for GH levels.
Octreotide suppression test
After an overnight fast, all patients had baseline blood samples taken for GH, and 100 µg of octreotide (Sandostatin®, Novartis, Basel, Switzerland) was then administered intravenously. Blood sampling for GH testing was continued every hour for four hours. Responders to the OST were defined as those whose nadir GH level was less than 2.5 µg/L during the test (9).
Measurement of GH and IGF-I
Serum GH concentration was measured before 2005 with commercial radioimmunoassay (RIA) kits (HGH 100T Kit, Nichols Institute Diagnostics, San Juan Capistrano, CA, USA). These assay standards and controls were calibrated against the first World Health Organization (WHO) International Reference Preparation (IRP) International Standard (IS) 80/505. Its sensitivity was 0.02 µg/L, and intra- and inter-assay coefficients of variation (CV) were 2.8%-4.2% and 3.5%-7.2%, respectively. Since 2005, commercial immunoradiometric assay kits to measure serum GH concentration were changed (hGH-RIACT, Cisbio Bioassays, Bedford, MA, USA). The sensitivity of this kit was 0.01 µg/L. The intra- and interassay coefficients of variation (CV) ranges were 1.3%-2.1% and 3.8%-5.0%, respectively. Standards and controls for this assay were calibrated against the second WHO IRP IS 98/574. In order to correct the discrepancy between these two assays, the previously reported correlation equation (y=0.6617x + 0.0692, R2=0.99) was applied (10). Serum IGF-I concentrations were also measured by commercial immunoradiometric assay kits (IGF-I NEXT IRMA CT, IDA S.A., Liége, Belgium). The minimum detectable concentration of IGF-I was 1.25 µg/L. The intra- and interassay CV ranges were 2.6%-4.4%, and 7.4%-9.1%, respectively.
Data analysis
We first compared GH levels between macroadenomas and microadenomas measured during the OGTT, ITT, and OST. GH levels during the ITT may represent the maximum GH secretory capacity of tumor cells and any remaining normal somatotrophs during insulin-induced hypoglycemia. On the other hand, the OGTT creates a hyperglycemic environment that suppresses GH secretion. We calculated ΔGHIO by subtracting GH levels measured during the OGTT from those measured during the ITT (ΔGHIO=GHITT-GHOGTT, at 0, 30, 60, 90, and 120 min). We assumed that ΔGHIO represents the amplitude of GH under the effect of SST which is enhanced by the glucose elevation during the OGTT, and the values were compared according to tumor sizes.
We also defined ΔGHOS as the difference in GH between the OGTT and the OST, calculated by subtracting the GH levels measured during the OST from those measured during the OGTT (ΔGHOS=GHOGTT-GHOST, at 0, 60, and 120 min, respectively). This measurement was used to investigate the extent of suppression of GH secretion not achievable only by hyperglycemia-induced SST during the OGTT but with additional other pharmacologic interventions such as somatostatin analogues.
Statistical analysis
Baseline characteristics were described as mean and standard deviation. The nadir GH levels during the OGTT and the OST were defined as the lowest GH at any time point during the two tests. The peak GH level during the ITT was defined as the highest GH at any time point during the test. Since the data were expected not to achieve the normal distribution due to the small sample size, we applied the non-parametric test such as the Mann-Whitney test for statistical comparison of age and BMI, basal GH and IGF-I, and peak and nadir GH levels during the tests between patients with macroadenomas and microadenomas. A linear mixed model (LMM) was used to compare GH levels between macroadenomas and microadenomas during the test. LMM was also used for the analysis of ΔGHIO, and ΔGHOS based on tumor size. All statistical analyses were performed with PASW (version 18.0; SPSS Inc., Chicago, IL, USA), and a P-value<0.05 was considered statistically significant.
RESULTS
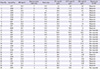
Twenty-two of 29 patients had macroadenomas (mean width 19.9±6.7 mm), and 7 patients had microadenomas (mean width 6.5±2.7 mm). It was found that only 50% of macroadenomas (11/22) could be classified as responders to the OST, whereas the majority of microadenomas (6/7) were responders (Table 1). Those with macroadenomas were mostly categorized as either grade III or IV of Hardy classification (11). In addition, 9/29 patients were diagnosed as having diabetes mellitus and 10/29 as prediabetes after their OGTT.
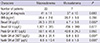
Age and BMI did not show any significant differences (Table 2) when comparing baseline characteristics by tumor size. Basal GH levels were significantly higher in those patients with macroadenomas (P=0.002), but IGF-I levels did not show significant difference based on tumor size (P=0.077).
