

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Metabolic syndrome is not a single disease but a conglomeration of risk factors for cardiovascular disease (CVD) including central obesity, elevated blood pressure, hypertriglyceridemia, low high-density lipoprotein (HDL) cholesterol, elevated fasting glucose, and insulin resistance. Subjects with metabolic syndrome are at increased risk for type 2 diabetes mellitus and cardiovascular disease (1). Korea has experienced a rapid increase in the prevalence of metabolic syndrome during the 2000s, partly due to increasing adoption of a western lifestyle (2). Given the high prevalence of metabolic syndrome and its potential consequences, it is crucial to identify its predictors and mechanisms in longitudinal studies.
It is well recognized that visceral adipose tissue (VAT) plays a major role in the development of metabolic syndrome (3). Measurement of waist circumference is widely used as an indicator and screening tool of VAT in population-based studies, but it does not distinguish between accumulations of VAT and subcutaneous abdominal fat. Imaging modalities, particularly computed tomography (CT) and magnetic resonance imaging (MRI), have been used to allow the accurate measurement of visceral and subcutaneous abdominal fat because they clearly distinguish VAT from other tissues (4). However, these imaging studies are expensive and are not suitable for routine clinical practice due to the risk of ionizing radiation exposure.
Epicardial adipose tissue (EAT) thickness measured by echocardiography was proposed as a novel imaging indicator of VAT. It was well correlated with VAT assessed by MRI, which is the gold standard for measurements of VAT (5). Recent studies have suggested that increased EAT is positively associated with the risk of metabolic syndrome (5-7), but little is known about measurement of EAT by echocardiography as a predictor of metabolic syndrome in population based longitudinal studies.
Thus, we studied the prospective association of EAT thickness measured by echocardiography with the risk of incident metabolic syndrome and its components in a community-based middle-aged population. We hypothesized that EAT thickness measured by echocardiography would be a positive predictor of progression to metabolic syndrome.
MATERIALS AND METHODS
Study population
We used data from the Korean Genome and Epidemiology Study on Atherosclerosis Risk of Rural Areas in the Korean General Population (KoGES-ARIRANG), a population-based prospective cohort study, to assess the prevalence, incidence and risk factors for chronic degenerative disorders such as hypertension, diabetes, osteoporosis, and cardiovascular disease (8-10). KoGES-ARIRANG invited adults aged 40-70 yr in rural areas of Wonju and Pyeongchang in Korea where demographic shifts are infrequent and high long-term follow up rates are expected.
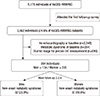
The baseline survey, carried out from November 2005 to January 2008, included 5,178 adults (2,127 men and 3,051 women) aged 40 to 70 yr. All study subjects were invited to the first follow-up survey (April 2008 to January 2011) and 3,862 (74.6%) attended. Then we excluded 2,548 subjects who did not carry out baseline echocardiography, 696 subjects who were unavailable for EAT measurements and 264 subjects with metabolic syndrome at baseline. The final sample size for the present analysis was 354 subjects (134 men and 220 women) (Fig. 1).
Data collection
At baseline and follow-up examinations, study subjects completed a standardized medical history and lifestyle questionnaire and underwent a comprehensive health examination according to standard procedures. Body weight and height were measured while subjects wore light indoor clothing without shoes. Waist circumference was measured in a horizontal plane, midway between the inferior margin of the ribs and the superior border of the iliac crest using a tape measure (SECA-200, SECA, Hamburg, Germany). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured twice in the right arm using a standard mercury sphygmomanometer (Baumanometer, Copiague, NY, USA). The mean of the two blood pressure readings was used for data analyses. Smoking status was determined based on self-report. Nonsmokers were defined as subjects who had smoked <100 cigarettes (<5 packs of cigarettes) in their lifetime. Current smokers were defined as subjects who had smoked ≥100 cigarettes in their lifetime and who reported that they were "currently smoking" in the questionnaire. Former smokers were defined as subjects who had smoked ≥100 cigarettes in their lifetime but who reported that they "abstain from smoking" in the questionnaire. Subjects who answered yes to the question: 'Do you perform physical exercise regularly enough to make you sweat?' were assigned to the regular exercise group. Dietary data were obtained using a semi-quantitative food-frequency questionnaire that listed 103 food items generally consumed by Koreans (11). Postmenopausal women were defined as subjects who had not experienced a menstrual period for at least 12 continuous months (12).
A venous blood sample was drawn from study participants after fasting for >12 hr or overnight. Fasting glucose was determined by a glucose oxidase-based assay. Fasting insulin was determined by a double-antibody radioimmunoassay (Biosource, Nivelles, Belgium). Serum concentrations of low-density lipoprotein (LDL) cholesterol, high-density lipoprotein cholesterol (HDL) and triglycerides (TG) were determined by enzymatic methods (Advia 1650, Siemens, Tarrytown, NY, USA). High sensitivity C-reactive protein (hsCRP) was measured by the Denka Seiken (Tokyo, Japan) assay, which has been validated against the Dade Behring method. Insulin resistance was calculated using the homeostasis model assessment of insulin resistance (HOMA-IR) model, following the formula: fasting insulin (µIU/mL)×fasting plasma glucose (mg/dL)/405.
Measurement of epicardial adipose tissue (EAT) thickness
EAT thickness was measured using echocardiography (Vivid-7; General Electric-Vingmed, Milwaukee, WI, USA) and it was defined as an echo-lucent area between the free wall of the right ventricle and the visceral layer of the pericardium at end-systole in the parasternal long axis view. As proposed by Iacobellis et al. (13), EAT thickness was measured on the free wall of the right ventricle to be perpendicular to the aortic annulus at end-systole. Each echocardiography image was reviewed by two experienced readers who were blind to the clinical data of study subjects. The inter-reader correlation coefficient was 0.992 (95% confidence interval [CI], 0.970-0.998), indicating very low inter-reader variability.
Endpoint definition
The study endpoint is the development of metabolic syndrome at the follow-up visit, defined following the harmonized definition for metabolic syndrome (14) as the presence of at least three of the following criteria: 1) Abdominal obesity, defined as a waist circumference ≥90 cm for men or ≥85 cm for women (following Korean-specific cutoffs for abdominal obesity defined by the Korean Society of Obesity) (15); 2) Hypertriglyceridemia, defined as a serum TG concentration ≥150 mg/dL (1.69 mM/L); 3) Low HDL cholesterol, defined as a serum HDL cholesterol concentration <40 mg/dL (1.04 mM/L) for men or <50 mg/dL (1.29 mM/L) for women; 4) High blood pressure, defined as a SBP ≥130 mmHg or a DBP ≥85 mmHg, or treatment with antihypertensive agents; 5) High fasting glucose, defined as a fasting serum glucose ≥100 mg/dL or previously diagnosed type 2 diabetes.
Statistical analysis
The data are expressed as means, medians, and frequencies. Either a t-test or Mann-Whitney U test was conducted to compare characteristics of subjects with and without metabolic syndrome for continuous variables. And the chi-square test was performed for categorical variables. All analyses were performed separately by gender. Multivariate logistic regression was used to assess the independent association of baseline epicardial adipose tissue with incident metabolic syndrome. We adjusted for age (continuous variable), body mass index (continuous variable), smoking (current/former/never), regular exercise (yes/no), daily energy intake (continuous variable), hsCRP (continuous variable), and HOMA-IR (continuous variable). The upper quartiles of EAT were used as cut-off points (2.55 mm for men, 2.35 mm for women) of increased EAT. The results of logistic regression were expressed as odds ratios (ORs) with 95% confidence intervals (CI). Area under the receiver operating characteristic (ROC) curve analyses were used to describe the ability of epicardial adipose tissue to predict new-onset metabolic syndrome in men and women. All analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC, USA). P values of <0.05 were considered to be statistically significant.
RESULTS
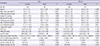
After an average of 2.2 yr of follow-up, 32 men (23.9%) and 37 women (16.8%) developed metabolic syndrome. Baseline body mass index, waist circumference, systolic blood pressure, diastolic blood pressure and the number of metabolic syndrome components were significantly higher in men and women who developed metabolic syndrome compared to those who did not (Table 1). There were no significant differences in LDL cholesterol, triglyceride, current smoking, and regular exercise between the groups. Median EAT thickness at baseline were significantly higher in men who developed metabolic syndrome compared to men who did not (1.52 vs 2.37 mm, P<0.001), but not in women (1.51 vs 1.73 mm, P=0.186).
In multivariate adjusted models (Table 2), the risk of incident metabolic syndrome increased in subjects with the highest quartile of EAT thickness (≥2.47 mm), compared to those in the three lower quartiles (OR, 1.99; 95% CI, 1.05-3.74). The corresponding ORs (95% CIs) for developing high waist circumference, low HDL cholesterol, high TG, high blood pressure, high blood glucose were 2.13 (1.08-4.22), 0.69 (0.40-1.17), 1.26 (0.67-2.39), 1.64 (0.95-2.83), and 1.13 (0.56-2.27), respectively.
When analyses were performed separately by gender, the OR for incident metabolic syndrome comparing men with the highest quartile of EAT thickness to others (EAT thickness ≥2.55 mm vs <2.55 mm) was 3.09 (95% CI, 1.11-8.66). The corresponding ORs (95% CIs) for developing high waist circumference, low HDL cholesterol, high triglycerides, high blood pressure, and high blood glucose were 2.34 (0.68-8.03), 0.88 (0.35-2.20), 2.18 (0.83-5.74), 2.42 (0.93-6.26), and 1.10 (0.44-2.79), respectively. When comparing men in the highest quartile to those in the lowest quartile of EAT thickness, the OR for incident metabolic syndrome was 8.96 (95% CI, 1.70-47.11) (Supplementary Table 1).
The OR for developing metabolic syndrome comparing women in the highest quartile of EAT thickness to those in the three lower quartiles (EAT thickness ≥2.35 mm vs <2.35 mm) was 1.25 (95% CI, 0.54-2.90). No significant relationships were found in predicting the development of each component of metabolic syndrome in women. When comparing women in the highest quartile to those in the lowest quartile of EAT thickness, the OR for incident metabolic syndrome was 1.23 (95% CI, 0.42-3.57) (Supplementary Table 1).