Peak GH levels during the ITT were similar between macroadenomas and microadenomas (Table 2), and overall GH levels during the ITT did not differ according to tumor size (Fig. 1A). Nadir GH levels during the OGTT and the OST were significantly higher in macroadenomas than in microadenomas (Table 2; P=0.007 and 0.005, respectively). Such differences were examined at the nadir GH and during the entire test time during both the OGTT and the OST (Fig. 1B; P=0.028, Fig. 1C; P=0.033).
ΔGHIO in microadenomas during the entire test time showed a tendency to be higher than macroadenomas (Fig. 2A; P=0.066). A rapid elevation of ΔGHIO, peaking at 60 min and declining afterward (-1.2 µg/L at 0 min, 24.7 µg/L at 60 min, and 7.6 µg/L at 120 min), was apparent in patients with microadenomas. Such a change was not observed with macroadenomas (-1.9 µg/L at 0 min, 5.6 µg/L at 60 min, and 5.3 µg/L at 120 min). Patients with microadenomas appeared to have significantly lower ΔGHOS during the entire test time, with more a marked decline after 60 min compared with macroadenomas (Fig. 2B; P=0.042).
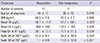
There were 11 macroadenomas responders in the OST. This means that SST in these macroadenomas substantially suppressed GH secretion. Based on this, additional analyses were performed according to the response of macroadenoma subjects to the OST (Table 3). The age and BMI of responders and non-responders did not show any significant differences. Basal GH levels, but not IGF-I, were significantly higher in non-responders (P=0.023 for basal GH). Non-responders also had a peak GH during the ITT and nadir GH during the OGTT and the OST that were significantly higher (Table 3). These differences in GH levels were observed during the entire two hours of each test (Fig. 3). Unlike ΔGHIO, ΔGHOS was different between responders and non-responders with borderline significance during the entire test time (Fig. 4).
DISCUSSION
The present study was designed to investigate the change in SST response according to the size of GH-producing pituitary tumors. Due to the lack of quantitative and direct methods for measuring SST, we estimated the change in SST by analyzing GH levels measured during the OGTT, the ITT, and the OST. It was found that, as the size of tumors increased, the effect of glucose on SST decreased. Macroadenomas that were non-responders to the OST were more likely to contain a portion of GH secretion exceeding the regulatory capacity of SST.
Under normal conditions, glucose loading during the OGTT stimulates hypothalamic somatostatin release (5). This possibly accompanies physiologic enhancement of SST (6), and thus results in the suppression of GH secretion. In contrast, the ITT depletes the glucose essential for cell survival, and consequently various counter-regulatory hormones including GH are released to compensate for hypoglycemia (12). The maximum level of GH secretion that hypoglycemic states can physiologically elicit is therefore induced by the ITT, and it is reasonable to assume that the difference in GH levels between the ITT and the OGTT (ΔGHIO) indirectly represents the amplitude of GH under the effect of SST which changes according to the different glucose levels. Unfortunately, there have been no previous literature which introduced a direct method to measure SST, and it was inevitable to apply such an indirect method which used GH levels during various tests.
GH-producing pituitary adenomas in acromegalic patients, especially with macroadenomas in general possess a greater capacity for autonomous GH secretion and greater basal GH secretions (7). Obviously, it is shown in higher GH levels in macroadenomas (Fig. 1B). However, the overall GH levels during the ITT did not differ (Fig. 1A). These findings suggest that although larger tumors produce greater GH secretion, the SST response to hypoglycemia does not differ regardless of the tumor size in order to alleviate hypoglycemic conditions. In contrast, glucose loading during the OGTT enhances the SST response to inhibit GH secretion, and the degree of inhibition varies depending upon the tumor size. This finding is consistent with a previous study by Mancini et al. which reported that the SST response induced by glucose possibly produced different suppressive effects on GH secretion depending on tumor size (13). BMI did not significantly differ between two groups (Table 2); thus, the possible influence of BMI upon GH secretion and action can be excluded.
This idea is further supported by our findings that ΔGHIO, defined as the amplitude of GH regulated by the change in glucose level, was non-significantly larger in microadenomas than macroadenomas; and ΔGHIO did not fluctuate in macroadenomas during the two hours of the tests (Fig. 2A). This means the amplitude of GH under the effect of SST was smaller in macroadenomas than microadenomas. It is because SST in macroadenomas is unable to suppress GH secretion effectively due to their autonomous secretory capacity which surpasses the regulation by SST. On the other hand, a pituitary gland with a microadenoma would still possess a fair portion of normal tissue where a hyperglycemia-induced SST response can exert its effect, though not enough to suppress GH production below 1 µg/L. Thus, GH secretion in microadenomas should partially remain under the physiologic regulation of glucose, as seen by their higher ΔGHIO values compared with macroadenomas.
Since glucose affects hypothalamic somatostatin release possibly through physiologic processes such as cholinergic pathways (6), it may be regarded as indirectly controlling GH secretion. In contrast, octreotide binds to somatostatin receptors (SSTRs) and suppresses GH secretion (14), and thus could be regarded as exerting direct regulations on GH secretion with a much stronger suppressive effect than indirect mechanisms (glucose). In this sense, GH levels during the OST may represent the minimal capacity for GH secretion due to the direct suppressive effect of somatostatin analogues. Therefore, ΔGHOS, defined as the difference in GH levels between the OGTT and the OST, could be interpreted as a portion of GH secretion which exceeds regulation by the hyperglycemia-induced SST response. Our data demonstrated that overall ΔGHOS values between those with macroadenomas and microadenoma remained significantly difference over the two hours of the tests (Fig. 2B), and thus macroadenomas are expected to contain a portion of GH secretion which surpasses the regulation by SST. This may be one of the reasons for higher basal GH levels and less suppression during the OGTT in macroadenomas compared with microadenomas.
In our study, 50% of macroadenoma patients were classified as responders to the OST, demonstrating sufficient suppression of GH secretion following an octreotide injection (Table 1). Basal GH levels were significantly different between responders and non-responders, whereas IGF-I levels were similar between the two groups (Table 3). As shown in previous analyses (Table 2), serum IGF-I levels did not differ according to the responding pattern after the OST (Table 3). This finding suggests that continuous secretion of GH, regardless of tumor size, should play a crucial role in maintaining high serum IGF-I levels. BMI also did not show any significant difference in either group. Interestingly, GH levels during the ITT were significantly lower in responders than in non-responders (Table 3 and Fig. 3A). It is postulated that higher expression of SSTRs in responders as reported by Reubi and Landolt (15), may contribute to more sustained SST and consequently greater suppression of GH secretion in responders than non-responders. For the same reason, lower SST in non-responders may allow the GH secretion exceeding its regulatory capacity, as ΔGHOS between responders and non-responders was shown to be different with a near-significant trend (Fig. 4B).
This study has several limitations. It is well known that GHRH or GH-releasing peptides (GHRPs) such as ghrelin are also closely intertwined in the regulation of GH secretion (16, 17). However, GHRH and hypoglycemia may act on separate releasable pools of GH within the somatotroph population (5). GHRPs also stimulate GH production, but by virtue of enhancing pituitary GH gene expression, and thus apparently independent of somatostatin (18). On the other hand, hypoglycemia may inhibit somatostatin release and presumably the SST response which in turn augments GH secretion and consequently raise the glucose level (5, 12). Thus, the GH secretory response induced by a change in glucose levels may be more relevant to reflect the physiology of SST in tumoral status. GH-secreting cell subtypes (either densely or sparsely granulated somatotrophs) are another factors affecting to GH secretion but are not taken into account in this study. However, it was recently reported that different granulation patterns did not reflect distinct pathophysiological entities in GH-producing pituitary adenomas (19). It should be also noted that most of macroadenomas in our study were classified as grade IV-C, IV-D or IV-E according to Hardy classification (Table 1). Such macroadenomas are more likely to accompany the suprasellar extension which could cause the pituitary stalk compression and consequently reduce the effect of SST. There must be further studies which could investigate the relationship between SST and structural deformities in pituitary macroadenomas.
In conclusion, as the size of the pituitary tumor increases, the effect of glucose on SST appears to be attenuated. Macroadenomas that are non-responders to the OST possesses a portion of GH secretion exceeding the range of regulation by SST. This is the first study to examine changes in SST of GH-producing pituitary tumors by the additional manipulation of test results necessary to confirm the diagnosis of acromegaly. Though SST carries little weight in the diagnosis of acromegalic patients with GH-producing pituitary adenomas, its response in tumoral status is believed to demonstrate significant tumoral characteristics. The possible clinical utility of this method to evaluate SST will require additional studies with a larger number of patients.




 XML Download
XML Download