The areas under the ROC curve to predict incident metabolic syndrome using EAT thickness results were 0.706 (95% CI, 0.602-0.810) in men and 0.567 (95% CI, 0.470-0.664) in women (Fig. 2). We estimated that the best cut-off value for the EAT thickness to predict incident metabolic syndrome was 1.95 mm for men and 1.69 mm for women.
DISCUSSION
In this prospective cohort study in an Asian population, EAT thickness measured by echocardiography was a predictor of incident metabolic syndrome in men, but not in women. A recent meta-analysis showed a significant relationship between EAT and metabolic syndrome (16); however, the role of EAT in predicting incident metabolic syndrome has not been evaluated in a prospective longitudinal study. To our knowledge, the present study is the first prospective study to demonstrate that the increased EAT thickness measured by echocardiography is an independent predictor of incident metabolic syndrome in men.
Visceral adiposity is one of the key mechanisms in development of metabolic syndrome. Although waist circumference is a convenient method for estimation of visceral adiposity, it is limited by the inability to distinguish visceral fat from abdominal subcutaneous fat. A previous study has demonstrated that echocardiographic EAT thickness is a better indicator of visceral adiposity than measuring waist circumference (6). Furthermore, the measurement of echocardiographic EAT is more convenient than other imaging modalities such as CT or MRI. Thus, the echocardiographic measurement of EAT could be considered a useful tool for prediction of visceral adiposity.
EAT is true visceral fat which originates from brown adipose tissue during embryogenesis. It surrounds the myocardium and is not divided by fascia (17). EAT is also an active endocrinometabolic organ, not just a form of fat storage. It has been found to produce several bioactive molecules that indicate insulin resistance and systemic inflammation (17-19). Previous cross-sectional studies show that increased EAT thickness measured by echocardiography is also associated with insulin resistance (20) and obesity (5-7). Weight reduction in obesity is also associated with decreased EAT thickness (21, 22). These properties of EAT could partly explain why increased EAT thickness is related to increased prevalence and incidence of metabolic syndrome in men.
In the present study, increased EAT thickness was significantly associated with incident metabolic syndrome in men, but not in women. Although we could not establish a clear reason for this gender difference, we suggest several plausible explanations. First, we need to note that high EAT thickness is highly predictive of high waist circumference, high TG and high blood pressure in men (OR>2.00), but high EAT thickness is only predictive of high waist circumference in women, even though these related ORs are not statistically significant. This difference of impact of the EAT may explain gender differences in the incidence of metabolic syndrome. Second, menopausal status could influence the gender difference. The prevalence of metabolic syndrome increases significantly with menopause in women. Estrogen deficiency is believed to be one of the culprits for this phenomenon (23). Estrogen deficiency may play a more influential role than EAT in the development of metabolic syndrome in postmenopausal women. The confounding effect of postmenopausal state may be one explanation for gender differences. Additionally, we performed an analysis in pre-menopausal and postmenopausal women separately. The association between EAT thickness and incident metabolic syndrome was insignificant in both groups (Supplementary Table 2). However, the majority of female subjects in the present study were postmenopausal (59.6% at baseline and 69.0% at follow-up) and the mean age of female subjects was above 52 yr. Many pre-menopausal women in the present study may be transitioning to menopause. In a recent cross-sectional study targeting 650 recently menopausal women, high EAT volume measured by computed tomography did not show a significant relationship to serum insulin level in age, race-ethnicity, education level, smoking status, alcohol intake, physical activity level, study center and BMI. The study used an adjusted model that is similar to the model used in the present study (24). Further research is required to understand gender differences in the association between EAT and metabolic syndrome.
Besides EAT, many factors could influence the development of metabolic syndrome such as smoking, diet, exercise or medications with antihypertensive or lipid-lowering properties. In the present study, 52 (14.7%) and 17 (4.8%) of the total study population was taking antihypertensive medication and lipid-lowering medication, respectively. After exclusion of subjects with antihypertensive or lipid-lowering medication, a similar association was observed between EAT thickness and the risk of incident metabolic syndrome (Supplementary Table 3).
Several limitations of our study should also be considered. First, we were able to use echocardiography to measure EAT thickness in only 24% of the whole study cohort. However, we found similar baseline demographics between study subjects and the rest of cohort population (Supplementary Table 4). Second, the study included only middle-aged and elderly Koreans living in rural areas, and may not be generalizable to other populations, such as urban residents, groups with different lifestyles or different incidence trends of metabolic syndrome, and those who are younger. However, EAT thickness measured by echocardiography has been associated with metabolic risk factors in other races and ethnicities, suggesting that the associations that we observed also could apply to other settings. Third, the follow-up period was only 2.2 yr, and we could not evaluate whether the association between EAT thickness and incident metabolic syndrome would persist in longer follow-up.
In conclusion, increased EAT thickness is an independent predictor for incident metabolic syndrome in men. Echocardiographic EAT thickness may be a novel imaging tool to predict the development of metabolic syndrome.


 XML Download
XML Download